
Abstract
Objectives:
To evaluate the effectiveness of weaving therapy on clinical outcomes and quality of life of autistic children.
Design:
Randomized waitlist-controlled trial.
Setting/Location:
Developmental and Behavioral Pediatrics Clinic, Faculty of Medicine Ramathibodi Hospital.
Subjects:
Twenty-three autistic children.
Interventions:
Weaving therapy was performed weekly for 6 months (3 months for hospital-based intervention and 3 months for home-based intervention).
Outcome measures:
Childhood Autism Rating Scale—second edition (CARS-2) and Pediatric Quality of Life Inventory (PedsQL) were measured at preintervention, 3 and 6 months postintervention.
Methods:
Twenty-three autistic children, aged 7.8–16.6 years, were randomized into an intervention group (N = 11) and a 3-month waitlist period group (N = 12). Ten weaving sessions were performed by the children, along with their parents, weekly for 3 months in hospital, and continued at home for an additional 3 months. The weaving therapy was delayed for 3 months in the waitlist group, followed by a 6-month intervention as the intervention group.
Results:
There was significant improvement on CARS-2 (p < 0.01) and PedsQL scores (p < 0.01) in the intervention group after the first 3-month weaving therapy. Meanwhile, in the waitlist group, no significant difference was found on CARS-2 (p = 0.09) and PedsQL scores (p = 0.26) during no weaving period. After the waitlist group began weaving therapy for 3 months, the authors found a significant improvement on both CARS-2 and PedsQL scores (p < 0.01both). Between-group comparisons showed that the intervention group had significant improvement on CARS-2 (p = 0.002) and PedsQL (p < 0.001) after 3-month weaving comparing with the waitlist group. After all the 23 participants finished a 6-month weaving therapy, there was significant difference in CARS-2 (p < 0.001) and PedsQL scores (p < 0.001) between pre- and postintervention.
Conclusions:
These findings suggest that traditional Thai fabric weaving therapy, as an alternative and complementary intervention, appears to be an effective therapy in improving the clinical symptoms and quality of life among autistic children.
Clinical Trial Registration number: TCTR20200420002
Introduction
Autism spectrum disorder (ASD) is one of the most common neurodevelopmental disorders characterized by difficulties in social communication accompanied with the presence of repetitive and restrictive behaviors, interests, and activities. 1 The prevalence of ASD has been increasing dramatically in the last few decades. It is estimated that the worldwide prevalence is 1 in 54 children in a recent study. 2 As a lifelong disorder, ASD significantly affects the child's and family's quality of life.
Several treatment strategies for ASD have been proposed such as behavior therapy, speech therapy, occupational therapy, individual education program, and medication. 3 Since there is no definite treatment for ASD, many parents turn to alternative medicine. Up to 28%–95% of autistic children have been reported to use at least one type of complementary and alternative medicine (CAM). 4
CAMs are usually referred to a broad set of health care practices that are not part of that country's own tradition and are not integrated into the dominant health care system. 5 CAMs for ASD can be categorized into biological therapies (e.g., alternative diets, neurofeedback, chelation, hyperbaric oxygen therapy, intranasal oxytocin, melatonin, Traditional Chinese herbal Medicine, and cannabis) and nonbiological therapies (e.g., sensory integration, music therapy, art therapy, yoga, massage, acupuncture, and animal-assisted therapy). 4,6 Although some interventions may be effective in alleviating certain symptoms and improving certain skills, the scientific evidence backing up their effectiveness remains scarce. 6,7 In Thailand, Thai elephant-assisted therapy program 8 and Thai traditional massage 9 for individuals with ASD were reported to be beneficial for sensory processing, postural control and balance, anxiety, and conduct problem without any adverse effect.
