
Abstract
Background:
Current treatments for osteoarthritis (OA) pain and stiffness have limitations, including adverse effects. Therefore, effective and safe complementary or alternative therapies are needed. Dietary supplement GJ 191, comprising Epimedium, Dioscorea, and Salvia miltiorrhiza extracts, may address this need.
Methods:
This randomized, double-blind, placebo-controlled study investigated GJ 191 supplementation on knee OA symptoms. Seventy-two adults (40–75 years) with mild to moderate knee OA and mild to moderate knee pain were enrolled. The Knee Injury and Osteoarthritis Outcome Score (KOOS), Pain Visual Analog Scale (VAS), Quality of Life questionnaire, knee joint range of motion, serum C-reactive protein, and rescue medication use were assessed. The Western Ontario McMaster Universities Osteoarthritis Index (WOMAC) pain and stiffness scores were computed using KOOS scores.
Results:
Decreases in WOMAC pain scores were reported by both GJ 191 and placebo groups after 6 (−1.78 ± 2.71 and −1.34 ± 1.93, respectively; p < 0.01) and 12 (−2.31 ± 2.83 and −1.59 ± 2.69, respectively; p < 0.01) weeks, with no significant difference between groups. There were decreases in WOMAC stiffness scores for participants supplemented with GJ 191 by 0.53 ± 1.22 and 0.72 ± 1.46 (p ≤0.02) after 6 and 12 weeks, respectively, with respective decreases of 0.81 ± 1.51 and 0.75 ± 1.85 (p ≤0.03) for those on placebo. Significant improvements in current pain, as assessed by the Pain VAS, and bodily pain were reported by the GJ 191 group after 6 and 12 weeks, while the placebo group only reported significant improvements in these measures after 12 weeks. GJ 191 supplementation was safe and well tolerated.
Conclusion:
There was no significant difference in pain and stiffness scores between GJ 191 and placebo over the 12 weeks. While both groups reported improvements in WOMAC pain from baseline, improvements in current and bodily pain were experienced sooner with GJ 191 than placebo and were sustained over the study period. GJ 191 supplementation was safe and well tolerated. (CTR#: NCT04395547).
Introduction
Knee osteoarthritis (OA) is a joint disorder caused by sustained wear and tear on the joint, leading to the breakdown of protective cartilage, 1 pain, stiffness, and unfavorable health, 2,3 and economic 4 outcomes. Approximately 19% of Americans ≥45 years of age are affected by knee OA, 5 accounting for 83% of the global burden caused by all OA types. 6 Current treatment options for OA include exercise, physiotherapy, pharmacotherapy, intra-articular injections, and surgery, which are effective, but have limitations to their use such as compliance, associated adverse events, cost, and risk of infection. 7 –9 Therefore, given these limitations, there is an increasing demand for effective and safer alternatives, such as natural health products with pain-relieving potential.
Epimedium, Dioscorea, and Salvia miltiorrhiza are plant extracts with bioactive compounds, which have individually shown potential to improve OA, 9 –13 both in vitro 10,13 –22 and in animal models. 20,23,24 Moreover, the combination of these ingredients improved symptoms in a preclinical model of OA. 25 Human studies that have orally administered these extracts individually or in combination have also shown improvements in knee OA symptoms. 26,27 However, further clinical investigation is warranted to better understand the potential favorable effects of these plant extracts on knee OA.
Therefore, the aim of this study was to investigate the effects of an Epimedium, Dioscorea, and S. miltiorrhiza extract formulation on knee OA symptoms and joint functionality in an adult population with mild to moderate knee OA and self-reported mild to moderate knee pain, who were otherwise healthy.
Research ethics board (Advarra, Aurora, Ontario) approval was granted in May 2020 and the final protocol was approved in January 2021 (Pro00043636).
Materials and Methods
Study design
This randomized, double-blind, placebo-controlled, parallel clinical trial was conducted at KGK Science Inc. (London, Canada) from June 2020 to March 2022. This study was registered with ClinicalTrials.gov (ClinicalTrials ID: NCT04395547).
Participants reported to the clinic at screening, baseline, week 6, and week 12 with touchpoints for compliance and participant questions at weeks 3 and 9. Screening assessments included blood for clinical chemistry and hematology, urine pregnancy test (females only), vital signs, anthropometrics, and completion of the Knee Injury and Osteoarthritis Outcome (KOOS) pain subscale to assess eligibility. Study assessments at baseline and weeks 6 and 12 included the KOOS, Pain Visual Analog Scale (VAS), Quality of Life (QoL) questionnaire, knee joint range of motion, serum C-reactive protein (CRP), vital signs, and anthropometrics. Blood was also collected for clinical chemistry and hematology at week 12.
