
Abstract
Background:
Normal labor is stressful, and the intense pain and anxiety can have an adverse effect on the mother, the fetus, and the delivery procedure. This study aimed to determine how acupressure applied to multiple acupoints during normal labor affected labor pain and anxiety in primiparous women.
Method:
This study was a double-blinded randomized controlled trial that involved 43 primiparous women aging 20–30 years who were referred for normal labor. Subjects were randomly allocated to one of two groups: acupressure or control. Acupressure was administered to the Large Intestine 4 (LI4), Heart 7 (He-7), and Spleen 6 (SP6) acupoints in the acupressure group, whereas sham acupressure was administered to the control group. The study assessed the mothers' anxiety levels using the Spielberger Inventory questionnaire and measured their pain levels using the visual analog scale before and after the intervention. In addition, pulse rate and blood pressure were also measured.
Result:
In the acupressure group, both the anxiety score and pain level showed a substantial improvement (p < 0.001), but in the control group, only the anxiety score showed a significant improvement (p < 0.001). After the intervention, the difference in anxiety and pain scores between the two groups is statistically significant (p < 0.001). Furthermore, neither group's blood pressure nor pulse rate showed any significant changes (p < 0.05).
Conclusion:
According to the study's findings, acupressure targeting LI4, He-7, and SP6 acupoints was effective in relieving anxiety and pain during labor. Compared with the sham acupressure group, the acupressure group showed a greater decrease in both anxiety and pain levels. As such, acupressure may be recommended as an effective, affordable, and accessible technique for managing pain and anxiety during labor. This study has been registered in the database of clinical trials under the identifier Clinicaltrials.gov NCT05411289.
Introduction
Delivery is a significant phenomenon and could be among the most traumatic and stressful experiences mothers have in their lifetime. 1 While maternal stress during pregnancy raises glucocorticoid levels in the fetus, it has negative consequences for the neurologic system. 2 Stress as well as the release of catecholamines and cortisol can prolong labor, reduce the blood flow to the placenta, and cause fetal hypoxia. 3 Prolonging the delivery time makes the pain worse and increases anxiety. 4 Acute stress causes the release of noradrenaline, which causes a state of anxiety response that enables the organism to hold high attention. 5
The manifestation of anxiety-like behavior after acute stress exposure is initiated by the persistent firing activity elicited by the stressor. 6 Furthermore, negative labor and delivery experiences that involve unanticipated medical interventions, intense pain, or fear of death cause women an immense amount of anxiety and fear and have been known to eventually result in anxiety disorders. 7 Fear and anxiety cause muscles to tense up more and send more blood and oxygen to the mother's muscles and brain. As a result, mother's sensitivity to pain, fatigue, and tension all increase, and she becomes less compatible with pain. 8
There are several medical and nonmedical techniques used today to decrease labor pain. 9 Nonpharmacologic techniques assist women in developing this capability to cope with stress and pain, reducing their probability of experiencing stress and anxiety during labor. 8,10,11 The utilization of nonpharmacologic approaches has many benefits, including a smaller negative impact on the mother and fetus and minimal disruption of the labor process. 12 This requires the adoption of nonpharmacologic pain-relieving techniques such as exercise, aromatherapy, touch, and acupressure. 13
Acupressure is one of these methods that has gained increasing interest for its potential to reduce labor-related issues such as easing labor pain, speeding up delivery, and reducing anxiety. 14 In contrast to acupuncture, which uses needles, acupressure is a Traditional Chinese Medicine treatment in which pressure is applied to specific acupoints situated at specific anatomical points. This method has benefits, including convenience of use, cost-effectiveness, and safety. 14
As a noninvasive technique, acupressure promotes blood circulation and vital functions, relieves pain, eases muscle tension, removes energy imbalances, and lessens the symptoms of anxiety. 15
The mechanism of pain reduction by acupressure may be explained by Melzack and Wall's Gate Control Theory. Acupressure stimulates large nerve fibers that transmit impulses to the spinal cord, which in turn can close the “gates” of pain transmission, potentially reducing the sensation of pain. By activating mechanoreceptors, acupressure triggers thick nerve fibers (A-alpha and A-beta) to close the “doors” that transmit pain signals. Conversely, fine nerve fibers (A-delta and C) can open these doors, influencing pain signal transmission. The gates of pain transmission can be kept closed by continuous stimulation, which might lead to less pain. 16
Acupressure promotes the production of opioids and endorphins in the body, which decrease pain and promote relaxation, which enhances overall well-being and reduces muscular soreness. 17
Numerous studies have found that stimulating a single point or a couple of points can minimize labor pain 18,19 and anxiety. 14,20 Heart 7 (He-7) acupoint is often employed to address emotional distress, pain conditions, and cognitive impairments. 21 The utilization of acupressure on the large intestine 4 (LI4) point has proven to be an efficacious approach for managing labor pain and reducing the duration of both the first and second stages of labor. 22 Furthermore, acupressure applied to the spleen 6 (SP6) acupoint is a viable alternative method that has shown promise in reducing maternal anxiety levels and the need for sedatives and analgesics during labor. 23
The ability of acupressure to relieve anxiety and pain during labor has not been adequately studied in controlled trials, as has been the case with other complementary and alternative therapies, which has restricted the use of this low-cost simple-to-apply technique in clinical settings. Furthermore, it is essential to evaluate the effectiveness of using a combination of various acupoints to alleviate labor pain and anxiety. In addition, stimulation of different points may result in different outcomes. This will aid in identifying the most effective methods for reducing both anxiety and pain during labor. The current randomized controlled trial aimed to detect the impact of LI4, He-7, and SP6 acupressure on anxiety and pain intensity in primiparous women during the active part of first-stage labor.