Art therapy is an intervention based on theories that the creative process involved in artistic self-expression helps people handle their problems and provides sensory stimulation in a safe organized environment via art materials and techniques. 10 Many studies showed that using different forms of art therapies (e.g., drawing, painting, collage, sculpture, fabric, and fiber art) in autistic children can improve self-esteem and self-awareness, minimize stress, improve interpersonal skills, and improve coping skills. 10 –12 Art therapy can also improve social communication skills, cognitive function, flexibility, attention, emotional control, internalizing/externalizing behavioral problems, sensory processes, motor coordination, quality of life, and relaxation. 10,13 –15 A recent systematic review highlighted the importance of providing a safe sensory-rich environment, promoting a variety of visual, tactile, and kinesthetic experiences and engaging in reciprocal communication via the symbolic means of art in autistic children. 10
Traditional Thai fabric weaving is an art that can be used as art therapy for autistic children. The advantage of soft, smooth, and colorful thread materials provides both visual and tactile stimuli to attract the child to participate in continuous and meaningful repetitive motion during the fabric weaving process. The aesthetic value of creative art also provides opportunities for occupational training and economic-related life skills for children and families. 16 Previously, weaving activities that were arranged for children with special needs in Thailand received positive responses from both parents' and coaches' perspectives. The purpose of this study was to evaluate the efficacy of fabric weaving therapy in autistic children.
Materials and Methods
Participants
The autistic children who attended the developmental and behavioral clinic, Faculty of Medicine Ramathibodi Hospital, Bangkok, were enrolled in the study. The ASD diagnosis was done by board-certified developmental and behavioral pediatricians using clinical criteria based on the Diagnostic and Statistical Manual of Mental Disorders-5 (DSM-5). 1 The ASD diagnosis was confirmed by the Developmental, Dimensional and Diagnosis interview (3Di). 17 Children were recruited only if they had the competency to cooperate, focus on tasks, and can follow the steps of weaving process with parental support. Children who had serious motor or neurological diseases, which may interfere with the weaving process, were excluded from the study. Eligible participants were randomly assigned to either the intervention group or waitlist control group.
Procedure
Ethical approved was granted by the Institutional Review Board, Faculty of Medicine Ramathibodi Hospital (No. MURA2019/196). The study has been registered at the Thai Clinical Trial Registry (
Eligible participants were contacted via telephone for a preliminary interview, providing research information and recruitment details. Written informed consents were obtained from all parents. Participants were randomly allocated to either the intervention group or waitlist control group using computer-generated random numbers (
The time frame of the study was divided into T0 (preintervention), T1 (at 3 months), T2 (at 6 months), and T3 (at 9 months). Both groups received the same intervention protocol, but with a 3-month delay in the control group. At T0, all participants were assessed for intelligence or adaptive function using either the Wechsler Intelligence Scale for Children—third edition (WISC-III) 18 or Vineland Adaptive Behavior Scale (VABS). 19 Concurrently the Childhood Autism Rating Scale—second edition (CARS-2) 20 and Pediatric Quality of Life Inventory (PedsQL) 21 were performed. The intervention was hospital-based weaving started at T0, while the waitlist control group received standard therapy at T0 and started hospital-based weaving at T1.
Subsequently, both groups received home-based weaving for further 3 months following hospital-based weaving. CARS-2 and PedsQL were redone after completion of hospital-based weaving and home-based weaving. Parent satisfaction questionnaire was also completed after hospital-based weaving. The study time line is demonstrated in Figure 1.
