
Abstract
Background:
Several meditation interventions showed positive effects on physical and mental health. The aim of this study is a first evaluation of the (within-group) effects of a 21-day online meditation course of the “expansion method.”
Methods:
For this exploratory observational study, parameters were assessed at baseline, at 1 month, and at a 3-month follow-up. Exploratory endpoints were health-related quality of life (PROMIS Preference Score), global health (PROMIS) with the subscales physical and mental health, stress perception (Perceived Stress Scale), positive and negative affect regulation (Positive and Negative Affect Schedule), flourishing (Flourishing Scale), self-efficacy (Short Scale for Measuring General Self-Efficacy Beliefs), gratitude and awe (Gratitude and Awe Questionnaire), resilience (Connor-Davidson Resilience Scale), spirituality (Aspects of Spirituality), and mysticism (Mysticism Scale) on validated inventories. In addition, self-constructed questions (NRS) assessed health status, lifestyle, and concept evaluation.
Results:
Data from 359 participants were included in this study (response rate: 68% at 1 month, 46% at 3 months). The main analysis was based on the complete cases at 1 month (n = 244 participants; 84% female; 51 ± 11 years; 89% German). Medium effect sizes were found for mental health (p < 0.0001; d = 0.6), flourishing (p < 0.0001; d = 0.63), and negative affect (p < 0.0001; d = 0.68) at 1 month. Small effect sizes were obtained for physical health, stress, positive affect, self-efficacy, spirituality, and mysticism at 3 months. In a sensitivity analysis, the strongest effects at 1 month were found in the subgroup that completed per-protocol (n = 140), followed by those with complete data at all time points (n = 159). Effects were lowest in the intention-to-treat analysis (n = 359). The content of the course was positively evaluated by the participants.
Conclusions:
The online meditation course based on the expansion method had potentially beneficial effects, especially on mental health parameters. Based on the feasibility results, further research using randomized controlled designs is warranted.
Clinical Trial Registration:
NCT04950543.
Introduction
Globally, the number of disability-adjusted life years due to mental illness increased from 80.8 to 125.3 million between 1990 and 2019. 1 During the COVID-19 pandemic, the situation regarding mental health has further deteriorated. 2,3 In Germany, 20% of incapacity to work per person and year is caused by psychological complaints such as depression, anxiety, and stress disorders. 4
The German Federal Institute for Occupational Safety and Health estimates the associated costs at EUR 39 billion annually. 5 Most likely, the boundaries between mental stress and medically relevant complaints will continue to blur.
In resilience research, it is assumed that the body's stress response does not depend on the type of stressor, but rather on the perceived need for an adaptive response. 6 Resilience is not a fixed behavioral component but can be improved as a skill through training, for example, by meditation practice. 7,8 Whether coping strategies (“coping behavior” in ref. 9 ) can be implemented in everyday life depends on the individual's self-efficacy conviction. 9
Thoughts and feelings affect health, especially at the psychoneuroimmunological level. 10,11 Meditation shows robust efficacy in improving mental and physical health despite great heterogeneity in applied techniques and study populations. 12 Structured meditation programs have shown improvements in function and Health-Related Quality of Life (HRQoL) in people with chronic diseases. 13 –15 The effectiveness of meditation and mindfulness methods is also well documented in moderate depression and anxiety disorders. 16 This gives patients the opportunity to actively influence their health management. 17
Due to the COVID-19 pandemic, the interest in digitally supported health care has increased, especially online-based meditation methods. 18,19 Scientific investigation has also increased in the field of mindfulness practice through mobile applications. 20 Compared with the large number of treatments on offer, however, the evidence on effectiveness is still slightly lacking. 21
In respect to the large number of meditation interventions, systematic research, especially in online settings, is a useful contribution to meditation research. The expansion method is an innovative mind-body technique that makes use of meditation and guided introspection. The basic idea of this method is to retrieve and expand the feeling of positive emotions from memory. 22,23 The origin of the expansion method lies in different traditions, supplemented by aspects of positive psychology.
The aim of this study is a first evaluation of the effects of a 21-day online meditation course based on the “expansion method” in adults.
Materials and Methods
Study design and setting
In this prospective, uncontrolled observational study, the within-group effects † of a 21-day online meditation course were examined. The target parameters were assessed at baseline (V0), after 1 month (V1), and after 3 months (V2). The first patient was enrolled on July 7, 2021, and the last patient completed the study on October 17, 2021.
Validated questionnaires were used in German and English-language versions. The participants could choose whether they wanted to fill out the questionnaires in German or English. The questionnaires were filled out online via Limesurvey, hosted on Charité servers. The study was conducted at the Charité Outpatient Center for Complementary and Integrative Medicine at Immanuel Hospital Berlin, Germany, and the Department of Internal and Integrative Medicine, Evang. Kliniken Essen-Mitte, Essen, Germany.