Materials and Methods
Study design
This parallel-group double-blind randomized controlled trial included 43 primiparous women. They ranged in age from 20 to 30 years. The study was carried out from June to September 2022 at Cairo University Hospital, Egypt. Before beginning the study, the Institutional Review Board of the Faculty of Physical Therapy, Cairo University, granted ethical approval under study number P.T. REC/012/003704. This study adhered to the CONSORT and STRICTA checklists (supplementary files 1 and 2). Before being enrolled in the trial, the patients gave their informed consent. Furthermore, all processes were carried out in conformity with the guidelines described in the Helsinki Declaration.
Participants
Patients who met the following criteria, as determined by a blinded obstetrician, were deemed eligible: primiparous pregnant women having no history of clinical, mental, or surgical problems and having experienced no problems during pregnancy with gestational ages between 37 and 40 weeks according to the last menstrual cycle date, which has been confirmed by ultrasound in the first and second trimesters, and a fetal weight of 2500–3500 g as determined by ultrasonography, cervical dilatation of 3–4 cm, the absence of problems that could cause dystocia during labor, with one healthy fetus in the vertex position, and neither anesthetic nor analgesia was administered during the first stage of labor.
Participants who needed an emergency C-section or oxytocin-assisted labor, had fetal distress, or had pregnancy complications, such as gestational diabetes, intrauterine death, and preeclampsia, were excluded, as were those who had psychological disorders or systemic diseases while pregnant, took pharmacologic pain relievers, had lesions in acupressure points, had communication problems, or were taking medication for those conditions.
Upon recruiting eligible patients, a block randomization strategy was utilized to assign participants randomly to the acupressure or control group at a preset ratio of 1:1. The assignment of participants to their respective groups was carried out by a blinded assistant in a sequential manner through the use of an opaque envelope, which was created by an impartial party using a process of random number generation. To mitigate the risk of bias, all participants, outcome assessors, and data analysts were kept blinded to the group assignments of the research participants. The researcher who delivered the intervention was aware of the group assignment.
Outcome measures
All outcome measures were evaluated before and after 30 min of cessation of the intervention by the assistant researcher. The Spielberger Inventory's anxiety score and the visual analog scale's (VAS's) pain score served as the primary outcome measures. Changes in blood pressure and pulse rate served as secondary outcome measures. The Spielberger Inventory was employed to assess anxiety form (y), which was utilized to assess anxiety's contextual or transitory activation. 24
The primary objective of the anxiety scale was to determine the severity of anxiety, ranging from mild to severe. For this study, a questionnaire comprising 20 brief items was employed to evaluate anxiety. The lowest possible score was 20, indicating that there was no anxiety, whereas the highest possible score was 80, indicating the most severe level of anxiety. 25 Form Y is a more refined version of the anxiety scale, with better-defined state and trait anxiety factors. Its simple structure is more precise, and the anxiety factors are more stable and distinguishable.
Currently, this form is more commonly utilized than the original Form X. In this study, the section of Form Y that assesses state anxiety was utilized. The participants used the VAS to rate their pain level. It uses a scale on a 10-cm ruler with no pain indicator at one side and the strongest pain sign at the opposite end to enable users to evaluate their own experience of pain.