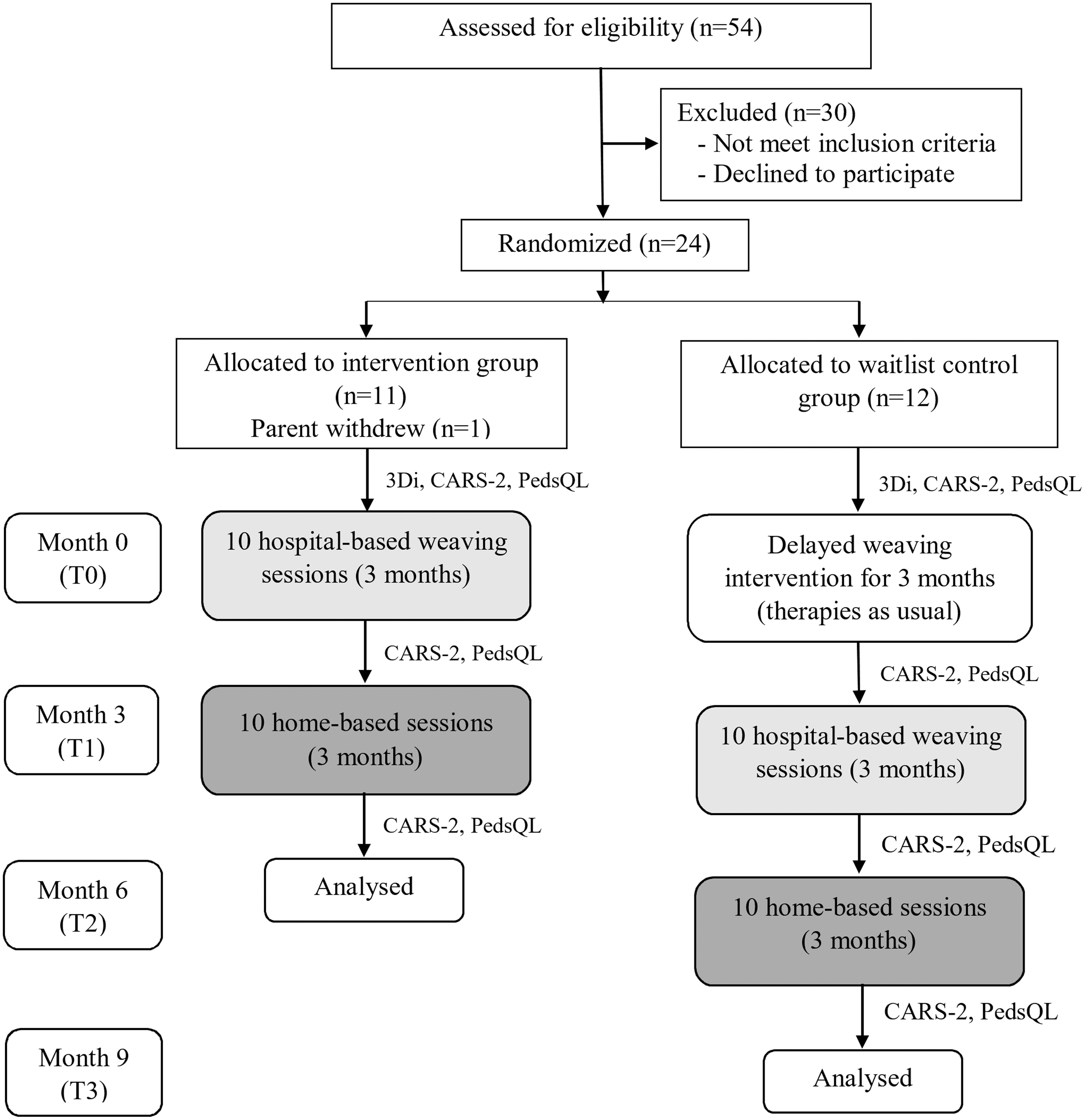
Flow diagram shows the enrollment, allocation, and intervention time line.
Intervention
The authors specially made a handloom, which is a device to weave fabric by interlacing two sets of yarns into patterns, to use in this study. The size of the loom was reduced from the traditional loom to fit the children and easily movable for home-based intervention. The wooden loom frame and a single stick used to insert into the warp to make interlace were designed to be safe. The weaving process was simplified and demonstrated to be feasible with each participant.
Fabric weaving sessions were organized by the Heartist project manager (previously organized fabric weaving activities for children with special needs in a regional area of Thailand), art therapists, volunteer cotherapists, and developmental and behavioral pediatricians. All 10 hospital-based sessions were held weekly for 3 months. Each session lasted 45–60 min. The participants and parents were trained one-on-one by the therapists. Participants were introduced to use the wooden looms, threads, and weaving materials. Weaving techniques were interactively taught under therapists and parents' supervision. The children had their chance to express their imagination in the creation of color selection, type of threads, pattern, and were encouraged to weave by themselves. Parents were allowed to help and promote social interaction. Participants who failed to attend at least 80% of the sessions were excluded from the study.