It was approved by the ethics committee of the Charité—Universitätsmedizin Berlin (EA1/327/20) and registered at ClinicalTrials.gov before patient recruitment. The study was conducted and reported according to the Observational Studies in Epidemiology (STROBE) Statement. 24
Recruitment
Potential study participants were contacted via a cross-content online recruitment campaign on the course registration website. Participants were recruited from July 7 to July 14, 2021 (Table 1). The course was advertised internationally as a 21-day meditation challenge. Participation in the study was voluntary. Before being enrolled in the study, participants gave their informed consent for the collection of study-related data.
Eligibility Criteria
Outcome measurement and data collection
Sociodemographic data on the participants and data on chronic disease were collected. For the evaluation of all exploratory endpoints, validated questionnaires were used. Besides these, self-developed questions assessed lifestyle, course concept, and adverse events.
Validated questionnaires
We assessed self-reported HRQoL using the PROMIS 29 + 2 profile v2.1 and calculated the PROMIS Preference Score as well as the seven subscores: physical function, emotional distress (anxiety and depression), fatigue, sleep disturbance, the ability to participate in social roles and activities, and an attached pain scale. 25,26
To measure global health, we used the PROMIS 10-item Global Health Scale (PROMIS Scale profile v1.2) with the subscales physical (GH physical) and mental health (GH mental). 27 The subscales consist of four items, and two additional items provide independent scores to estimate pain interference and fatigue.
The Perceived Stress Scale (PSS) is a 4-item self-report instrument that assesses the perception of stress in the past month. 28
Affect regulation was measured using the Positive and Negative Affect Schedule (PANAS). 29 Positive affect regulation (PA) and negative affect regulation (NA) are covered by 10 items, each consisting of adjectives that describe different sensations and feelings. The construct validity is based on the agreement of the subscales with the personality traits extraversion and neuroticism from the Big Five taxonomy of personality psychology. 30
Psychological well-being/flourishing was assessed via a short 8-item measurement tool, the Flourishing Scale (FS). 31,32
Using the Short Scale for Measuring General Self-Efficacy Beliefs (ASKU), competence expectations in everyday life were reported. 33 At the core of the unidimensional construct, which goes back to Bandura (1977), is the self-belief of solution-oriented thinking and acting in critical situations. 9,34,35
The Gratitude and Awe Questionnaire (GrAw) is a 7-item instrument for measuring experienced spirituality. 36
The Connor-Davidson Resilience Scale (CD-RISC) includes 10 items. 37,38 Resilience regulates the perception of stress and promotes recovery and adaptation processes concerning psychological symptoms.
For the measurement of various Aspects of Spirituality (ASP), a short version of the questionnaire with 25 items was used. 39 A distinction is made between the four subscales: religious orientation (ASPro), search for insight/wisdom (ASPsiw), conscious interactions (ASPci), and transcendence conviction (ASPtc). The questionnaire can be used for various spiritual orientations, as well as in secular societies.
Hood's Mysticism Scale (M-Scale) in the 8-item version enables a differential assessment of mysticism and its relation to spirituality. 40,41 The definition of spirituality is based on a cross-cultural study conducted in the United States and Germany. 42,43 The questionnaire consists of the three subscales: introvertive mysticism (M-Intro), extrovertive mysticism (M-Extro), and interpretation (M-Inter).
Lifestyle parameters
General lifestyle parameters were collected using self-developed questions at all three measurement points (Supplementary Material S1). These can be clustered into the consumption of everyday drugs, exercise behavior, and previous experiences with relaxation methods. The questions refer to the behavior in the month before the respective measurement point to discover a possible modification of the effects. In addition, any previous experience of the participants with the expansion method was queried.
Evaluation of the course concept and adverse events
The fulfillment of expectations, whether the content was considered helpful or implemented as a coping strategy in everyday life, was assessed on a Numeric Rating-Scale (NRS) from 1 (not at all) to 6 (very). In the same way, the extent to which participants liked the challenge and their motivation to repeat the online course were documented. Moreover, adverse events were systematically assessed during the study period.
Description of the 21-day online meditation course
The content of the course consists of daily changing topics, with lessons of 25–40 min in total on theoretical background and guided meditation in the “expansion method” delivered via audio (in ref. 44 and Supplementary Material S2). 44 As with the questionnaires, participants could choose whether to take the whole course in German or English. The practice of expansion is taught through focusing, mindfulness, breathing, and visualization exercises.
In five repetitive steps, the manifestation of the memory of a positive feeling is extended beyond physical boundaries. These five steps are: the imagination of a shape, an image, and a color, the recreation of a general sensation, and the assignment of a label. A reminder email was sent to the participants daily. For the accompaniment of the participants, there is a procedure for dealing with psychological emergencies.
Through an online forum, there was the possibility of a common exchange of experiences, which was supervised by a qualified person. If the problems cannot be clarified in writing, a free therapeutic conversation is offered. The cost of participation in the course was EUR 21. Course fees were charged to cover the costs of creating the concept and digitizing it and had to be paid by the participants themselves. The expansion method has been used for self-practice, in coaching and therapy, for about 10 years.
Statistical methods
The study was designed to include 270 participants, so 300 participants were planned to be enlisted to allow for a dropout of 10%. Given an α = 0.025 for a two-sided t-test, β = 0.20, corresponding to a power of 80%, the sample size of 270 is sufficient to detect all effects with an effect size of Cohen's d > 0.20 (G*Power version 3.1).
