
Abstract
Background:
Moxibustion has been used in the treatment and prevention of obesity. However, there has been no systematic review or meta-analysis conducted on the use of moxibustion on obesity treatment. This study aimed to evaluate the role of moxibustion in the treatment of obesity.
Methods:
The Cochrane Central Register of Controlled Trials, EMBASE, and MEDLINE/PubMed databases were searched to identify all randomized controlled trials (RCTs) that evaluated the effect of moxibustion on obesity. The primary outcome was body weight. The secondary outcomes were the body mass index (BMI), waist circumference (WC), hip circumference (HC), and waist-to-hip ratio (WHR). The risk of bias assessment and meta-analysis were conducted using the Cochrane Collaboration tool.
Results:
Eleven RCTs involving 761 participants were included in this systematic review and meta-analysis. Other interventions that were included in the analyses were manual acupuncture, electroacupuncture, embedding therapy, herbal medicine, and diet control. Moxibustion combined with other interventions resulted in a significant improvement in body weight reduction (mean difference [MD] −3.32, 95% confidence interval [CI: −4.25 to −2.38]; I 2 = 17%), BMI (MD −1.51, 95% CI [−1.88 to −1.14]; I 2 = 76%), and WC (MD −2.82, 95% CI [−3.50 to −2.13]; I 2 = 75%), but did not improve HC (MD −2.05, 95% CI [−4.21 to 0.11]; I 2 = 0%) or WHR (MD −0.01, 95% CI [−0.03 to 0.01]; I 2 = 57%).
Conclusions:
Moxibustion can be used with other interventions to improve body weight, BMI, and WC in people with obesity. However, the conclusions of this review should be cautiously applied to clinical practice because most of the included studies had a high or unclear risk of bias.
Introduction
Obesity is a serious health problem that is an imbalance between energy consumption and expenditure. The prevalence of obesity has increased rapidly in the past few decades. 1 Obesity is a risk factor for various chronic diseases, such as diabetes, hyperlipidemia, hypertension, heart disease, and cancer, 2 as well as for psychological problems, such as decreased self-esteem, difficulties in social life, and eating disorders. 3 Obesity has also been shown to reduce overall life expectancy. 4
Current treatment options for obesity include diet modification, exercise, 5 pharmacologic agents, herbal medicines, 6 and acupuncture. 7 Moxibustion is a component of Traditional Chinese Medicine (TCM). It consists of the combustion of dried moxa or mugwort (Artemisia argyi) directly or near a patient's skin and acts by stimulating the surface of the human body. 8,9 Traditionally, moxibustion has been used for various diseases, including musculoskeletal and endocrine system disorders, and it has recently being used to treat obesity usually in combination with other therapeutic methods. 10
Several studies on the effects of combined treatment of moxibustion and acupuncture on obesity reported improvements in weight and body mass index (BMI), 11,12 and regulation of molecular mechanism concerned with obesity. 13 In vivo and in vitro studies suggested that application of moxibustion could be a promising strategy against obesity. 14 –17 However, there were a number of methodological differences between studies, and many only included a small number of participants.
Furthermore, there have been no systematic reviews or meta-analyses of moxibustion combined therapy for obesity. Study by Yin et al. 18 reported efficacy of acupuncture and moxibustion therapy for simple obesity in adults, but none of the included studies have reported moxibustion for its intervention. Therefore, a systematic review and meta-analysis of randomized controlled trials (RCTs) were conducted on moxibustion for obesity.
Materials and Methods
The protocol of this systematic review was uploaded and registered with the Open Science Framework (osf.io/ntkdf). 19 The protocol follows the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines. 20 See PRISMA checklist for the details.
Criteria for the inclusion of studies
Types of studies
RCTs were selected and analyzed in this systematic review. Quasi-RCTs or crossover studies were not included. There were no language restrictions.
Participants
Patients diagnosed with obesity whose BMI ≥25 kg/m2 were included with no restrictions regarding age or sex.
Interventions
The experimental groups were those who received moxibustion. Studies that included the use of materials to protect the skin from direct contact with the heat were included. Thermal needle therapy was not included as an intervention in this study. Studies with moxibustion combined with other interventions, those with a control group who received any intervention other than moxibustion, and studies where the control group only received a placebo were all included. Other interventions or treatments included were lifestyle modifications, TCM, and conventional drugs.
Outcome measurements
The primary outcome was body weight. The secondary outcomes included the BMI, waist circumference (WC), WHR (waist-to-hip ratio), and hip circumference (HC).
Search strategy
Electronic data
The Cochrane Central Register of Controlled Trials, EMBASE, and MEDLINE/PubMed databases were searched and screened. One Japanese database (Citation Information by the National Institute of Informatics), one Chinese database (Chinese National Knowledge Infrastructure), and three Korean databases (Oriental Medicine Advanced Searching Integrated System, KoreaMed, and ScienceON) were also systematically searched from their inception to March 2021. The search results for PubMed are presented in Table 1.