The most widely used pain assessment instrument in the world is the VAS. The VAS is a standard technique for determining the level of pain severity, and prior research has validated its validity and reliability. 26 Heart rate (HR) and blood pressure were assessed three times by the Boso Medistar + fully automatic wrist blood pressure monitor 476/Germany, and the average of them was calculated.
Intervention
Acupressure
Acupressure intervention was carried out during the patient's uterine contractions (the frequency of contractions varied for each individual patient). Applying pressure was stopped by the end of each contraction and started again at the beginning of another contraction. The participants were positioned in their preferred positions. LI4 and He-7 points were the initial two locations to be pressured bilaterally, followed by SP6 point. LI4 acupoint was found radially to the middle of the second metacarpal bone on the hand's dorsum.
The He-7 acupoint is situated in the tiny dip between the pisiform and ulnar bones at the ulnar edge of the transverse crease of the wrist. The SP6 point is four finger-widths from the medial malleolus, behind the posterior edge of the tibia. When respondents described feeling tingling, numbness, heaviness, pressure, or a pleasant sensation in the acupoint location, the precise location of the acupoint was verified. Also, the Acuhealth TENS Pro 900 (Acuhealth Pty, Stepney, South Australia) was utilized to verify the precision of the acupoint localization. Acupoints have a lesser electric resistance than their surroundings, which causes this instrument to make a different sound there.
The intervention was carried out by the primary researcher, a highly skilled physiotherapist who possesses specific training in acupressure with 5 years of practical experience in the field. The transformation of the researcher's nail bed to white served as an indicator of proper pressure intensity. 23 Pressure was applied intermittently for 1-min durations during contractions, followed by 1-min relaxation periods. No pressure was applied between contractions.
This cycle was repeated, resulting in a cumulative total of 30 min of pressure application. Where the study was conducted, the pregnant woman was accompanied by a companion, typically a nurse, who instructed the laboring women to take slow deep breaths in and out of their thoraxes (slow thorax–abdomen breathing rhythm) during the contractions and between them to completely relax their bodies.
In the control group, they simply provided routine care; no special labor techniques or painkillers were given. In the control group, sham acupressure was administered to non-acupoints at the dorsal side of the hand and the tibia. These areas were chosen because they do not align with the meridians, and they were ∼3–4 cm away from the acupoints under study. Non-acupoints are body points that are not represented on recognized acupuncture-point charts. 27 The researcher's thumb was used to apply pressure to non-acupoints of the participants' hands and legs (referred to as “sham points”) in the same way as the acupressure group.
Sample size and data analysis
The sample size was determined utilizing G*Power (version 3.0.10, Germany) based on the difference between two dependent means of the major outcome measurement (VAS score). According to the results in the literature, 14 the following parameters were used to determine the sample size: an analytical power of 90%, an alpha significance level of 0.05 (one-tailed), Cohen's standardized effect size d = 0.8, and a standard deviation of 2.
A sample size of 19 patients for each group was deemed sufficient, resulting in a total sample size of 38. To account for the anticipated high dropout rate, 60 patients were enrolled. Enrollment began in June 2022, and follow-ups ended in September 2022. Among the initial sample of 70 women who were assessed for eligibility, a randomized allocation process assigned 60 women to their respective groups. However, during the course of the study, 17 out of the 60 participants had a change in their birth plan and opted for a cesarean section instead of normal labor.
Consequently, the data from these 17 women were excluded from the subsequent analysis. Ultimately, a total of 43 participants from both groups adhered to the intervention, completed the required follow-up, and were included in the final analysis. Figure 1 displays how the participants progressed from the recruitment phase to the follow-up stage.