All tests were conducted in a purely exploratory manner, with p-values <0.05 indicating “exploratory significance”; thus, no alpha adjustment to correct for multiple testing was applied. In explorative studies, outcomes with p < 0.05 are taken to indicate results that qualify for further testing (first in a pilot study, then possibly in an randomized controlled trial [RCT]). We further highlight that the results obtained here (p < 0.05) cannot be considered as confirmatory evidence.
For the main analysis, data from patients with complete cases in the first two visits (V0 and V1) were evaluated.
In the subsequent sensitivity analyses, results for three further (sub)groups are presented: (1) patients who participated in all three visits (V0–V1–V2), that is, complete cases for all three visits, (2) patients who participated in all three visits (V0–V1–V2) and had also completed all course sections within the first month (per-protocol group). And finally, for further research purposes, (3) the results of the intention-to-treat analysis are also enclosed. For the latter, incomplete data sets were imputed by a multiple imputation method (miceforest v5.6) using Python (version 3.7). This led to a complete set for the entire study population (n = 359) across all three visits (V0, V1, V2).
In the context of the evaluation of the validated questionnaires, in all analyses paired t-tests were calculated using R-Studio (version 4.1.2). Results are presented in the tables with means and standard deviations for the visits, and a 95% confidence interval for the observed change between the visits. t-test results are described by the probability value (p) and Cohen's d as an effect size—with the anker values of 0.2, 0.5, and 0.8 indicating small, medium, and large effects. 45
Chi-squared tests were employed to investigate whether participants changed their behavior in respect to lifestyle parameters such as consumption of alcohol and cigarettes, their engagement in regular sports (general, endurance, and weight training) in particular, and their practicing of relaxations techniques and meditation.
Finally, subgroup analyses were conducted for three parameters: GH mental, FS and NA for subgroups defined by gender (male vs. female), country of residence (the German-speaking countries Germany and Austria) versus other countries (UK and U.S.), whether participants had previous experience with the expansion method (yes vs. no), and whether participants had additionally practiced during the course participation (yes vs. no). For these, individual changes (differences) were calculated between V0 and V1 and compared across subgroups using t-tests.
Results
Study participants
A total number of 374 participants registered online for the study (Fig. 1). n = 14 people did not enter any data and were not included in the analysis, and another person did not meet the inclusion criteria because of their age and was also not included, leaving the data from 359 participants to be included in the study. Of these, 68% (n = 244) filled out V1 and 46% (n = 159) filled out V2. Data from 244 participants (complete cases) were included in the main analysis for the pre-post comparison (V0–V1).

Flowchart. Parameters were assessed at baseline (V0), after 1 month (V1), and after 3 months (V2).
Subgroups of the sensitivity analysis
Sociodemographic data
In the main analysis (CC V0–V1; n = 244), 84% (n = 205) were female, with a mean age of 51 ± 11 years, ranging from 23 to 82 years (Table 2). The mean body mass index of the study population was 24 kg/m2, which corresponds to normal weight. Most of the study participants resided in Germany (88.9%; n = 217), and 15 other participants (6.1%) were from Austria. Two hundred thirty-four (95.9%) participants completed the questionnaires in German.
Sociodemographic Data by Subgroups
If the numbers do not add up to 244 participants (100%), the differences are due to rounding errors or missing data.
CC (V0–V1), complete cases V0 (baseline)−V1 (1 month); CC (V0–V1–V2), complete cases V0 (baseline)−V1 (1 month)−V2 (3 months); ITT, intention to treat; n = number of subjects; PP, per-protocol.
Sixty percent (n = 147) of the participants lived in family relationships and almost half (44.3%; n = 108) were married. Fifty-nine percent (n = 144) of the participants stated having children. Regarding educational level, over half of the participants were academics (55.3%; n = 135), and the largest proportions were either self-employed (34.8%; n = 85) or fully employed (24.6%, n = 60).
Despite the high average age of 51 years, only a very small percentage (3.7%; n = 9) were unemployed. The monthly net income of 30% (n = 72) of the study participants was between EUR 2001 and 3000. Further sociodemographic data are shown in Table 2.
The sociodemographic data of the sensitivity analysis did not differ significantly from those of the main analysis (V0–V1; n = 244) (Table 2).
Chronic diseases
In the main analysis (CC V0–V1; n = 244), a total number of 129 (52.9%) participants suffered from chronic diseases (Table 3). Of these, 29% were physical and 21% were mental disorders. Affective disorders stood out with a relatively high percentage, above all depression (10.2%; n = 25). Anxiety disorders accounted for 6% (n = 14) of mental illnesses. This was followed by hypertension (5.7%; n = 14), as well as chronic pain (4.9%; n = 12) and lung diseases (4.9%; n = 12). One person reported abusing substances. Six people (2.5%) did not provide any information about their health status.
Chronic Diseases by Subgroups
N.A., no answer.