After completion of hospital-based weaving, the participants continued weaving at home weekly for another 3 months. The time spent in weaving activity was recorded in a diary. The woven fabric progression was evaluated monthly by the therapists. Weaving materials and the recommendation were provided regularly. All participants must engage in the weaving activities at least 80% of the 10 home-based sessions.
Measurements
Childhood Autism Rating Scale—second edition
The CARS-2 is clinical rating scale widely used to identify ASD and determine clinical symptom severity. Fifteen items (e.g., relating to people, emotional response, verbal communication, listening response) ranging from 1 (appropriated for age), 2 (mild symptom), 3 (moderate symptom), to 4 (severe symptom) are manual-guided scoring by a clinician using a combination of directed observation, parent interview, and questionnaire. CARS scores range from 15 to 60, and the cutoff point for an autism diagnosis is a score of 30 or above. The scores between 30 and 37 indicate mild-to-moderate autism and scores between 38 and 60 are characterized as severe autism. 20
Developmental, Dimensional, and Diagnosis interview
The 3Di is a computerized parent interview focused on current behavior and development for ASD assessment. Fifty-three questions of abbreviated version were translated and validated for the Thai population. After coding the interview data, results were computerized interpreted into subscale scores consisting of social reciprocity, communication skill, and repetitive behavior domains. A higher score means more impairment in development and current behaviors. 17
Pediatric Quality of Life Inventory
The PedsQL is a widely used questionnaire to measure health-related quality of life. Twenty-three items of 5-point scale rating, ranging from 0 (never), 1 (almost never), 2 (sometimes), 3 (often), to 4 (almost always), are grouped into four subscales consisting of physical functioning, emotional functioning, social functioning, and school functioning. A higher score means worse quality of life. 21
Parent satisfaction
A 7-point Likert-scale questionnaire was used to evaluate parents' overall satisfaction with the intervention.
Weaving diaries
Parents were asked to record time spent for weaving at home weekly (min/week).
Statistical analysis
All analyses were conducted using Stata version 18 (StataCorp, College Station, TX). A convenience sampling was utilized for the study and the sample size was not calculated as the study focused on a new intervention. Descriptive statistics were used to describe baseline demographic data. A normal distribution of scores was assessed by the Shapiro–Wilk test of normality. The results were not normally distributed, and nonparametric statistics (Wilcoxon signed-rank tests) were conducted. The paired t test was used to compare the scores that were normally distributed. Regarding between-group comparison of CARS-2 and PedsQL scores, analysis of covariance (ANCOVA) was performed with the preintervention scores as a covariant and postintervention scores as the dependent variable. The significance level was set at p < 0.05 for all analyses. CONSORT Checklist for randomized-controlled trials can be found in Supplementary Material.
Ethical considerations
The study protocol was based on the Declaration of Helsinki for Medical Research Involving Human Subjects. Before commencing the research, the protocol was approved by the Ethics Committee of Mahidol University (ID 312).
Results
Participant characteristics
Twenty-three children were enrolled in the study. The mean age was 12.2 ± 2.6 years. Eighteen participants were male and five participants were female (Table 1). All participants were confirmed ASD diagnosis by 3Di. There was no significant difference in sex, age, IQ, medication, conventional therapy, family income, and maternal education, and baseline mean scores of CARS and PedsQL between groups. Mean intelligence quotient of all participants was 65.0 ± 21.1. Eight children had no intellectual disability (ID; IQ ≥70) and 15 children had ID (IQ <70).
Demographic Characteristics of Participants
1 USD = 33 baht.
SD, standard deviation.