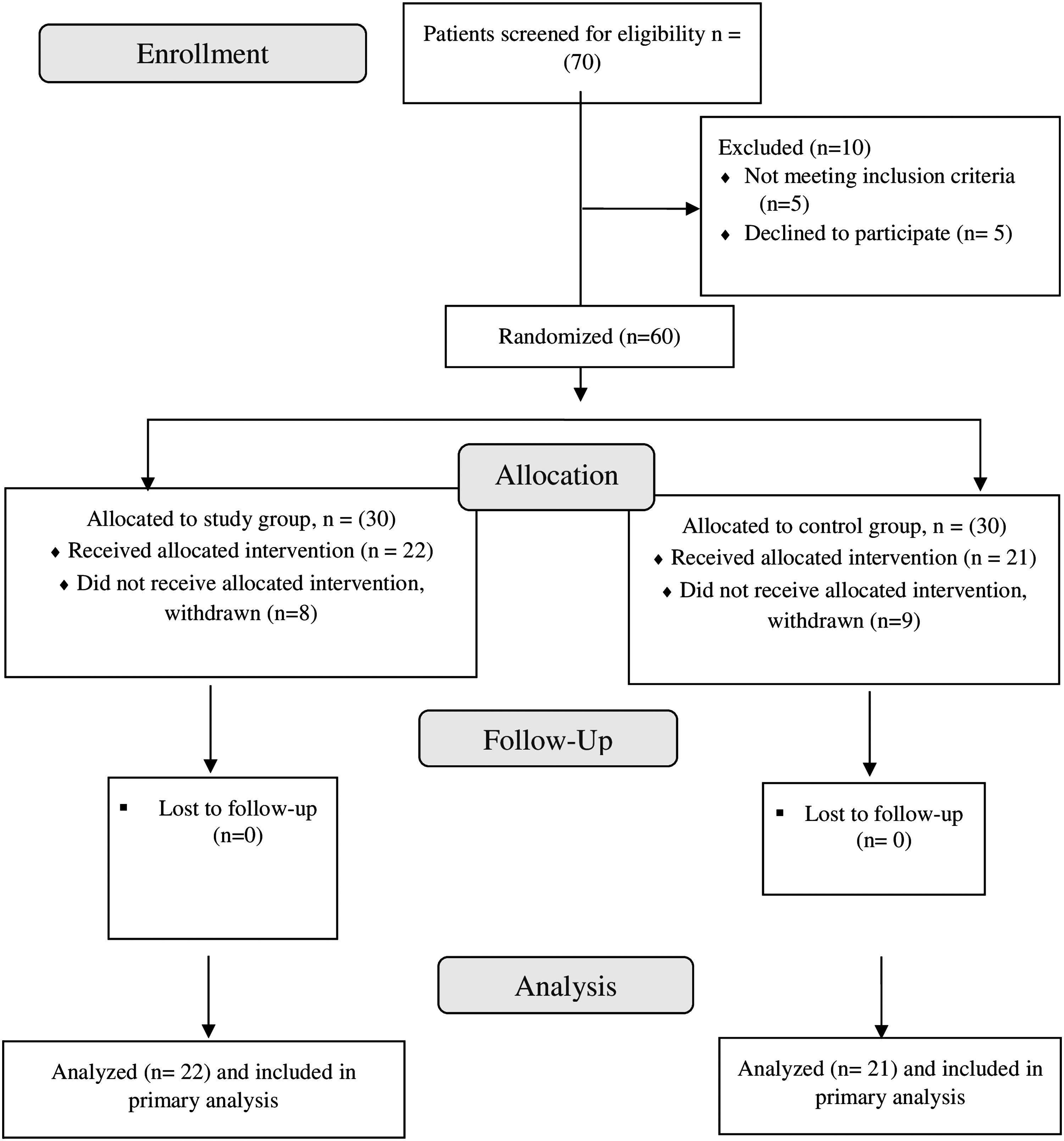
Consort diagram for the study.
Before the final analysis, the normality and homogeneity of variance for the dependent variables (HR, VAS, and anxiety score) were assessed using the Shapiro–Wilk and Levene's tests. The results showed no violations of these variables. However, the Shapiro–Wilk test indicated that the systolic blood pressure (SBP) and diastolic blood pressure (DBP) variables were not normally distributed. Unpaired t test and chi square were used to compare between subjects characteristics of the two groups.
For variables that were normally distributed, a two-way multivariate mixed model analysis of variance (MANOVA) was performed to assess the main effect between and within groups. For variables that were not normally distributed, Wilcoxon and Mann–Whitney tests were employed. Additional univariate analysis of variances (ANOVAs; two-way mixed models) were run when a significant time-group interaction effect was identified. To conduct the statistical analyses, SPSS version 23.0 (SPSS, Inc., Chicago, IL, USA) was used. The p-value cutoff for significance was established at 0.05.
Results
The data analysis revealed no discernible difference between the two groups before the intervention in terms of the demographic and clinical characteristics of the patients (p > 0.05). The mean ages of the two groups were comparable, with the acupressure group's mean age being 27.13 and the control group's mean age being 28.76 years. In the acupressure group and control group, the percentages of participants with a high school, a secondary school, and an elementary school were 40.0% vs. 60.0%, 64.7% vs. 35.3%, and 50.0% vs. 50.0%, respectively.