Characteristics of the Included Studies
AC, acupuncture; ACE, acupuncture embedding therapy; BMI, body mass index; BW, body weight; C, control group; EA, electroacupuncture; ER, effective rate; HC, hip circumference; HM, herbal medicine; I, intervention group; NR, not reported; WC, waist circumference; WHR, waist-to-hip ratio.
Other resources
The reference lists of the included studies were scanned to search for other related articles. A manual search of offline-only data was also conducted.
Data collection and analysis
Study selection
Two researchers searched the databases and other sources individually, using search instructions. These two researchers independently selected the articles by reviewing the studies against the inclusion and exclusion criteria of this study. Any disagreements between these two researchers were resolved by a third reviewer. The flowchart of the selection process is shown in Figure 1.

Flow diagram of the selection process.
Data extraction and management
Data were extracted by the reviewers on a previously produced spreadsheet in Microsoft Excel. The variables extracted and recorded in Microsoft Excel were the author names, number of patients in the intervention and comparison groups, intervention details, duration and frequency of treatment, units and time point of the measurements, results, and the side effects. If the data were not clear or the contents of the two datasheets differed, the third reviewer was consulted.
Assessment of the risk of bias and quality of the included studies
Two independent reviewers evaluated the risk of bias in seven domains using a tool developed by the Cochrane Collaboration group. The domains for this assessment were the blinding of participants and staff, allocation concealment, random sequence generation, blinding of the outcome assessment, incomplete outcome data, reporting of selective outcomes, and other sources of bias. Each domain could be rated as “high risk,” “low risk,” or “unclear risk.” When two reviewers disagreed on a decision regarding a category, the opinions of the other reviewers were considered.
Assessment of the effect of treatment
Continuous data on the outcomes are represented by the mean difference (MD) with 95% confidence intervals (CIs).
Management of missing data
If there were any missing data, the corresponding author of the study was contacted by e-mail to try and obtain the required data. If the author refused or did not respond to the request, the missing data were not included in the analysis.
Data synthesis
The researchers synthesized the data and conducted a meta-analysis using the software distributed by Cochrane Collaboration-Review Manager (RevMan; 2014; version 5.3; Copenhagen). In studies with high heterogeneity (I 2 > 50%), a random-effects model was used, whereas in the case of I 2 < 50%, a fixed-effects model was used. Subgroup analysis was conducted when the results were highly heterogeneous, and it was deemed reasonable to divide the entire group according to a specific category.
Subgroup analysis
The criteria for the subgroup analysis were as follows: Types of interventions combined with moxibustion in the experimental groups Intervention period Time point of the follow-up.
Ethics and dissemination
This study did not require approval from the institutional review committee because it evaluated the completed and published studies.
Results
Included studies
The search and selection procedures were performed according to the PRISMA guidelines, as shown in Figure 1. Initially, a total of 418 articles were identified. Two authors reviewed the articles. Of these, 197 duplicates were excluded. The titles and abstracts of the remaining articles were further examined for eligibility. Twenty-two studies were excluded because the intervention was a warm needle, the intervention was not executed properly, the primary subject of study was not obesity, studies were duplicate cases, retracted studies, and the article was a protocol. A total of 11 studies were finally included in analyses.
Research characteristics
The characteristics of the included studies are given in Table 1. The studies were published between 2009 and 2019. The sample sizes ranged from 30 to 120. Only one 21 of the studies was written in English, whereas the others 22 –31 were written in Chinese. Of the included studies, 1022–31 were conducted in China and 121 in Mexico. All the patients in the study were obese. Various treatments, combined with moxibustion, were administered to the experimental groups.
The control group interventions included electroacupuncture, acupuncture, embedding therapy, herbal medicine, and diet control. None of the controls had moxibustion for intervention. The main outcome was body weight. The secondary outcomes were BMI, WC, HC, and WHR. Only two studies 22,26 reported adverse events, such as burns, dizziness, or mild bleeding.
Risk of bias
The risk of bias is shown in Figure 2. Four studies 21,22,26,31 had a low risk of bias due to a random sequence generation process. In another five studies, 23,25,27 –29 the sequence generation procedure was unclear. In the remaining two studies, 24 –30 the sequence generation had a nonrandom component and, therefore, was deemed to have a high risk of bias. Most of the studies 21 –23,25,27 –31 did not report allocation concealment. Of those that did, one study 26 had a low risk of bias, while the other 24 had a high risk of bias. The blinding of participants and personnel was not ensured or reported uniformly. Only one study 26 specifically mentioned blinding of the outcome assessment. This study was deemed to have a low risk of bias.