Within the sensitivity analysis, the prevalence of chronic diseases is almost comparable to the main analysis (Table 3).
Main analysis of the validated questionnaires (CC V0–V1; n = 244)
Medium effect sizes occurred for GH mental (T = 4.81; p < 0.0001; d = 0.6), FS (T = 9.9; p < 0.0001; d = 0.63), and NA (T = 10.65; p < 0.0001; d = 0.68) (Table 4, Fig. 2).
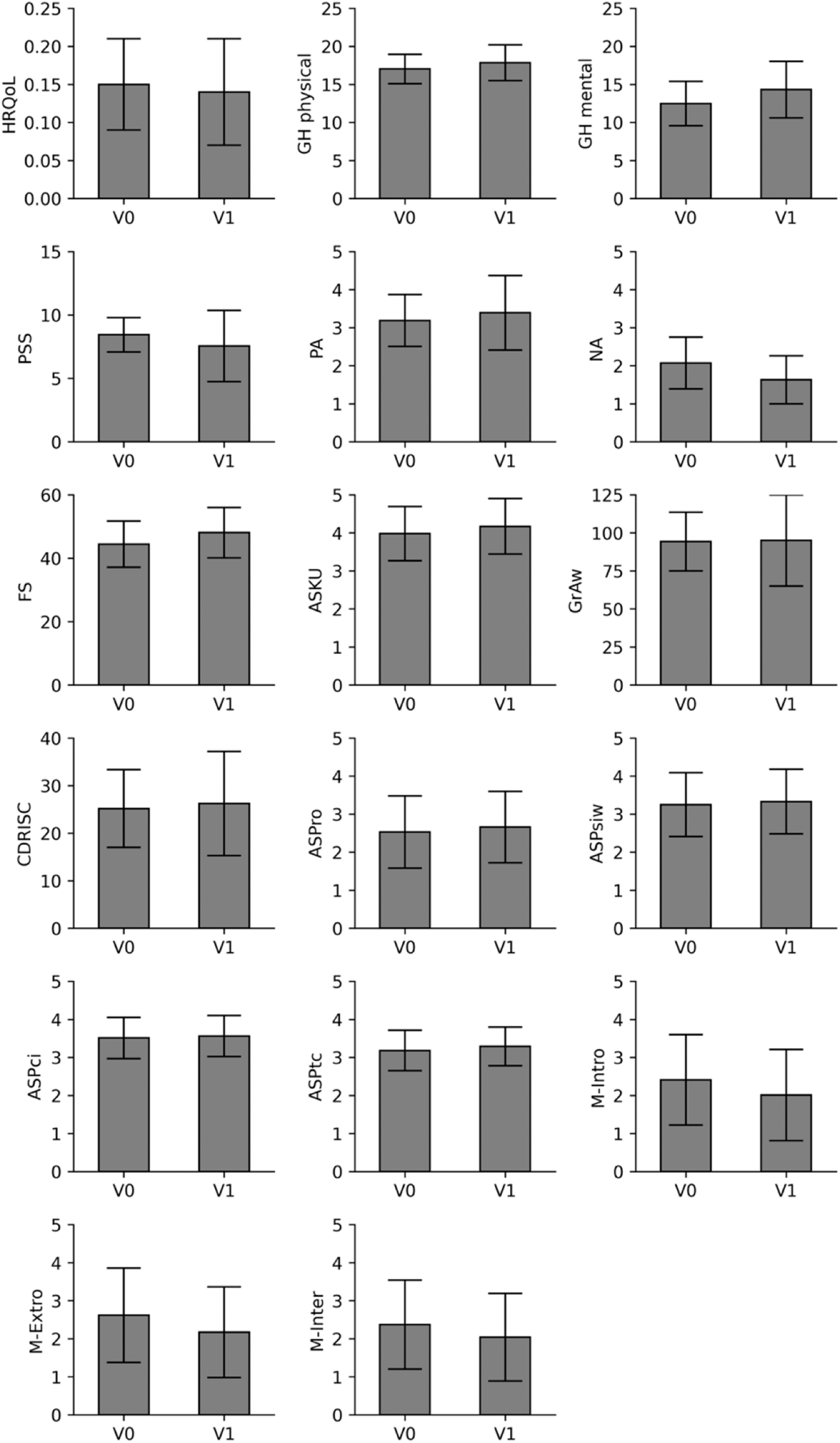
Multiplot of the main analysis of the validated questionnaires (CC V0–V1; n = 244). ASKU, Short Scale for Measuring General Self-Efficacy Beliefs; ASP, Aspects of Spirituality (ASPro, religious orientation; ASPsiw, search for insight/wisdom; ASPci, conscious interactions; ASPtc, transcendence conviction); CD-RISC, Connor-Davidson Resilience Scale; FS, Flourishing Scale; GH physical and GH mental, PROMIS Scale profile v1.2; GrAw, Gratitude and Awe Questionnaire; HRQoL, PROMIS 29 + 2 profile v2.1; M-Scale, Hood's Mysticism Scale (M-Intro, introvertive mysticism; M-Extro, extrovertive mysticism; M-Inter, interpretation); PA and NA, Positive and Negative Affect Schedule; PSS, Perceived Stress Scale.