Registration
This study was approved by the Natural and Non-Prescription Health Product Directorate, Health Canada, in April 2020. This study was conducted in accordance with the Declaration of Helsinki and its subsequent amendments, and in compliance with the International Council for Harmonization of Technical Requirements for Pharmaceuticals for Human Use (ICH) Guideline for Good Clinical Practice (GCP). The study followed the Consolidated Standards of Reporting Trials guidelines (Supplementary Table S1). 28
Participants
Participants were healthy adults 40–75 years of age with a BMI of 18.5–34.9 kg/m2, who had been diagnosed with mild to moderate knee OA, as confirmed by the Qualified Investigator (QI) based on physical examination and medical history. Participants also had self-reported mild to moderate knee pain, as assessed by a score of ≤75 on the KOOS pain subscale. All participants agreed to refrain from taking pain relievers for 48 h before study visits. Informed consent was obtained from participants before performing any study procedure including the screening process.
Individuals were excluded if they had an injury or intraarticular injections to the target knee within the past three and six months, respectively; had knee joint disease (e.g., rheumatoid arthritis), history of knee surgery; or used concomitant medications, supplements, foods, or drinks. Full details of inclusion and exclusion criteria can be found in Supplementary Table S2.
Investigational product and placebo
The investigational product (IP), GJ 191 (Chenland Nutritionals, Inc., Irvine, CA), comprised Epimedium extract (190.1 mg), Dioscorea extract (114.6 mg), Salvia miltiorrhiza extract (13.7 mg), and magnesium stearate. GJ 191 consists of extracts from Epimedium brevicornum leaves, Dioscorea nipponica rhizomes, and Salvia miltiorrhiza roots and rhizomes in the proportions of 60%:36%:4%, respectively, and was extracted with ethanol and water. The placebo comprised dextrin and magnesium stearate. Participants were instructed to take one capsule in the morning and one in the evening with a meal. The study products were identical in appearance, including product bottles, which were labeled per the requirements of ICH-GCP guidelines and applicable local regulatory guidelines by unblinded personnel not involved in any study assessment.
Rescue medication use
Participants were permitted to take two regular strength acetaminophen (Tylenol, 325 mg, DIN: 00559393) if relief was not experienced two hours after taking the study product. If relief was still not experienced four to six hours after taking the initial dose of acetaminophen, participants were permitted to take another dose of two acetaminophen, and then again, every four to six hours, without exceeding nine in a 24-hour period. Rescue medication (RM) could be taken up to four hours before study product administration and use of acetaminophen was recorded daily.
Study outcomes
This study assessed change in knee joint function, as determined by change in pain or stiffness as co-primary outcomes from baseline to week 12 between GJ 191 and placebo, as assessed by the Western Ontario McMaster Universities Osteoarthritis Index (WOMAC) pain and stiffness scores calculated using KOOS. Secondary outcomes included WOMAC pain and stiffness scores after six weeks of supplementation, knee OA symptoms, daily physical function, physical function in sports and recreational activities, current pain, QoL, knee joint range of motion, CRP, and RM use. Safety outcomes included adverse events (AEs), vital signs, clinical chemistry, and hematology.
Study assessments
KOOS
The KOOS is a validated tool used to evaluate symptoms and functions of knee OA. 29 It comprises six subscales, including symptoms, stiffness, pain, function in daily living, function in sport and recreation, and QoL. The WOMAC pain and stiffness scores were computed according to the KOOS scoring instructions. 30
Pain VAS
The Pain VAS is a measure of pain intensity, which is commonly used for OA. 31,32 A horizontal line anchored by descriptors ranging from “no pain” to “as much pain as I can imagine” was used to measure current pain.
SF-36 QoL
The RAND SF-36 questionnaire is a set of easily administered QoL measures, including physical functioning, role limitations due to physical health, role limitations due to emotional problems, energy/fatigue, emotional wellbeing, social functioning, bodily pain, and general health that has been applied in OA research. 33
Knee joint range of motion
Participants were instructed to lay down in a supine position on the examining table. For the extension measurement, participants were asked to straighten their leg three times and the examiner measured the angle in degrees using the goniometer. For the flexion measurement, participants were asked to bring the foot as close as possible to their buttocks without using their hands. The examiner measured the angle in degrees using the goniometer. 34
CRP
Blood for CRP was inverted 5-6x and left to clot for 30 min, followed by centrifugation for 10 min at 2050 g at 25°C, and stored at −80°C. CRP was analyzed using particle-enhanced immunoturbidimetric assay by Dynacare (London, Canada) with a detection limit of 0.3–700.0 mg/L.