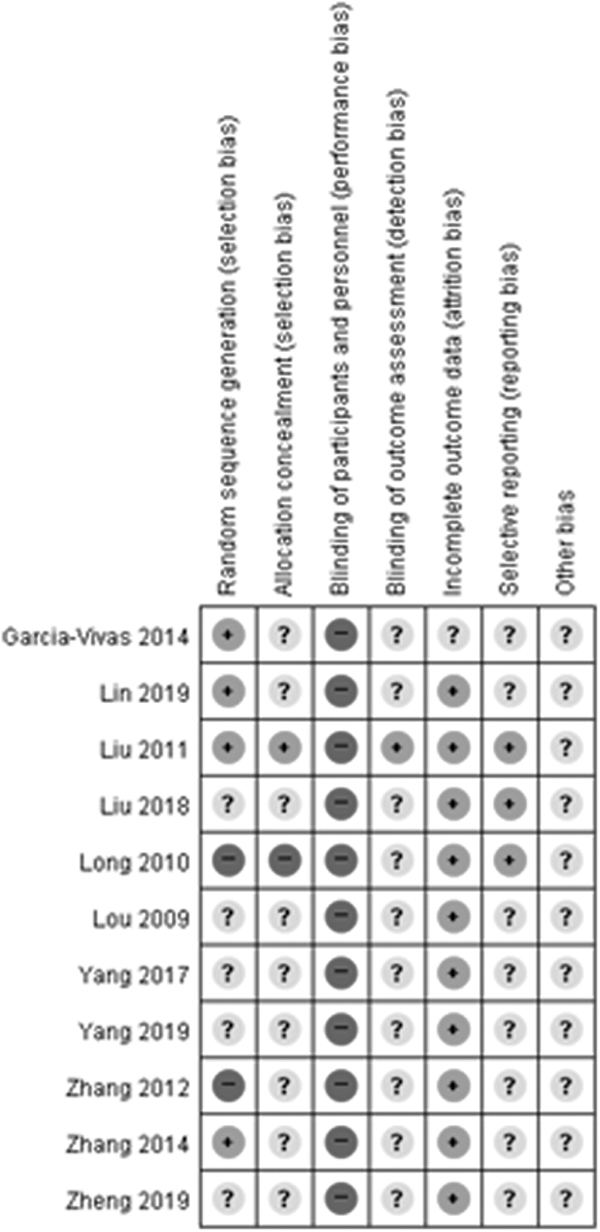
Risk of bias graph.
Ten studies 22 –31 had a low risk of bias due to incomplete outcome data, and one study 21 did not discuss why there was incomplete outcome data. In eight studies, 21 –23,25,28 –31 the selective reporting could not be clearly determined since there was ambiguity, whereas the other three studies 24,26,27 did selective reporting clearly. All the studies were evaluated for other possible biases, which were found to be absent.
Effects of intervention
This meta-analysis included 11 studies involving 761 participants. The meta-analysis was based on five results: body weight, BMI, WC, HC, and WHR.
Primary outcome
In the meta-analysis of nine studies, involving 625 subjects, the combined moxibustion group showed a more significant improvement in body weight than the control group (MD −3.32, 95% CI [−4.25 to −2.38]; I 2 = 17%) (Fig. 3). The subgroup analysis was based on the type of intervention combined with moxibustion.
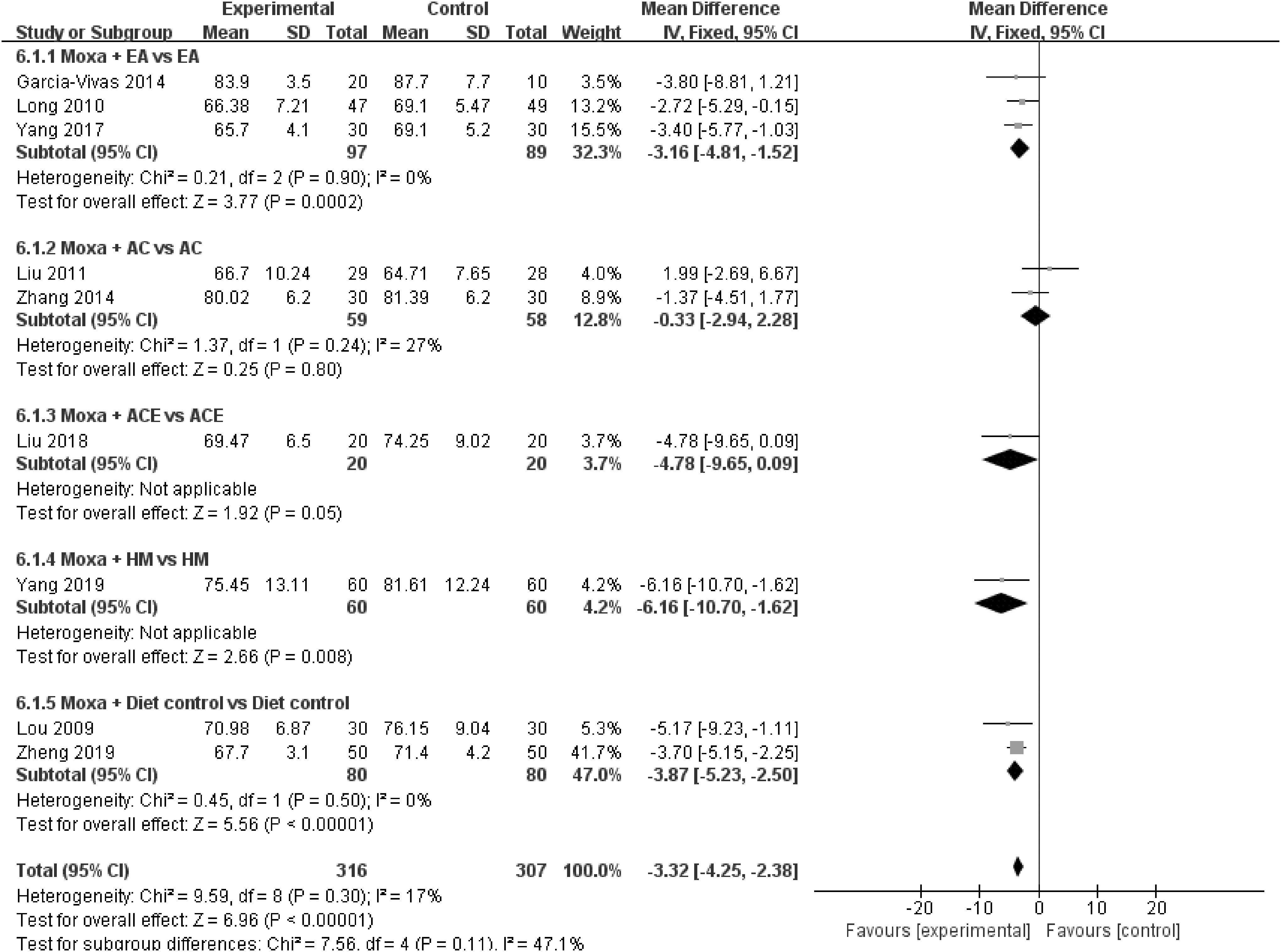
Body weight (subgroup analyzed by treatment type of interventions combined with moxibustion). AC, acupuncture; ACE, acupuncture embedding therapy; EA, electroacupuncture; HM, herbal medicine.
All the treatment types combined with moxibustion, including electroacupuncture (MD −3.16, 95% CI [−4.81 to −1.52]; I 2 = 0%), herbal medicine (MD −6.16, 95% CI [−10.70 to −1.62]; I 2 = not applicable), and diet control (MD −3.87, 95% CI [−5.23 to −2.50]; I 2 = 0%), had significantly better body weight results