The distribution of occupations was similar in the two study groups, and housewives made up the majority of participants (48.1% in the acupressure group as opposed to 51.9% in the control group). No significant difference was found in the average gestational age between both groups (p = 0.241), as reported in Table 1.
Baseline Demographic and Clinical Characteristics of Patients
Level of significance at p < 0.05.
DBP, diastolic blood pressure; HR, heart rate; SBP, systolic blood pressure; SD, standard deviation; VAS, visual analog scale.
The analysis of the data indicated that there was no significant variation between the two groups in the measured variables before the intervention (p < 0.05). However, the repeated measures MANOVA revealed a significant main effect of time [Wilks' Λ = 0.246, F(3,39) = 39.79, p = 0.001, η 2 = 0.754] and a significant time-treatment interaction [Wilks' Λ = 0.516, F(3, 39) = 12.178, p = 0.0001, η 2 = 0.484], whereas no significant main effect of treatment was detected [Wilks' Λ = 0.852, F(3, 39) = 2.26, p = 0.096, η 2 = 0.148].
Follow-up univariate ANOVAs showed a significant change in VAS score [F(1, 41) = 13.95, p < 0.001, η 2 = 0.254] and anxiety score [F(1, 41) = 106.89, p < 0.001, η 2 = 0.723], but no significant change in HR [F(1, 41) = 2.88, p = 0.097, η 2 = 0.066]. The findings proposed that there were dissimilarities between the groups in a linear combination of outcomes during the pre- and postintervention phases.
Postintervention between-group analyses showed no significant differences in HR, SBP, and DBP, whereas there was a significant difference between both groups in VAS and anxiety score, with mean differences and 95% confidence intervals (CIs) for VAS [−0.688, CI (−1.049 to −0.328)] and for anxiety score [−5.86, CI (−9.74 to −2.00)], respectively (see Table 2).
Between-Group Analysis of the Outcome Variables
Significant.
MD, mean difference.
Safety
Throughout the trial, acupressure was generally considered safe. Ninety-nine percent of the study participants found acupressure to be tolerable. Acupressure therapy was not involved in the few modest self-limiting adverse events that occurred, as reported by the study's physician. Two participants in each group experienced postlabor weakness and dizziness, with one participant in each group reporting these symptoms. Furthermore, it was reported that a participant in the intervention group experienced postpartum hemorrhage as an unrelated adverse event to acupressure therapy.
Discussion
The aim of this study was to determine the effect of acupressure on anxiety and pain levels in primiparous women during normal labor. The findings of this study revealed that in the acupressure group, both the anxiety score and pain level showed a substantial improvement (p < 0.001), but in the control group, only the anxiety score showed a significant improvement (p < 0.001). The difference between the two groups' anxiety and pain scores after the intervention is statistically significant (p < 0.001).
These findings were consistent with those of Lee et al., who conducted a study comparing the impact of acupressure on anxiety levels during labor. They reported a considerable reduction in anxiety levels among the group that received acupressure treatment on the SP6 acupoint compared with the control group. 13 In another study, a significant improvement was also found in anxiety level at Point LI-4. 28 Although the exact mechanism of labor pain relief is not yet fully understood, some theories suggest that it may be linked to a reduction in anxiety levels. 13
According to two additional studies, acupressure was found to stimulate the release of neurotransmitters, including serotonin, which has a calming effect. 29,30 This has been shown to reduce pain intensity and decrease the use of morphine in patients. 31
In a Cochrane review that examined the effect of acupressure on pain management during labor, four studies involving 549 women were evaluated. Various acupoints, including SP6, LI4, and BL67, were used in these studies. The findings revealed that acupressure was linked to a decline in pain (SMD, −0.55; 95% CI −0.92 to −0.19); a reduction in the duration of labor (standardized mean deference [SMD], −1.06; 95% CI −1.74 to −0.38); and a decrease in cesarean rates (risk ratio, [RR], 0.24; 95% CI 0.11–0.54) compared with the sham acupressure. 32
Another study also demonstrated a reduction in pain among participants receiving acupressure treatment at 30 min postintervention compared with those in the touch and control groups (VAS score of 5.65 [1.87] vs. 6.85 [1.89] and 8.18 [1.59], respectively). 26
The Yin-Yang symbol, which is used in acupressure, stands for the traditional Chinese conception of how things function. As shown in Figure 2, the black and white shapes inside the circle reflect the interaction between the two energies known as “yin” (black) and “yang,” which allow everything to happen. The outer circle is symbolic of “everything.” They are neither entirely black nor entirely white, just as neither are things in life, and they are mutually exclusive.