Main Analysis of the Questionnaires (CC V0–V1; n = 244)
ASKU, Short Scale for Measuring General Self-Efficacy Beliefs; ASP, Aspects of Spirituality (ASPro, religious orientation; ASPsiw, search for insight/wisdom; ASPci, conscious interactions; ASPtc, transcendence conviction); CD-RISC, Connor-Davidson Resilience Scale; FS, Flourishing Scale; GH physical and GH mental, PROMIS Scale profile v1.2; GrAw, Gratitude and Awe Questionnaire; HRQoL, PROMIS 29 + 2 profile v2.1; M, mean value; M-Scale, Hood's Mysticism Scale (M-Intro, introvertive mysticism; M-Extro, extrovertive mysticism; M-Inter, interpretation); PA and NA, Positive and Negative Affect Schedule; PSS, Perceived Stress Scale; SD, standard deviation.
Small effect sizes were obtained for GH physical (T = 7.07; p < 0.0001; d = 0.45), PA (T = 3.27; p = 0.0012; d = 0.21), ASKU (T = 4.87; p < 0.0001; d = 0.31), and PSS (T = 4.81; p < 0.0001; d = 0.31). Small effect sizes also occurred in three of the ASP subscales: ASPro (T = 4.77; p = 0.0031; d = 0.31), ASPsiw (T = 3.19; p = 0.0016; d = 0.20), ASPtc (T = 3.74; p < 0.0002; d = 0.24), and in all three subscales of the M-Scale: M-Intro (T = 7.04; p < 0.0001; d = 0.45), M-Extro (T = 7.06; p < 0.0001; d = 0.45), and M-Inter (T = 5.42; p < 0.0001; d = 0.35).
No effects were found in HRQoL, GrAw, CD-RISC (non-significant), and ASPci (p = 0.0314).
Sensitivity analysis of the validated questionnaires (V0–V1–V2)
CC analysis (n = 159)
In the CC analysis, medium effect sizes occurred significantly in GH mental, PA, FS, and NA at V0–V1 (Supplementary Material S3, Table 1).
Significant differences with small effect sizes were found in GH physical, PSS, ASKU, GrAw, CD-RISC, and all subscales of ASP and the M-Scale (V0–V1).
Compared with the main analysis (n = 244), one medium and two small effects were added. Compared with the second measurement point, at V2 the medium effect size in NA remained stable.
PP analysis (n = 140)
In the PP analysis, significant differences with medium effect sizes were found in GH mental, PA, NA, FS, GrAw, and CD-RISC at V0–V1 (Supplementary Material S3, Table 2).
Small significant differences occurred in GH physical, PSS, and ASKU, in two of the subscales of the ASP (ASPsiw and ASPci), and in all subscales of the M-Scale (V0–V1).
Compared with the main analysis (n = 244), three more medium effect sizes occurred and two fewer small effect sizes. Compared with the second measurement point, at V2 all medium effect sizes decreased.
ITT analysis (n = 359)
In the ITT, there was only one significant difference with a medium effect size at V0–V1 in NA (Supplementary Material S3, Table 3).
Small significant differences developed in GH physical and GH mental, PA, FS, ASKU, and CD-RISC (V0–V1).
Compared with the main analysis (n = 244), there were two fewer medium and four fewer small effect sizes. Compared with the second measurement point, at V2 the medium effect in NA and the non-significant effect in GrAw became small effects. In the imputed ITT dataset, effect sizes were the smallest compared with the other analyses.
Subgroup analyses
Subgroup analyses were conducted for the following three parameters: GH mental, FS, and NA. However, results show that there are no significant subgroup differences for (1) gender (male vs. female), (2) the country of residency as this may have indicated both differences in culture or language (Germany and Austria vs. other countries, comprising the United Kingdom and the United States), (3) whether participants had previous experience with the expansion program, or not, or finally (4) whether participants had additionally practiced during the intervention period, or not (Table 5).
Subgroup Analyses for Selected Questionnaires (CC V0–V1; n = 244)
Δ V0–V1, differences between V1 and V0 scores; Additional practice, additional practice of the expansion method; Country, country of residence; D & A, German speaking countries Germany and Austria; GH mental, PROMIS Scale profile v1.2; m and f, male and female participants; p, p-values of the interaction between subgroups; Prev exp, previous experience with the expansion method; y and n, yes and no.
Summary of all results of the validated questionnaires
In summary, across all analyses, we found stable effects for the parameters GH physical, ASKU, and NA. The strongest effects across three of the analyses (main analysis, CC V0–V1–V2, and PP) were in GH mental, FS, and NA at V1. PA remained stable across two of the analyses (CC V0–V1–V2 and PP). GrAw and CD-RISC were only present in the PP analysis with a Cohen's d over 0.5 (medium effect size).
Lifestyle parameters
Everyday drugs tended to play a subordinate role in the study population (n = 244) (Table 6). Sixty-eight participants (27.9%) stated that they had consumed alcohol weekly in the month before baseline. The proportion of those consuming alcohol decreased from n = 68 (27.9%) to n = 55 (22.5%), corresponding to a decrease of 5.3% points (non-significant).