than the control group. There was no significant improvement seen in the embedding therapy plus moxibustion studies (MD −4.78, 95% CI [−9.65 to 0.09]; I 2 = not applicable) and the acupuncture plus moxibustion studies (MD −0.33, 95% CI [−2.94 to 2.28]; I 2 = 27%) (Fig. 3).
Secondary outcomes
Body mass index
In the meta-analysis of 10 studies involving 703 subjects, the combined moxibustion group showed a more significant improvement in BMI than the control group (MD −1.51, 95% CI [−1.88 to −1.14]; I 2 = 76%) (Fig. 4). The subgroup analysis was based on the type of intervention combined with moxibustion.
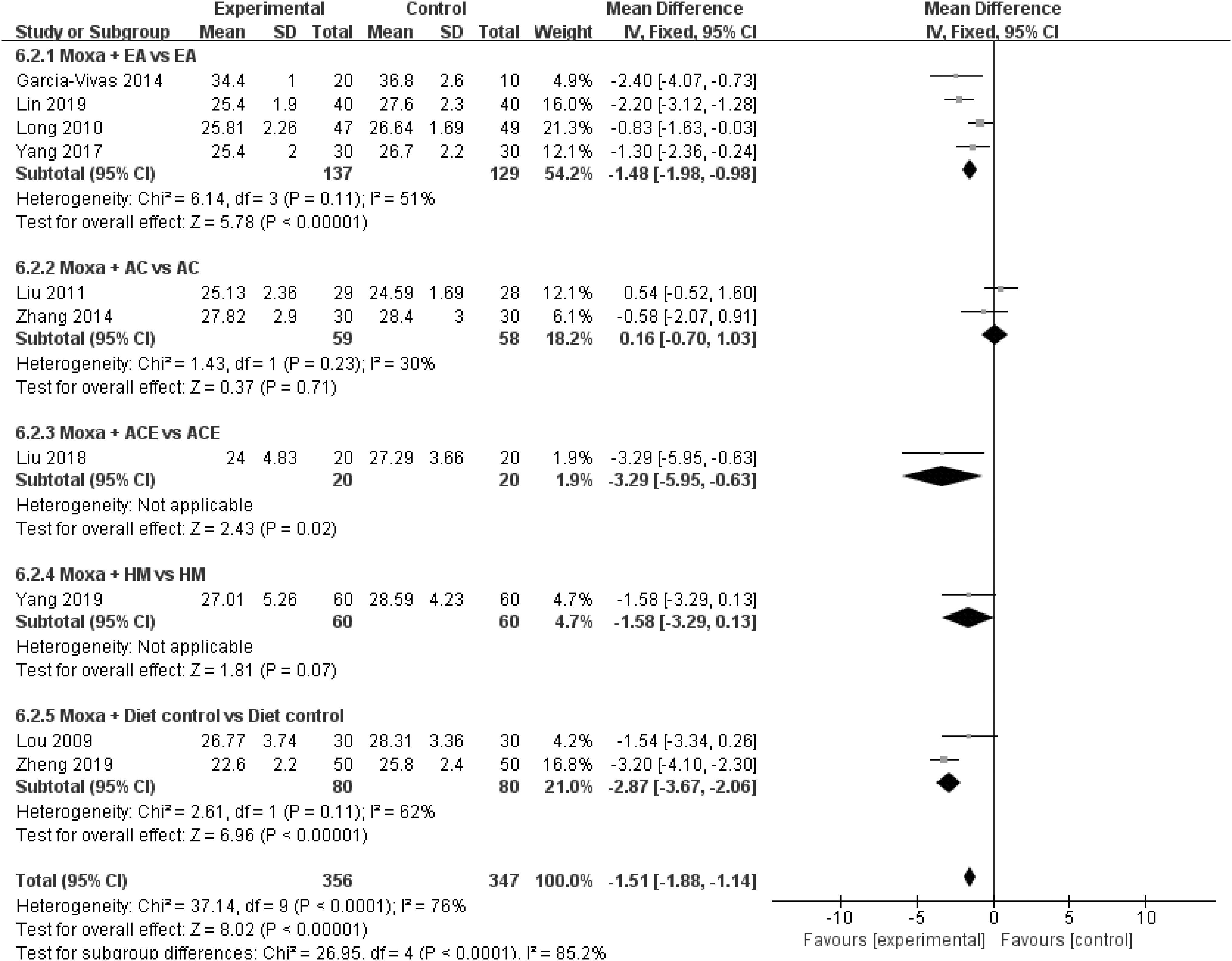
BMI (subgroup analyzed by treatment type of interventions combined with moxibustion). AC, acupuncture; ACE, acupuncture embedding therapy; BMI, body mass index; EA, electroacupuncture; HM, herbal medicine.
All the treatment types combined with moxibustion, including electroacupuncture (MD −1.48, 95% CI [−1.98 to −0.98]; I 2 = 51%), embedding therapy (MD −3.29, 95% CI [−5.95 to −0.63]; I 2 = not applicable), and diet control (MD −2.87, 95% CI [−3.67 to −2.06]; I 2 = 62%), had significantly better BMI results than the control group. There was no significant improvement seen in the acupuncture plus moxibustion studies (MD 0.15, 95% CI [−0.70 to 1.03]; I 2 = 30%) and herbal medicine plus moxibustion studies (MD −1.58, 95% CI [−3.29 to 0.13]; I 2 = not applicable) (Fig. 4).
Waist circumference