Safety
Safety was assessed by AEs, blood pressure, heart rate, clinical chemistry, and hematology. Clinical chemistry and hematology included standardized blood safety parameters of liver/kidney markers and complete blood count, respectively, and were analyzed using standardized procedures by Dynacare (London, Canada). AEs were recorded by participants in their study diary and at each study visit. The QI classified AEs using the Medical Dictionary for Regulatory Activities version 24.0.
Statistical analysis
A total sample size of 72 participants (36 per group), at 5% 2-sided significance level, was estimated to have 80% power to detect a difference in mean change in WOMAC pain score of 6.6 mm, between GJ 191 and placebo groups, assuming a 20% attrition rate and pooled standard deviations of 7.41 mm and 9.56 mm at baseline and week 12, respectively. 35 The same sample size, at 5% two-sided significance level, was estimated to have 80% power to detect a difference in mean change in WOMAC stiffness score of 2.5 mm, between GJ 191 and placebo groups, assuming a 20% attrition rate and pooled standard deviations of 2.73 mm and 3.72 mm at baseline and week 12, respectively. 35
All continuous data variables were evaluated for normality and log-normality using the Shapiro–Wilk test. Demographics were compared between groups using a two-sample t-test for continuous variables or a test of independence using Chi-square test for categorical variables. Depending on normality, between-group differences in outcomes were compared using a two-sample t-test or Wilcoxon signed-rank test. Changes from baseline to weeks 6 and 12 were analyzed using a paired t-test or a Wilcoxon signed-rank test. Fold changes and their 95% confidence intervals were calculated within groups between baseline and weeks 6 and 12 using the ratio of mean values. Use of RM was compared between groups for each time period using the z-test. Subgroup analyses based on BMI classification and KOOS pain score (moderate or mild) at baseline were conducted using an ANOVA or a Kruskal–Wallis Test. Data are presented as mean ± standard deviation (SD).