Lifestyle Parameters
p, p-value from x2 -test (df = 1, n = 244).
Quantitatively, alcohol consumption decreased on average from 5.6 (±5.9) to 4.7 (±3.5) drinks per person per week (with one drink referring to 0.25 L beer, 0.1 L wine, 0.1 L sparkling wine, or 0.04 L of spirits). This is an average of one alcoholic drink per week less after course participation (V1).
n = 31 (13%) of the participants stated that they had smoked cigarettes in the previous month. During the course, the number of smokers remains almost the same (n = 28). Quantitatively, however, a difference can be seen. While 275.2 cigarettes were smoked in the month before the study, which is a mean of 8.9 (±6.9) per person, 25.7 (9.34%) fewer cigarettes were smoked during the study (not significant). The number of smokers declined only slightly, and cigarette consumption by the remaining smokers remained about the same.
More than half of the population (55.7%; n = 136) did sports regularly, with endurance sports being preferred at 43% (n = 105). Over the course period, 12 participants (+4.9%) had done more endurance sports. The increase in total sports was significant (p = 0.035).
Around a fifth of the participants (23.4%; n = 57) had previous experience with the expansion method and had been practicing it for an average of 3 years (3.4 ± 4.8). n = 50 of these participants practiced the expansion method in the month before baseline. Fifty percent (n = 123) of participants reported having repeated the content outside of attending the course itself (V0–V1), with an average duration of 86 min per week (±119.9 min).
Sixty-three percent (n = 154) practiced further relaxation techniques during the course participation. Fifty-five percent (n = 133) of them practiced other forms of meditation alongside the course, which corresponds to an average effort of 2 h per week. The performance of relaxation procedures, excluding the expansion method, in the previous month decreased from V0 to V1 by 6.2% and by 8.6% percent only for meditation (not significant).
Evaluation of the course concept and adverse events
The expectations of the course concept were met for the majority of the participants (4.6 ± 1.4 on a 1–6 NRS; 1 = not at all to 6 = very) (Fig. 3). Most participants considered the course content helpful (5.1 ± 1.2 on a 1–6 NRS), and almost as many used the content as a coping strategy in everyday life and reported a positive impact (4.4 ± 1.5 on a 1–6 NRS). Almost all participants liked the challenge (5.1 ± 1.3 on a 1–6 NRS) and were motivated to repeat the course (5.0 ± 1.3 on a 1–6 NRS). Overall, this indicates rather strong to very strong agreement.
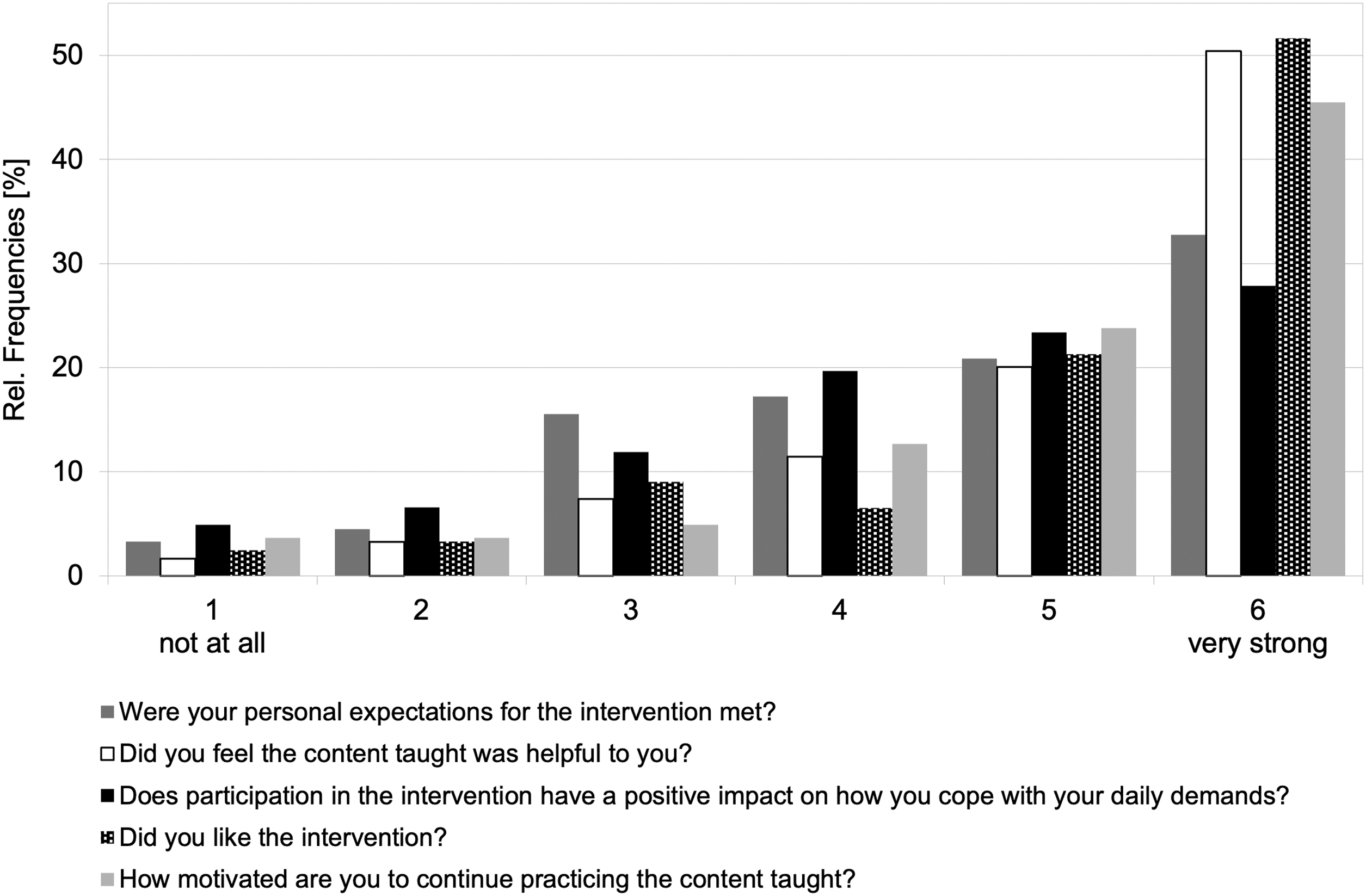
Feedback on the course concept.