In the meta-analysis of nine studies involving 583 subjects, the combined moxibustion group showed a more significant improvement in WC than the control group (MD −2.82, 95% CI [−3.50 to −2.13]; I 2 = 75%) (Fig. 5). The subgroup analysis was based on the type of intervention combined with moxibustion. In combination with electroacupuncture (MD −1.54, 95% CI [−2.46 to −0.63]; I 2 = 47%) and diet control (MD −5.01, 95% CI [−6.18 to −3.84]; I 2 = 44%), moxibustion was found to result in a significantly better WC than the control group.

Waist circumference (subgroup analyzed by treatment type of interventions combined with moxibustion). AC, acupuncture; ACE, acupuncture embedding therapy; EA, electroacupuncture.
However, in the analysis of moxibustion combined with acupuncture (MD −1.85, 95% CI [−4.30 to 0.60]; I 2 = 70%) and embedding therapy (MD −3.99, 95% CI [−8.49 to 0.51]; I 2 = not applicable), the experimental group did not show significant improvement (Fig. 5).
Hip circumference
In the meta-analysis of four studies involving 187 subjects, there was no significant improvement in any of the experimental groups. There was no comparative benefit overall (MD −2.05 95% CI [−4.21 to 0.11]; I 2 = 0%) or individually in those treated with moxibustion plus electroacupuncture (MD −0.90 95% CI [−5.86 to 4.06]; I 2 = not applicable), moxibustion plus acupuncture (MD −3.46 95% CI [−10.67 to 3.75]; I 2 = not applicable), moxibustion plus embedding therapy (MD −1.99, 95% CI [−5.96 to 1.98]; I 2 = not applicable), or diet control (MD −2.31, 95% CI [−5.62 to 1.00]; I 2 = not applicable) (Fig. 6).