Results are reported for the per protocol (PP) population, which included participants who consumed at least 80% of study product, did not have any major protocol violation, and completed all study visits and procedures associated with the primary outcome. Probabilities <0.05 were considered statistically significant. All statistical analyses were completed using the R Statistical Software Package Version 3.6.3 or newer for Microsoft Windows. 36
Results
Study population
A total of 162 individuals were screened for eligibility and 72 adults with mild to moderate knee OA (n = 36/group) were randomly assigned to either GJ 191 or placebo groups (Fig. 1, Table 1). Eight participants were excluded from the PP population due to change in concomitant medication (n = 4), early termination (n = 2), <80% compliance (n = 1), and out of window study visit (n = 1), with four participants excluded from each group.
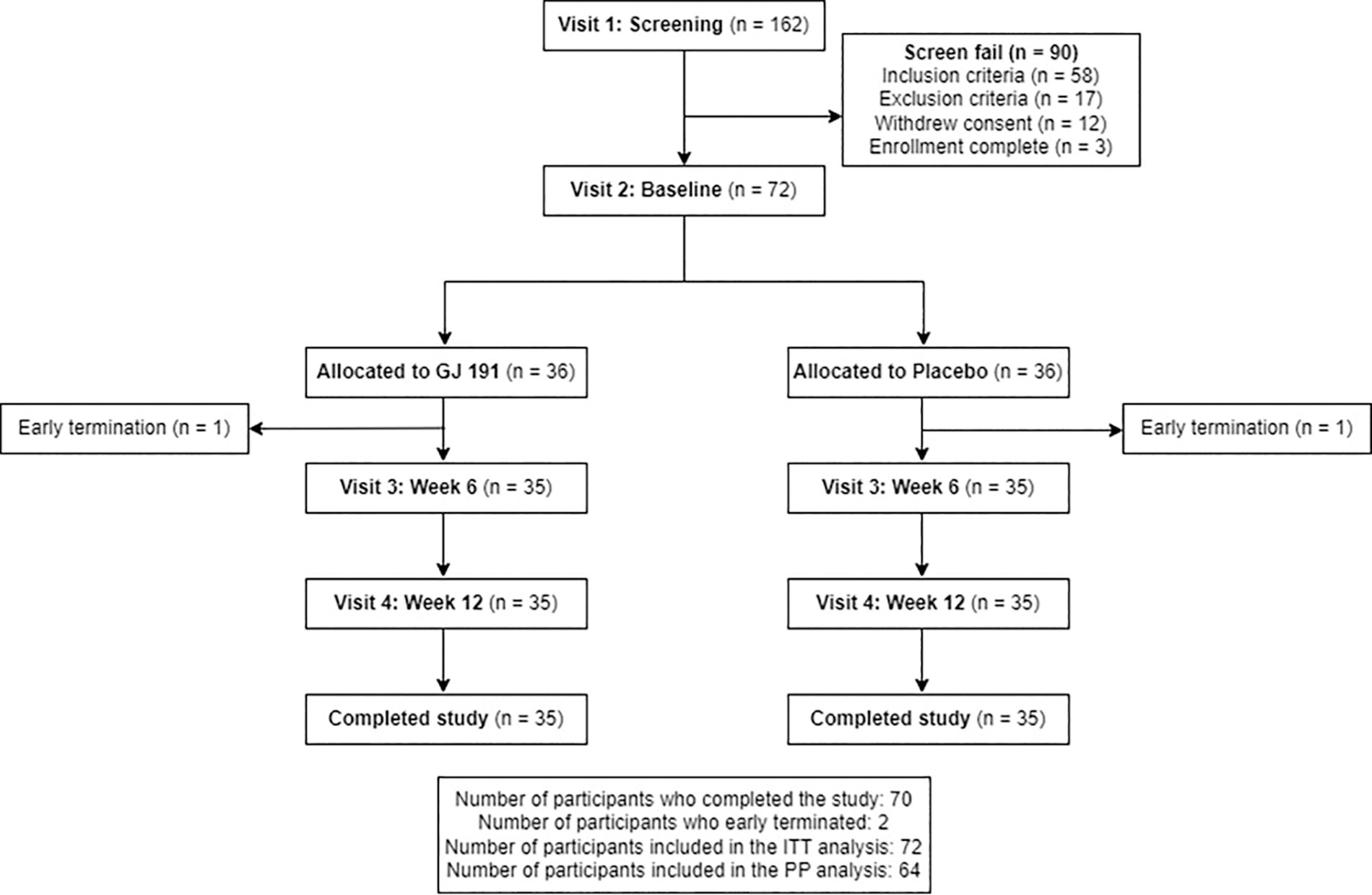
Disposition of study participants.
Demographic Information for Participants in the Per Protocol Population (n = 64)
n, number; SD, standard deviation.
*Two sample t-test. ** Test of independence using Chi-square test.
WOMAC
There was no significant difference in WOMAC pain or stiffness scores between groups. Participants in the GJ 191 and placebo groups reported significant decreases in WOMAC pain (Fig. 2) and stiffness scores (Fig. 3) from baseline to weeks 6 and 12. There was a 0.78-fold [95% CI: = 0.60–0.95] and 0.66-fold change [0.51, 0.81] from baseline to weeks 6 and 12, respectively, for WOMAC pain scores for participants supplemented with GJ 191. Those on placebo had a 0.81-fold [0.70, 0.92] and 0.76-fold change [0.61, 0.91] after 6 and 12 weeks for WOMAC pain scores. For WOMAC stiffness, there was a 0.94-fold [0.71, 1.18] and 0.90-fold change [0.62, 1.18] from baseline to weeks 6 and 12, respectively, for the GJ 191 group, with respective fold changes of 0.81 [0.65, 0.97] and 0.83 [0.66, 1.00] for the placebo group.

Change in WOMAC pain score (0–20) from baseline to weeks 6 and 12 for GJ 191 and placebo in the PP population (n = 64). All values presented are mean ± standard deviation (SD). * indicates statistically significant (p < 0.05) change from baseline. PP, per protocol; WOMAC, The Western Ontario McMaster Universities Osteoarthritis Index.