No physical or psychological harms or adverse events related to course participation were reported. There were also no psychological emergencies reported via the online forum.
Discussion
This study aimed at investigating the effects of the 21-day online meditation course based on the innovative “expansion method.” The study started at the beginning of the third wave of the COVID-19 pandemic in 2021. The COVID-19 pandemic had a significant impact on quality of life and especially mental health parameters. 46 –48 The study participants were predominantly women aged 45+, with a higher level of education belonging to the middle-income group in Germany. 49
In the main analysis, improvements in GH mental, NA, and FS showed medium effect sizes. The strongest effects occurred within the PP analysis (GH mental, PA, NA, FS, GrAw, and CD-RISC). With only one medium effect, the smallest effects were detected in the ITT analysis. During the follow-up period, all but one (ITT: GrAw) of the effects were stable (CC: NA, GH physical, PSS, ASKU, ASPro, M-Intro, M-Extro, HRQoL) or decreased (CC: GH mental, FS, PA, GrAw, CD-RISC, ASPsiw, ASPci, ASPtc, M-Inter).
Comparison of study results
Due to the different measurement instruments, contents, and timeframes of courses, the effects are only comparable to a limited extent.
Russell et al. reported a slightly lower number of female participants in their study (75% female). 50 Women with a higher income, and health-focused lifestyles are more likely to use meditation interventions than men. 51,52 Women are also more likely to seek emotional support; given mind-body interventions focus on emotion regulation, these interventions may intuitively have a greater appeal to women. 50
While in other studies women benefited slightly better from meditation, in this study no significant differences by gender could be demonstrated for the expansion method. 12 However, the low number of male participants (n = 35) must be taken into account. In difference to other studies in the field of online meditation, the mean age of the study population is 10 years above average (mean age of 40 years). 20 With an age range of 23–82 years, the expansion method is adopted by more age groups compared with the currently best evaluated mindfulness programs (age range: 18.73–57.6). 53
Compared with Sommers-Spijkerman's study, the expansion method stands out from the results of other recent developments of digital meditation interventions in the field of mental health. 20
Flett et al. examined the efficacy of two mindfulness meditation apps, Headspace (n = 72) and Smiling Mind (n = 63), in students. 54 In the pre-post comparison, small effects were found for depression (Center for Epidemiological Studies-Depression Scale [CES-D]), anxiety (Hospital Anxiety and Depression Scale-Anxiety Subscale [HADS-A]), stress (PSS), and resilience (brief resilience scale) (Smiling Mind only). The amount of exercise included 10 min each day for 10 days.
In comparison to both apps, the expansion method (n = 244) showed pronounced effects after 21 days in mental health and flourishing. The effects on stress perception and resilience are comparable to the results for Headspace. While app adherence was comparatively high during the study period (80% participation), the number of participants for both apps dropped to about half during the continued access period of 30 days. Despite the comparable scope of the courses and number of participants, the study of Flett et al. differs in study design (RCT) from the exploratory approach of the EXPAN study.
Feasibility
The response of 68% at V1 is comparable to other digital applications, and in some cases even above average. 55 Neither lifestyle nor chronic diseases differed strongly enough among subgroups to explain the dropout rate. While Internet-supported mindfulness-based interventions have been shown to be more effective over supervised groups, the lack of adherence is a well-known problem. 50 Based on the positive feedback from participants regarding the course content, the dropout rate is likely due to the usual reasons for online interventions and the uncertain situation during the pandemic. A clearly defined study population, the possibility of digital interaction, and personalized adaptation can reduce dropout and increase effectiveness. 56,57
Other possible explanations for lack of adherence include the short-term lifestyle changes involved in the study, which required about 30 min of effort per day, and participants' lack of commitment to a specific person or institution. 58 The time required for the numerous questionnaires in this study must also be taken into account. Better compliance may lead to better effects. 55
Limitations
This study allows for only exploratory findings, as no control group was established. The results showed only initial but promising indications of beneficial effects. However, all considerations must be made very cautiously. Possible biases are present due to: gender, age, (high) meditation practice, familiarity with content, and lack of adherence.