All the 23 participants attended more than 80% of weaving sessions. The median time spent on home-based weaving was 80 min/week (interquartile range 47.5–162.4). Participants without ID spent significantly lower time on weaving at home than participants with ID (42.5 and 135 min/week, respectively, p = 0.03).
Clinical outcomes
Tables 2 and 3 demonstrate the improvement on CARS-2 and PedsQL before and after the weaving intervention. In within-group comparisons during the first 3 months (between T0 and T1), the authors found a significant improvement on the total score of CARS-2 (p < 0.01) and PedsQL (p < 0.01) in the intervention group. Meanwhile, total scores of CARS-2 and PedsQL in the waitlist control group had no significant change due to no weaving intervention. The waitlist control group began weaving at T2, and after a 3-month hospital-based weaving therapy, the authors found significant improvement in the total score of CARS-2 (p < 0.01) and PedsQL (p < 0.01). Comparing pre- and postintervention scores of both groups (between T0 and T2 in intervention group and between T0 and T3 in waitlist control group), results showed a significant improvement on total score of CARS-2 and PedsQL, except for PedsQL in the waitlist control group.
Mean Scores (Standard Deviation) of Childhood Autism Rating Scale—Second Edition and Median Scores (Interquartile Range) of Pediatric Quality of Life Inventory of Intervention Group at T0, T1, and T2 (N = 11)
p < 0.01; compared with T0.
CARS-2, Childhood Autism Rating Scale—second edition; IQR, interquartile range; PedsQL, Pediatric Quality of Life Inventory; SD, standard deviation.
Mean Scores (Standard Deviation) of Childhood Autism Rating Scale—Second Edition and Pediatric Quality of Life Inventory of Waitlist Control Group at T0, T1, T2, and T3 (N = 12)
p < 0.01; compared with T0.
CARS-2, Childhood Autism Rating Scale—second edition; PedsQL, Pediatric Quality of Life Inventory; SD, standard deviation.
Between-group comparisons on total score of CARS-2 and PedsQL at T1 (completed the 3-month hospital-based weaving therapy in intervention group, but no weaving therapy in waitlist control group) showed a significant difference in both CARS-2 and PedsQL scores (p = 0.002 and p < 0.001, respectively) after adjusting for preintervention scores by ANCOVA (Table 4).
Comparison of Mean Difference Between Intervention Group and Waitlist Control Group at T1
p-Value from ANCOVA with preintervention scores as a covariant.
ANCOVA, analysis of covariance; CARS-2, Childhood Autism Rating Scale—second edition; CI, confidence interval; PedsQL, Pediatric Quality of Life Inventory.
According to an analysis for all 23 participants, there was a significant reduction in total CARS-2 scores and total PedsQL scores from pre- to postintervention (p < 0.001 both). Regarding PedsQL subscale scores, significant improvements were found on the physical functioning, emotional functioning, and school functioning subscales (p < 0.05 all). However, there was no significant change in social functioning scores of PedsQL (Table 5).
Median (Interquartile Range) of Childhood Autism Rating Scale—Second Edition and Pediatric Quality of Life Inventory of All Participants at Baseline and Endpoint (N = 23)
CARS-2, Childhood Autism Rating Scale—second edition; IQR, interquartile range; PedsQL, Pediatric Quality of Life Inventory.
Parent satisfaction
According to parent satisfaction, 100% of parents were satisfied with the weaving activity. Parents reported that their children increased their attention gradually during 6 months of activity. Ninety-six percent reported that the intervention improved child's eye–hand coordination and 87% reported improve parent–child relationship. The majority (91%) of parents reported that their children showed happiness during intervention. Furthermore, 78% reported improvement of child's self-control. No adverse events related to fabric weaving therapy, such as injury from a wooden loom frame, a stick, threads, and weaving materials, were reported during the hospital-based or home-based weaving intervention in both groups. None of the participants reported any unusual symptoms or abnormal complaints experienced at any time during and after intervention.