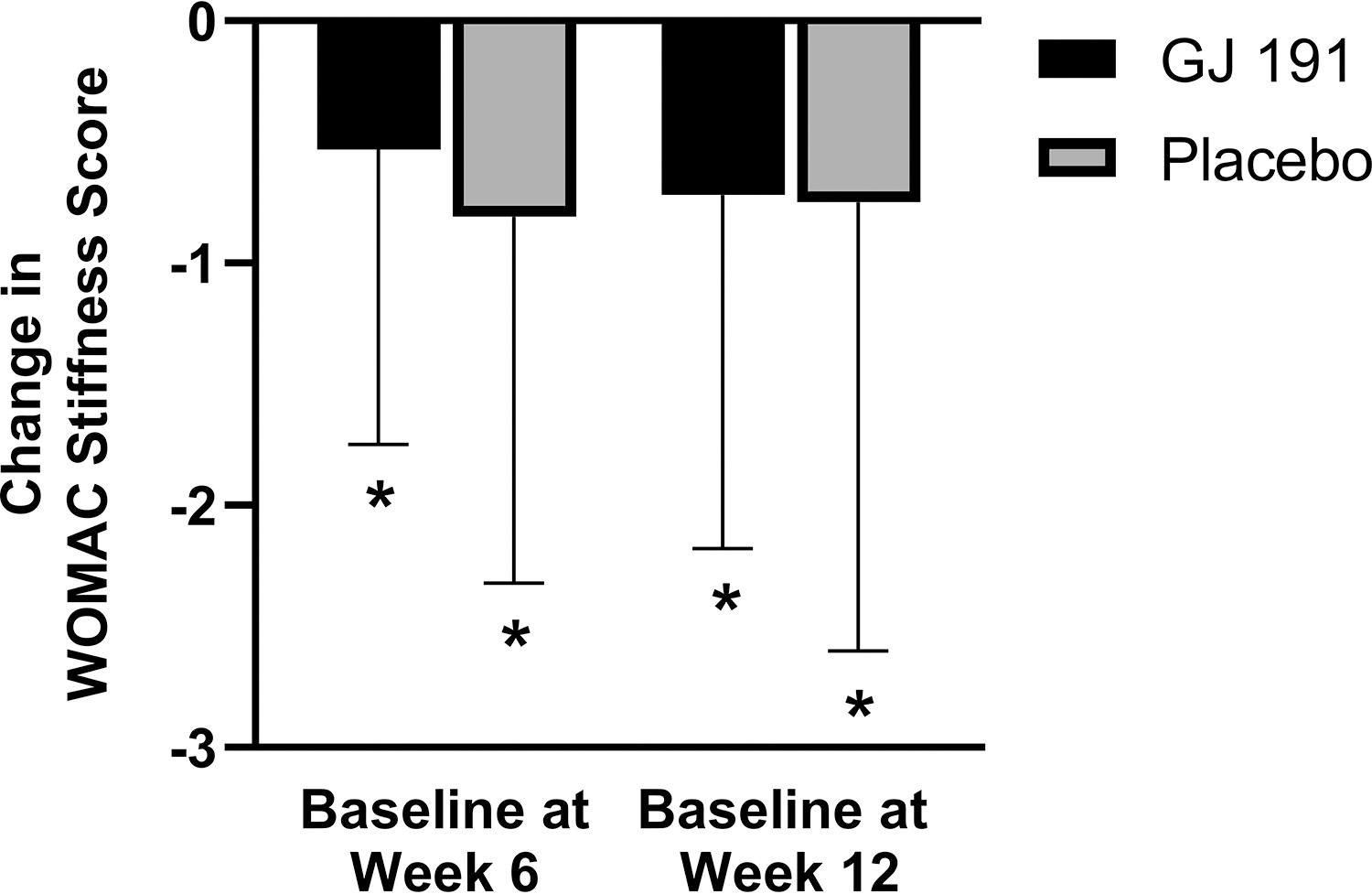
Change in WOMAC stiffness score (0–8) from baseline to weeks 6 and 12 for GJ 191 and placebo in the PP population (n = 64). All values presented are mean ± SD. * indicates statistically significant (p < 0.05) change from baseline. PP, per protocol; SD, standard deviation; WOMAC, The Western Ontario McMaster Universities Osteoarthritis Index.
Current pain
The GJ 191 group reported a significant decrease in current pain, as assessed by the Pain VAS, from baseline to week 6, whereas those on placebo did not (Fig. 4). Participants in both groups reported significant decreases in current pain from baseline to week 12 with those supplemented with GJ 191 reporting a greater decrease than placebo. There was no significant difference in current pain between groups at week 12.