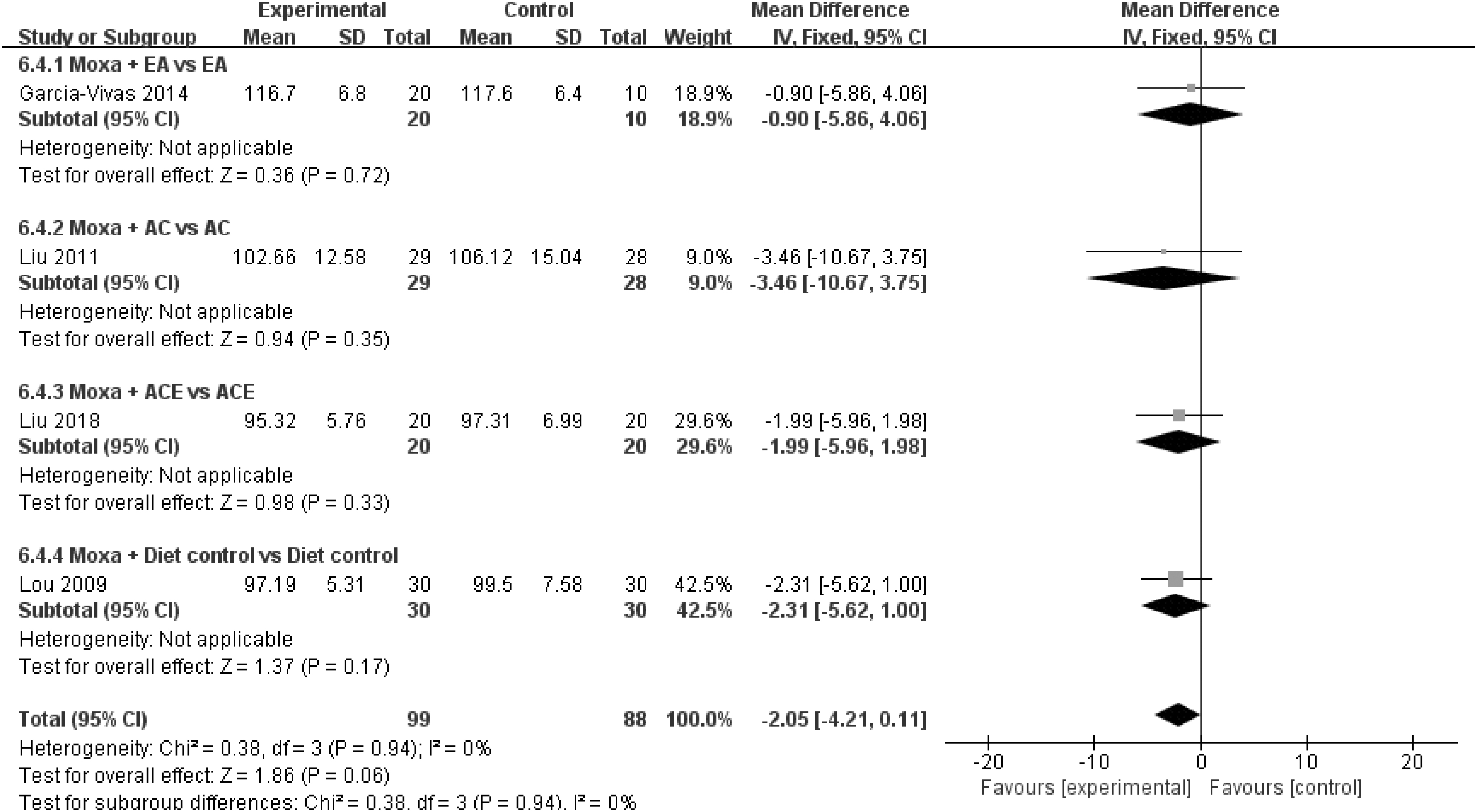
Hip circumference (subgroup analyzed by treatment type of interventions combined with moxibustion). AC, acupuncture; ACE, acupuncture embedding therapy; EA, electroacupuncture.
Waist-to-hip ratio
In the meta-analysis of seven studies involving 423 subjects, there was no significant improvement in the experimental group. There was no overall benefit of combining moxibustion with any of the other modalities (MD −0.01, 95% CI [−0.03 to 0.01]; I 2 = 57%). The subgroup analysis according to the design of the comparison group was conducted as follows.
The combined moxibustion groups did not show significant improvement compared with the control groups: moxibustion plus electroacupuncture (MD −0.02, 95% CI [−0.04 to −0.00]; I 2 = 65%), moxibustion plus acupuncture (MD 0.03, 95% CI [−0.01 to 0.07]; I 2 = not applicable), moxibustion plus embedding therapy (MD −0.04, 95% CI [−0.28 to 0.20]; I 2 = not applicable), and diet control (MD −0.04, 95% CI [−0.18 to 0.10]; I 2 = not applicable) (Fig. 7).