Based on the results of the ITT analysis, the effects of the further analyses may have been overestimated. 59 However, the large number of imputed data (54%) within the ITT analysis must be considered when interpreting the results. At V1, 32% of the participants who completed the questionnaires dropped out of the study. Ultimately, at the end of the study, the dropout rate was 56%.
The homogeneous distribution of the sociodemographic data and chronic diseases does not suggest an emigrative selection bias. The lifestyle of the participants, including the practice of further relaxation methods, did not differ much before and during the investigated course. Neither the increased practice of endurance sports nor the small decrease in everyday drugs can be attributed exclusively to a positive effect due to course participation.
The restrictions in gastronomy and social life, as well as more flexible working hours due to the pandemic, could explain the results. Almost a quarter of the participants already knew the method for up to 3 years. This may have influenced the reported results (selection bias). However, the subgroup analyses for the three clinically relevant effects (GH mental, FS, and NA) showed no significant subgroup differences regarding gender, country of residence, language, previous experiences, and additional exercises besides the course. A modification of the effects cannot be assumed.
Due to the freedom of choice in which language the participants filled in the questionnaires and selected the course content, a language bias cannot be completely excluded. Since 232 participants live in German-speaking countries and almost as many questionnaires (n = 234) were filled out in German, a distortion of the results due to a lack of language skills is very unlikely.
The fact that the method was used by half of the participants outside of the sessions could be in favor of the method, but also presents a difficulty for evaluation that should be considered in future studies. Practicing the expansion method in addition may have had an additional positive impact on the results.
Adverse events or psychological emergencies related to the content were not recorded. However, a warning of potentially triggering content was not given beforehand, which we would recommend for subsequent study.
Interpretation and generalizability
The positive effects on GH mental, FS, CD-RISC, and PSS suggest long-term effects of meditation in preventing stress-related illnesses. The composition of the study population in terms of gender, age, and experience with relaxation techniques must be considered when generalizing. Even if no significant differences were found in the subgroup analysis, the proportion of women and the age of the participants are slightly above the average for other mind-body medicine (MBM) interventions, as described earlier. 20
Possible reasons are a relatively high daily time expenditure, for example, for employees and parents.
The mindfulness meditations mentioned in the comparison are based on collecting new positive experiences and cognitive reappraisal. 60 With the expansion method, on the other hand, new experiences do not have to be had first. The method builds on already existing positive experiences and draws on the feelings associated with them. 22
The results of the PP analysis showed that regular practice of the expansion method could have a regulating effect in moments of distress. Especially the positive results in PANAS could be useful in therapy for affective disorders. The expansion of positive emotions may also lead to a decrease in psychological and endocrine responses to traumatic experiences. 61 –63
Although the additional subgroup analysis did not map evidence of differences between novice and advanced participants, possible effects should be further investigated in a methodologically high-quality study.
Conclusion
Despite the short duration of the course studied, this study provides promising initial evidence that the expansion method may be helpful in maintaining mental health and possibly building resources for personal development. Further studies—for example, with proof of effectiveness in the context of a larger RCT—are warranted. It will be important not only to choose an appropriate control group to demonstrate that the method works, but also possibly to show directly what particular advantages it may have over other methods.
How sustainable the possible effects are needs to be further investigated. Participants could use the content as coping strategies in their everyday lives and may in this way induce self-efficacy. Whether the presumed positive effects of course participation on mental health also led to improvements in lifestyle in general requires further investigation. Self-management support is one of the most sustainable goals in primary public health care.64
Footnotes
Authors' Contributions
H.M.F.: writing—original draft preparation, formal analysis, data curation, and visualization. F.J.S.: conceptualization, project administration, and writing—review and editing. S.S.: conceptualization, project administration, and writing—review and editing. H.H.: conceptualization, supervision, and writing—review and editing. H.C.B.: writing—review and editing. C.S.K.: writing—review and editing. J.K.: supervision, writing—review and editing. H.C.: supervision, project administration, and writing—review and editing. A.M.: supervision, writing—review and editing. F.I.K.: formal analysis, data curation, writing—review and editing, and visualization. M.J.: conceptualization, methodology, investigation, writing—review and editing, project administration, resources, and software. The authors do not have any conflict of interest with the content of the article. All authors approved the final version of the article.
Authorship Confirmation Statement
Guarantor of article: H.M.F., M.J.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work has been funded by HGC Total Human gGmbH, Berlin. The funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the article; or decision to submit the article for publication.
Supplementary Material
Supplementary Material S1
Supplementary Material S2
Supplementary Material S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.