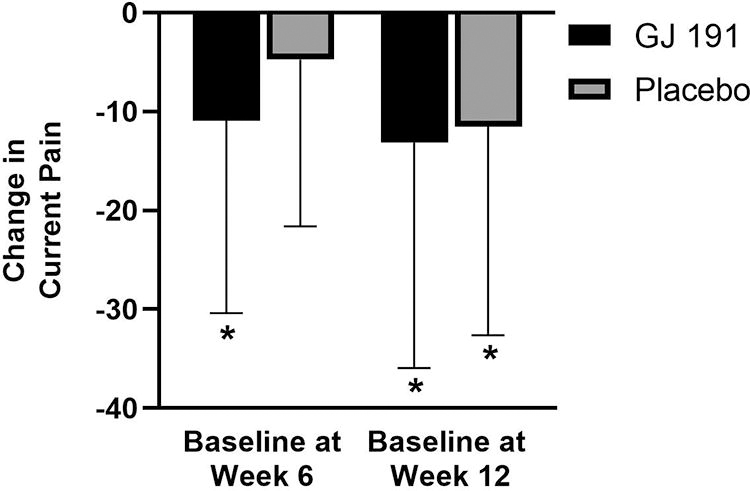
Change in current pain score, as assessed by the Pain VAS (0–100), from baseline to weeks 6 and 12 for GJ 191 and placebo in the PP population (n = 64). All values presented are mean ± SD. * indicates statistically significant (p < 0.05) change from baseline. PP, per protocol; SD, standard deviation; VAS, Visual Analog Scale.
KOOS
Participants in both groups reported significant increases in KOOS symptoms, function, daily living, and QoL from baseline to weeks 6 and 12 (Table 2). A total of 41% and 38% of participants in the GJ 191 and placebo groups, respectively, reached the MCIC for KOOS symptoms score at week 6. Similarly, 53% and 38% of participants in GJ 191 and placebo groups, respectively, reached the MCIC at week 12.
Change in KOOS Subscale Scores from Baseline to Weeks 6 and 12 for the PP Population (n = 64)
All values are mean ± SD.
p-value for change from baseline.
P-values for testing differences between groups were generated by the two-sample t-test on untransformed data or the two-sample t-test after log transformed data (lp) or the Wilcoxon signed-rank test (w) on untransformed data.
P-values for testing within-group difference were generated by the paired t-test after untransformed or the Paired t-test after log transformed (lp) or the Wilcoxon signed-rank test (w).
P-values considered statistically significant are indicated in bold font.
KOOS, The Knee Injury and Osteoarthritis Outcome Score.
Quality of life
Participants supplemented with GJ 191 reported a significant increase in bodily pain scores from baseline to weeks 6 and 12, with those on placebo reporting a significant increase at week 12, but not week 6 (Fig. 5). The GJ 191 group reported a significantly greater increase in role limitations due to physical health scores from baseline to week 6 compared to the Placebo group. There was no other significant difference between groups in QoL measures at week 6 or week 12, with the remaining QoL results presented in Supplementary Table S3.
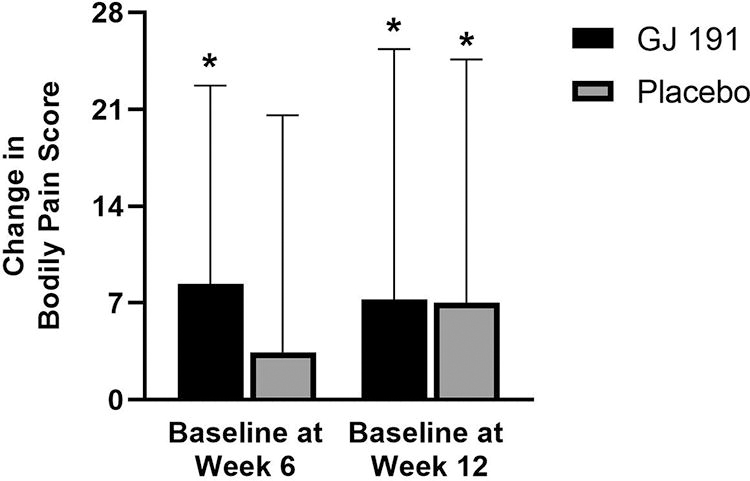
Change in bodily pain domain score (0–100) from the SF-36 QoL questionnaire from baseline to weeks 6 and 12 for GJ 191 and placebo in the PP population (n = 64). All values presented are mean ± SD. * indicates statistically significant (p < 0.05) change from baseline. PP, per protocol; QoL, Quality of Life; SD, standard deviation.
Knee joint range of motion and CRP
There was no significant difference in knee joint range of motion or CRP between groups nor was there any significant change from baseline to week 6 or 12 in the GJ 191 or placebo groups (data not shown).