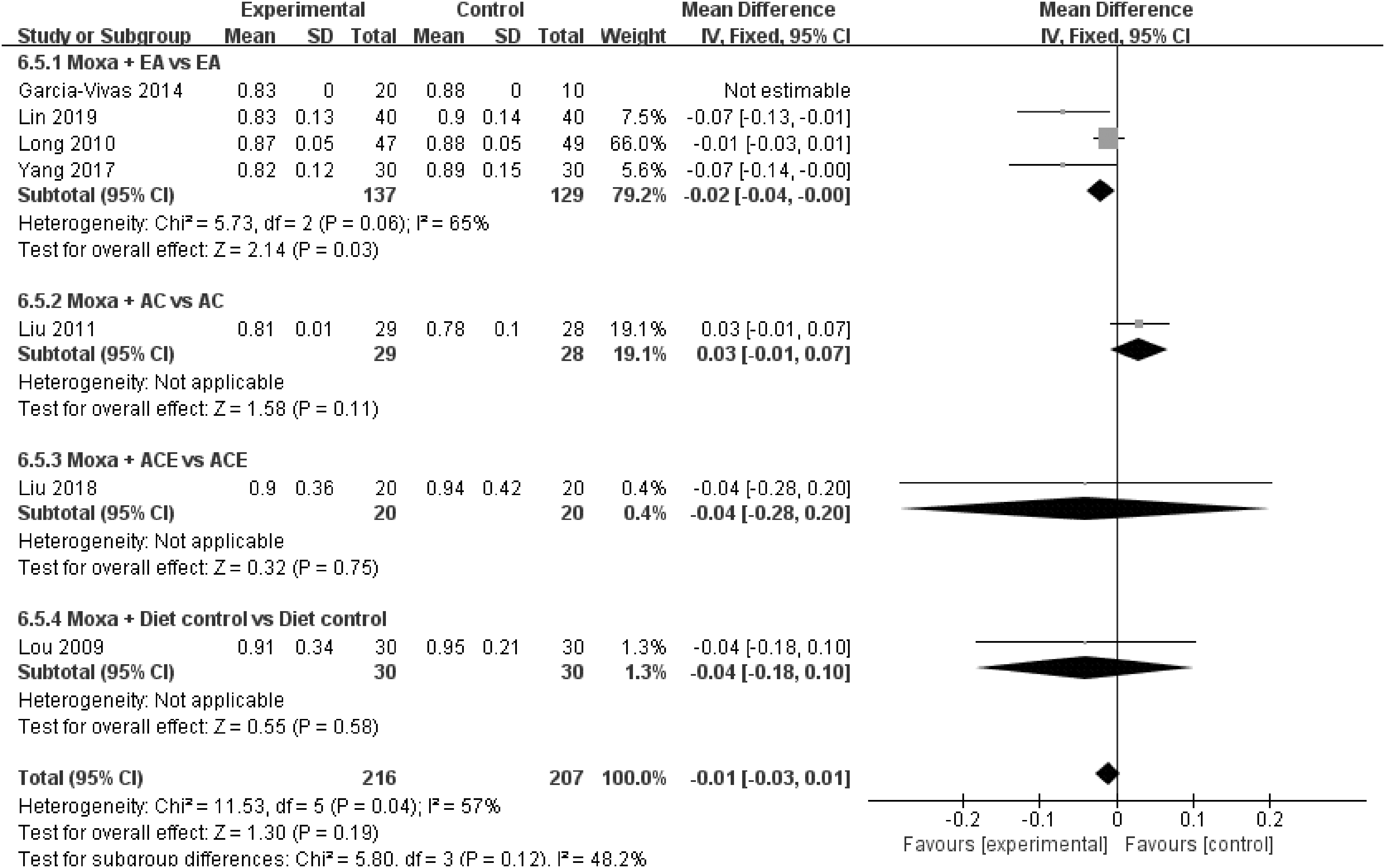
WHR (subgroup analyzed by treatment type of interventions combined with moxibustion). AC, acupuncture; ACE, acupuncture embedding therapy; EA, electroacupuncture; WHR, waist-to-hip ratio.
Limitations
This review has several limitations. First, there was high heterogeneity due to inconsistencies in the type of intervention, duration, and evaluation time. This effect was partially offset by the subgroup analysis. Second, several studies with a high risk of bias were included. Well-designed RCTs using high-quality methodologies should be conducted in the future. Third, most of the included studies were conducted in China, except for one from Mexico. As TCM treatments are commonly performed in China, cultural practices in China may be another cause of bias in this review.
Therefore, geographically diverse RCTs need to be conducted. Fourth, no analysis was conducted according to the location of moxibustion on body surface. Further research should be conducted that sets interventions by the moxibustion location. Despite these limitations, this is the first systematic review to evaluate the effectiveness of moxibustion for obesity and, therefore, makes a significant contribution to the literature.
Discussion and Conclusions
Obesity is the underlying cause of several chronic diseases, and its prevalence has been increasing in Korea. 32 According to the World Health Organization, a BMI of 30.0 kg/m2 or higher implies obesity. Body weight, BMI, WC, HC, and WHR can be used as indicators of obesity. 33 Therefore, body weight was used as the primary outcome and the other indicators as secondary outcomes. In addition, since moxibustion is a component of TCM, many Chinese studies were included in this analysis.
There are a number of approaches to treating people with obesity, including diet control, exercise, medications, and surgical treatment. 34 In the case of treatment with bariatric surgery, it takes the patient ∼3 months to adapt to the new eating patterns. In addition, there is the possibility that they develop vitamin and mineral deficiencies. 35 Pharmacologic treatment for obesity is mainly based on serotonin agents, and side effects may include lethargy, sweating, narcolepsy, and nausea. Given the significant limitations in the existing treatment modalities, it is necessary to find a new approach to the treatment of obesity.