Discussion
To the best of knowledge, this is the first study that showed benefits of traditional Thai fabric weaving therapy in autistic children. The authors found improvement regarding clinical symptom severity and quality of life after weaving intervention. The results showed that there are significant differences between the mean scores of CARS-2 and PedsQL between pre- and postintervention. These findings are consistent with previous studies that utilize other forms of art therapy in autistic children such as individual session, small group activity, or integrated into another therapy program. 10,14,22,23 A study of family training based on the art program showed significant improvement in clinical severity using the Gilliam Autism Rating Scale (GARS). 24 One study that uses art therapy in social skill therapy program revealed significant improvement in social assertion scores and problem behaviors using the Social Skills Rating System (SSRS). 25
Furthermore, studies in China showed improvement in communication skills and cognitive and behavioral performance in children with ASD. 26,27 The mechanism of art therapy effectiveness remains unclear, and therefore, further study regarding objective evaluation such as neurological imaging, and cellular or molecular study should be investigated.
As the authors integrated home-based weaving therapy in the study, they believed that weaving can be a recreation activity for children. This could improve the overall clinical severity of ASD owing to the activity that can enhance interpersonal interaction, communication, emotional control, adaptation to change, and activity level of autistic children. 24 Also, family members' and teachers' involvement can help to achieve better positive outcomes. 22 These might support the improvement of overall health-related quality of life that was found in the study.
After 6 months of intervention, the authors found significant improvement in physical functioning, emotional functioning, and school functioning. In fact, the weaving process allows children to practice fine motor, motor coordination, and imitation. Previous studies found significant improvement on the physical subscale of PedsQL after art therapy, which supported this study. 10 Moreover, movement of structural weaving process may also redirect the repetitive behavior of autistic children to be more purposeful, which might reduce nonpurposeful repetitive behaviors. Also, weaving is a quiet, calming, and relaxing activity in which children can develop and express their creative ideas.
One study also showed significant improvement on emotions after participating in painting therapy. 28 However, the subscale of social functioning had no significant difference after intervention. It is possible that the majority of participants in the study had ID. They spent most of the time at home or special education needs schools; therefore, the authors did not find the impact of intervention on social functioning.
The authors allowed the participants to select the color and type of thread and pattern, using their creativity. This strategy might motivate a child to engage in activity for a longer period of time and gain sense of self-control. The results found that children increased their attention and self-control by parental report during the weaving intervention. Similar results from previous studies stated that individuals with cognitive impairments were more successful in a task when given a choice of task. 29,30
In contrast to previous art therapy studies that mainly focused on high-functioning children with ASD, 10,14 this study recruited both ASD with and without ID. For ASD with ID group in this study, the outcomes were more promising compared with ASD without ID. They had better compliance for weaving activity at home because they had more free time with families. The results showed they had improvement in both clinical symptom severity and quality of life. The implementation of weaving as a form of art therapy is not limited by age, cognitive function, or disease severity, and is easy to be accepted by children and families. 31
Limitations
First, parents and researchers in the study were not blind to the intervention that children received, and therefore, they could have a bias on children's evaluation. Second, the authors had no follow-up evaluation after the endpoint of the study. Therefore, they did not know the durability of the intervention effects. Long-term follow-up assessment should be done.
Conclusions
These findings suggest that Thai traditional weaving can be used as an effective therapy combined with the conventional treatment of ASD to improve clinical symptom progression and quality of life in autistic children.
Footnotes
Acknowledgments
The authors would like to thank all the children and families who participated in this study. The authors are grateful to the Heartist project manager, therapists, and volunteers for organizing weaving therapy.
Authors' Contributions
Conceptualization: P.P., P.W., S.R., and J.C. Methodology: P.P. and J.C. Data curation: P.P. and J.C. Formal analysis: P.P. and J.C. Investigation: P.P. and J.C. Writing—original draft: P.P. Writing—review and editing: K.C. and J.C. Supervision: J.C.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by the Faculty of Medicine, Ramathibodi Hospital, Bangkok, Thailand (RF_62069).
Supplementary Material
CONSORT_checklist