Rescue medication use
There was no significant difference in RM use between participants supplemented with GJ 191 and those on placebo from baseline to week 6 (5.1% ± 0.09 vs. 4.2% ± 0.09). Participants in the GJ 191 group used RM on a significantly greater proportion of occasions, compared to those in the placebo group, from baseline to week 12 (5.6% ± 0.06 vs. 3.9% ± 0.06) and week 6 to 12 (6.0% ± 0.064 vs. 4.0% ± 0.06).
Knee pain subgroups
In a subgroup analysis based on knee pain at baseline, in the GJ 191 group, participants with moderate knee pain had a significant decrease in WOMAC pain scores at both weeks, whereas those with mild knee pain reported a significant decrease at week 12 only (Table 3). There were significant reductions in current pain scores reported by participants with moderate pain supplemented with GJ 191 at weeks 6 and 12, while scores for those with mild pain did not reach statistical significance (Table 3). There was no significant difference between GJ 191 and placebo for WOMAC pain or current pain scores in this subgroup analysis.
Subgroup Analysis Based on Pain from the PP Population (n = 64)
All values are mean ± SD; there was no statistically significant difference between groups for the primary outcome at week 6 or 12.
p-value for change from baseline.
P-values considered statistically significant are indicated in bold font.
VAS, Visual Analog Scale; WOMAC, The Western Ontario McMaster Universities Osteoarthritis Index.
BMI subgroups
In a subgroup analysis based on BMI at baseline, overweight participants in the GJ 191 group reported a significant decrease in WOMAC pain score from baseline to week 12, which was not observed for the normal weight or obese groups (Table 4). There were significant decreases in current pain scores reported by participants in the overweight and normal weight groups with GJ 191 supplementation at week 12, but not in the obese group (Table 4). There was no significant difference between GJ 191 and placebo reported in this subgroup analysis.
Subgroup Analysis Based on BMI Categories from the PP Population (n = 64)
All values are mean ± SD; there was no statistically significant difference between groups for the primary outcome at week 6 or 12.
p-value for change from baseline.
P-values considered statistically significant are indicated in bold font.
VAS, Visual Analog Scale; WOMAC, The Western Ontario McMaster Universities Osteoarthritis Index.
Safety
A total of 52 AEs were reported during the study period, with 25 experienced by 19 unique participants in the GJ 191 group and 27 experienced by 14 unique participants in the placebo group. Two AEs of mild heartburn and constipation in the GJ 191 group and one AE of facial swelling in the placebo group were deemed “possibly” related to study products. Two serious AEs were reported in the GJ 191 group, which were acute cholecystitis deemed “unlikely” related and COVID-19 deemed “not related” to the study product. All AEs were recovered by the end of study or upon subsequent follow-up. All clinical chemistry and hematology parameters outside the normal range were deemed not clinically relevant, as assessed by the QI, except for one instance of elevated potassium and ALT. Upon repeat blood work, these elevated safety parameters returned to normal.
Discussion
Twelve weeks of GJ 191 supplementation significantly improved WOMAC pain, current pain, and bodily pain scores from baseline in a population of adults with mild to moderate knee OA. However, the placebo group also showed significant improvements in these measures at week 12. The lack of statistically significant differences between groups was unexpected. Therefore, further research investigating GJ 191 in knee OA populations would provide further understanding of this relationship. These further directions could possibly include a longer study duration to understand the long-term effects of GJ 191 or utilizing an exercise model to induce pain to examine the potential of GJ 191 in mitigating other aspects of OA-related pain. The lack of significant differences between groups may be, in part, attributed to the placebo effect.