yin and yang symbol. Reprinted from Cross. 33
The opposite of “yang” would be “yin,” which could be bright, active, upward, hot, expanding, and powerful; “yin” could be dark, passive, downward, cold, and contracting. The symbol's yin and yang portions' design really conveys a sense of the two energies' constant movement, from yin to yang and vice versa, which causes everything to happen, such as the expansion and contraction of things and the transition from hot to cold temperatures. 33
Acupressure theory posits that the body contains 12 energy channels, known as meridians. Disease and illness are thought to arise from an imbalance or disruption of the vital energy flow within these meridians. By applying pressure to specific points along these meridians, the flow of vital energy can be restored and balanced, thereby treating the underlying causes of disease. 34
In Traditional Chinese Medicine, the effectiveness of acupressure in relieving labor pain is attributed to the reinforcement of blood circulation and vital energy, relieving the cramping pain in the uterus of the pregnant women. 35 The gate control theory proposed by Melzack and Wall and endorphin-release theory are the other endogenous mechanisms may explain why acupressure decreases labor pain intensity. Acupoints are the locations of the sensory receptors with thin afferent fibers placed in the muscles.
The gate control theory explains that stimulation of the thick myelinated nerve fibers causes a neural inhibition at the spinal level, blocking the transport of the pain stimuli to the brain through the nonmyelinated nerve fibers. According to the endorphin release theory, acupressure-related pain relief may be explained by the release of a group of substances called endorphins, which are natural opiate-like substances, thereby causing the pain suppression. 16 Besides, the decrease in labor pain occurring during the acupressure might be attributed to the distraction from pain. Distraction includes providing the laboring women with specific activities so that their conscious thoughts and anxieties are reduced. 36
According to other studies, acupressure can trigger the release of certain peptides that have a similar effect to painkillers. This can lead to a reduction in the function of the sympathoadrenal system, which is activated during periods of anxiety. Therefore, acupressure may be able to lower anxiety levels without causing any significant changes in vital signs. 37 The decrease in vital signs observed during acupressure treatments is not considered clinically significant as they remain within the normal range. This may be due to the patients' stability during the intervention and the sense of comfort provided by the attention they receive. 38
Several studies have reported a reduction in anxiety levels in the placebo group after acupressure treatment at nontherapeutic points, or sham points. This suggests that the reduction in anxiety may be due to the massage technique itself or the belief that the intervention is beneficial, rather than specific acupressure points being stimulated. It is possible that patients experience a reduction in anxiety due to self-reassurance, and a sense of safety resulting from their participation in the study. 34,39 –42
Study strengths and limitations
The study's strengths include taking into account participant matching, homogeneity, and inclusion criteria. In addition, women in the experimental group were all subjected to the same level of pressure for the same duration of time. The study's strengths also included the use of specialized equipment to confirm the correct location of the pressure point. Furthermore, all participants receive acupressure from the same therapist. One limitation of the study is that no intention-to-treat analysis was used, which could have been beneficial for a more comprehensive evaluation.
Furthermore, the mother's questionnaire responses may be influenced by her level of pain and individual pain thresholds, both of which are variables that are outside the researcher's control. Larger sample size investigations should be carried out to confirm the findings of the authors.
Conclusion
In this study, acupressure treatments significantly lowered participant perceptions of labor pain and anxiety. On the basis of these results, the following conclusions can be made: to care for women who are in labor, labor and delivery nurses should be adequately educated in acupressure techniques. Families should be given training during the antenatal period, and a proper environment should be created for the application of these techniques.
Although the placebo effect was observed to have a positive impact on anxiety reduction in this study, the use of acupressure demonstrated even greater efficacy in reducing maternal anxiety levels and pain during labor. As such, acupressure can be regarded as a viable alternative method for pain management, with the potential to decrease the need for analgesic use. Finally, health care professionals can employ acupressure to reduce anxiety and the need for sedatives and analgesics during delivery.
Footnotes
Authors' Contributions
M.E.H. created the concept and design, collected data, organized the project, and wrote the article; S.H.E. wrote the article and contributed to the article; and M.M.T. helped create the concept and design, as well as write and revise the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was funded by Princess Nourah bint Abdulrahman University Researchers Supporting Project number (PNURSP2023R99), Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Supplementary Material
CONSORT 2010 Checklist
STRICTA-2010-Checklist