Obesity has been dealt with extensively in TCM, with the use of herbal medicine 36 and acupuncture. 7,11,12,37 Although there have been fewer studies on moxibustion than on these other modalities, the number of studies focusing on the use of moxibustion has been increasing. 11,12,38 Several researches have suggested potential mechanism of moxibustion on obesity or related problems. One study presented that local heat stimulation can activate beige fat through the HSF1-A2B1 transcriptional axis that can be a promising strategy against obesity. 14
Another study showed heat stimulation induces upregulation of UCP1 and FGF21 expression in serum and/or white adipose tissues (WATs), which is correlated with reduced total body and WAT weight gain. 15 Furthermore, animal studies have shown that moxibustion can be used to adjust the level of fat accumulation, blood lipids, and female sex hormones. 39,40
This meta-analysis was based on 11 RCTs that examined the effects of moxibustion and combination of other therapies on obesity. Combination of moxibustion and other approach had a beneficial effect on the weight, BMI, WC, and efficacy rate of patients with obesity.
According to this study design, RCTs could be classified into five types: RCTs that compared combined moxibustion and electroacupuncture (experimental group) with only electroacupuncture (control group); RCTs that compared combined moxibustion and acupuncture (experimental group) with only acupuncture (control group); RCTs that compared combined moxibustion (experimental group) and embedding therapy with only embedding therapy (control group); RCTs that compared combined moxibustion and herbal medicine (experimental group) with only herbal medicine (control group); and RCTs that compared combined moxibustion and diet control (experimental group) with only diet control (control group).
Compared with the control group, the experimental group showed significant improvements in both the primary outcome, body weight, and the secondary outcomes, BMI and WC. However, since some of the studies included in this review had a high risk of bias, this conclusion should be carefully interpreted before application to clinical practice.
Adverse events were observed in two studies. 22,26 In one study, 22 dizziness occurred in two patients in the experimental group and one in the control group, but they soon recovered. In another study, 26 there were four cases of adverse events. Three patients experienced mild bleeding from the acupuncture point, which stopped without major intervention. The other patient experienced burns after moxibustion. Routine treatment was given to these burns, and treatment was resumed after 4 days. Since moxibustion is a treatment that involves thermal stimulation, there is a risk that burns can occur. Therefore, clinicians should be cautious.
The level of evidence and the reasons for the downgrades and upgrades are given in Table 2. Due to performance bias and obvious heterogeneity, the ratings for evidence quality for the overall outcomes ranged from moderate to very low. The ratings for evidence quality were as follows: moderate for body weight; low for the HC; and very low for BMI, WC, and WHR.
Summary of the Findings
If any of the three items (random sequence generation, blinding of participants and personnel, blinding of outcome assessment) are high risk, the level is considered to be “severe.”
If I 2 < 50, inconsistency would be considered “not serious”; 50 < I 2 < 75, “serious”; and I 2 > 75, “very serious.” Even though 50 < I 2 < 75, it is considered “not serious,” if the results of studies are located on the same direction.
The imprecision would be considered “not serious” if the total number >100, whereas it would be considered “serious” if the total number <100, or the CI of MD include 0 even if the total number >100.
Effective rate would be considered “serious.”
CI, confidence interval; HC, hip circumference; MD, mean difference; OR, odds ratio; WC, waist circumference; WHR, waist-to-hip ratio.
To the authors' knowledge, this is first study to report the effect of moxibustion combined with other interventions for body weight reduction. While several systematic reviews have reported the effects of diverse TCM modalities on obesity including moxibustion, 18,41 no study has been exclusively dedicated to investigate the effects of moxibustion or its combined influence with other interventions on obesity. The result of this research may indicate the need for further studies on the effects of thermotherapy, including moxibustion, on obesity. Also because none of the studies included in this research used moxibustion as single treatment for obesity, additional randomized clinical trial using moxibustion as a single treatment for obesity will be needed to clearly show the effect size of moxibustion.
In conclusion, this systematic review and meta-analysis examined the effect of moxibustion combined with other interventions on obesity. Moxibustion combined with other interventions was found to have a positive effect on the body weight, BMI, WC, and efficacy rate of people with obesity without any serious adverse events. Therefore, moxibustion may be combined with other interventions to treat obesity. However, the overall quality of the included RCTs was relatively low.
Therefore, this recommendation should be carefully applied in clinical practice. Moreover, most of the included studies had low methodological quality and high heterogeneity. Therefore, the results should be considered with caution. Studies with a strict research design and more participants need to be conducted to confirm these findings.
Data Availability Statement
Data will be provided upon request to the corresponding author.
Footnotes
Authors' Contributions
Hye.K. contributed to conceptualization, formal analysis, investigation, and writing—original draft. Hyu.K. was involved in data curation, investigation, and writing—original draft. W.-C.S. carried out visualization and writing—review and editing. S.K. took charge of resources and validation. J.-H.C. was in charge of methodology and supervision. M.-Y.S. carried out supervision. W.-S.C. was in charge of project administration and supervision.
Author Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
This research was supported by a grant from the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (Grant Nos. HI20C1405 and HF20C0208).
Supplementary Material
PRISMA_2020_abstract_checklist
PRISMA_2020_checklist
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.