This study found a placebo effect of 85% at week 6 and 71% at week 12, which is consistent with previous studies. 37,38 Although a significant difference between GJ 191 and placebo groups was not present at week 12, the results demonstrate a waning of the placebo effect over time. It is possible that if supplementation continued beyond 12 weeks, the placebo effect may have continued to wane, and a significant difference between GJ 191 and placebo would have been present. Therefore, studies of longer duration would further the understanding of the placebo effect in knee OA pain treatment with GJ 191 supplementation, keeping in mind that the placebo effect has been shown to vary based on treatment type (i.e., injections compared to dietary supplements). 39
While there was no difference between the groups after 12 weeks, there were notable changes at 6 weeks observed with GJ 191 supplementation, not reported with placebo. Those on placebo did not have significant improvements in bodily or current pain scores at week 6, suggesting GJ 191 supplementation may help to provide pain relief sooner than placebo, with sustained effects over time. Moreover, there were greater magnitudes of improvement in scores reported by participants in the GJ 191 group than those in the placebo group. These results are consistent with previous literature that administered a formulation containing Epimedium and S. miltiorrhiza extracts in patients with knee OA. 26 Addressing pain is priority as it is one of the most commonly targeted outcomes for OA treatment, 37,40 and can lead to disruptions in quality of life. 41,42
Results from subgroup analyses suggest those who reported moderate knee pain may benefit from GJ 191 supplementation to a greater extent than those with mild knee pain, possibly due to greater room for improvement in their symptoms of OA. Similarly, participants who were overweight reported significant reductions in WOMAC pain and current pain scores at week 12, consistent with previous studies that reported significant decreases in pain with nutraceutical supplementation in overweight adults with knee OA. 43 –45 Interestingly, these significant improvements were not observed for those with obesity, despite the effect of weight on joint health, 46 and increased risk for developing knee OA. 2 These results provide insight into specific subgroups of participants for whom GJ 191 supplementation may elicit a greater benefit and warrants further investigation.
Improvements with GJ 191 supplementation in knee pain were supported by a greater percentage of participants who reached an MCIC for KOOS symptoms score in the GJ 191 group than placebo at both weeks. A clinically relevant and meaningful change is important when considering efficacious options that may be discussed as part of the standard of care when treating OA. However, while a score change of 8–10 points is considered appropriate, more research is needed to define MCICs for specific populations. 30,43,47 The KOOS symptoms scale assessed knee OA symptoms beyond pain such as swelling and grinding, which may suggest other symptoms of knee OA were improved in more participants supplemented with GJ 191 than placebo to an extent that appears to be relevant to patients. These results are supported by findings from a preclinical study, which showed supplementation with the IP ingredients alleviated OA in a preclinical model. 25 Collectively, these studies suggest that the benefits of GJ 191 toward improving OA may extend beyond pain-relieving potential.
Importantly, supplementation with GJ 191 for 12 weeks was found to be safe in the studied population, with all AEs resolved by the end of study and no clinically relevant change in clinical chemistry and hematology. These findings support previously published literature examining safety parameters of this herbal formulation. Previous work has demonstrated that GJ 191 poses a low risk of potential health risks with the No Observed Adverse Effect Level (NOAEL) concluded as 5 g/kg bw/day for males and females and no risk of genotoxicity. 48 As other treatment options for knee OA are associated with negative side effects, 7,8,49 this study provides support for further research in more vulnerable populations, who may benefit from GJ 191 supplementation.
Beyond the placebo effect that has been previously discussed, the limitations of this study need to be considered. Participants were instructed to maintain their exercise routine for the duration of the study as exercise may positively affect knee OA. 50 However, participant data related to physical activity were not collected. Further, there are inherent biases in self-reported assessments; however, the tools used in this study are common in OA research. 43,51 –53 Although this clinical trial employed a robust randomized, double-blind, placebo-controlled study design, findings need to be confirmed in larger randomized controlled trials. Despite these limitations, the efficacy of GJ 191 supplementation on improving knee OA symptoms shows promise and future directions may be explored.
Conclusion
This study showed that supplementation with GJ 191 for 12 weeks significantly improved self-reported pain from baseline in a population of healthy adults with mild to moderate knee OA. These improvements were also observed by those on placebo, for which there was no statistically significant difference between the groups. However, results suggest improvements in pain may be experienced sooner with GJ 191 supplementation than placebo and may be sustained over time. The subgroup analyses suggest individuals with moderate pain, and those classified as overweight based on BMI, may benefit from GJ 191 supplementation to a greater extent. GJ 191 supplementation was found to be safe in the studied population.
Footnotes
Acknowledgments
Authors' Contributions
Z.L., J.Z., Y.C., Z.Zhang, and Z.Zhao: Conceptualization and methodology. L.L. and Y.W.: Methodology and resources. L.L., J.Z., and Z.L.: Investigation, formal analysis, writing—original draft, and writing—review and editing. S.W. and S.Z.: Supervision, project administration, and writing—review and editing.
Data Availability
The datasets used and/or analyzed during this study are available from the corresponding author on reasonable request.
Author Disclosure Statement
L.L., Y.W., S.W., J.Z., S.Z., and Z.L. are employees of
Funding Information
This research was funded by Chenland Nutritionals, Inc.
Supplementary Materials
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.