
Abstract
Introduction:
Stroke survivors can experience various consequences that affect their physical and psychological balance. Yoga seems to be relevant for this population as it allows to work on both the body and the mind. The first objective of this study was to investigate the non-inferiority of yoga compared with conventional physical activity in improving physical function in patients with chronic post-stroke sequelae. The secondary objective was to investigate the superiority of yoga in improving the mental health of these patients.
Methods:
A randomized controlled trial was conducted. Thirty-six patients were randomized into two groups to practice a yoga program (YOG'AVC) or the Fitness and Mobility Exercise (FAME) program. Patients were assessed in a blinding mode pre- (T0) and post-program (T1) and 3–4 months after completion (T2). The physical assessments were the Berg Balance Scale, timed up and go test, 6-minute walk test, and quadriceps strength measured by hand-held dynamometer. Questionnaire assessments were: Activities-specific Balance Confidence Scale–Simplified, State-Trait Anxiety Inventory, Beck's Depression Inventory, and the Reintegration to Normal Living Index.
Results:
The YOG'AVC program was not inferior to the FAME program in improving balance, functional mobility and muscle strength. Both groups showed significant improvement (p < 0.05) between T0 and T1 in their anxiety, depression, and reintegration to normal life scores, with no significant difference between groups.
Discussion:
Both programs seem to be valuable in improving the physical abilities and psychological well-being of chronic post-stroke patients. However, further studies are required to confirm the difference between these programs.
Introduction
Stroke survivors can experience a wide range of disabilities, including cognitive, motor, and psychological impairments. 1,2 Hemiparesis is one of the most common motor disorders resulting from altered muscle tone and motor control. 1,3 This often leads to functional mobility restrictions, with difficulties in walking, transferring, and other activities of daily living. 1,2,4 As a result, stroke survivors are often too sedentary, which is a major risk factor for stroke recurrence. 5,6
Also, balance difficulties are common since balance depends on the sensory, neuromotor, and musculoskeletal systems that can be affected by stroke. 1,4 As a result, stroke patients are at a significantly higher risk of falling, compared with healthy adults of a similar age. 7 Further, stroke increases the risk of developing psychological disorders such as anxiety, depression, emotion lability, and apathy. 8 In the chronic phase (≥6 month post-stroke), regular physical activity is recommended, including balance, weight transfer, walking and strengthening exercises, especially for patients with poorer balance ability. 7,9 –11
These exercises can be offered as circuit class therapy in small groups supervised by a therapist. 12,13 Yoga is a physical activity that is likely to improve balance and mobility in people with stroke, but which explores physical practice in a different way compared with traditional exercise. 14 –16 In addition, the combination of breathing and meditative exercises may bring psychological benefits through the regulation of emotions. 17 Its effect as a therapy is currently being studied by a growing number of scientists. 18
Yoga is a philosophy and a mind-body practice that originated in India more than 2000 years ago. In Western countries, the components of yoga that are very commonly applied for health benefits are physical posture (asanas), breath control (pranayama), and meditation. 19 Paranjape and Gore investigated the effect of a yoga postural practice (asanas only) in comparison with conventional balance exercises on functional balance abilities of hemiplegic patients. 16 Intra-group analysis showed significant post-treatment improvement in both groups, but inter-group analysis indicated no difference.
They concluded that the postural aspect of yoga appears to be as effective as conventional balance exercises in improving balance in post-stroke hemiplegic patients. Nevertheless, the methodological design of this study was originally conceived to establish the superiority of one therapy over the other. In the case where there is already a reference treatment and where an alternative treatment appears to provide additional benefit (e.g., easier to implement, less expensive, etc.) but not necessarily more effective for the outcome studied, an equivalence or non-inferiority design should be used. 20
Thus, as Paranjape and Gore suggest, it is possible that the physical components of yoga practices (asana) are as effective as conventional balance exercises since they have several similarities: muscular strengthening, improvement of proprioception, gain of mobility. However, they also have important differences: emphasis on breath control, mindfulness during practice, and importance given to maintenance of postures are some of the elements that differentiate yoga practices from physical exercises. 19
It would, therefore, be relevant to evaluate the effectiveness of a complete yoga approach on balance and functional mobility. In addition, the practice of meditation during yoga sessions could also have an effect on the mental health of participants. Indeed, a recent review suggested that the practice of passive meditation (i.e., non-active form) is more effective than physical exercise in improving psychological criteria, such as anxiety. 21
Previous meta-analyses have shown the benefits of yoga and especially meditation for general psychological disorders such as anxiety and depression, but the level of evidence was low. 22,23 It would therefore also be relevant to conduct a new study to compare the effects of yoga and conventional physical activity on the mental health of adults with stroke.
Other systematic reviews have investigated the improvement in balance, mobility, and health-related quality of life, in adults with stroke through yoga practice, but the quality of evidence was very low. 24,25 It seems necessary to carry out new randomized controlled trials on the interest of yoga in the rehabilitation of stroke patients.
The aim of the current study was to investigate the effects of an adapted yoga program (including asanas, pranayama, and meditation) to improve the physical functions and mental health of patients with chronic post-stroke sequelae. Our hypotheses, based on current knowledge from the studies presented earlier, were as follows: (a) an adapted yoga program would not be inferior to conventional therapy in improving physical function in chronic post-stroke patients, and (b) an adapted yoga program may be superior to conventional therapy in improving the mental health of participants.
Methods
Study design
A randomized controlled trial was performed. This manuscript is written in accordance with the Consolidated Standards of Reporting Trials (Supplementary Material S1 CONSORT Checklist) criteria. The research was conducted in France and approved by the protection National ethical committee (IDRCB: 2020-A03408-31). The protocol was registered on ClinicalTrial.gov (NCT04947293). All participants gave their written informed consent to participate. The treatments took place in a rehabilitation center as well as in the community, depending on where the participants lived.
Participants
For participant enrollment, articles were posted in local newspapers and information letters were distributed to local health professionals and patient associations. Inclusion criteria were as follows: hemiparesis resulting from a stroke that occurred more than 6 months ago, with a balance disorder (score between 22 and 51 points on the Berg Balance Scale [BBS]), and able to stand and walk at least 10 m, with or without a device.
Volunteers were not included if they met any of the following exclusion criteria: less than 18 years of age, suffering from a cognitive disorder (score <4 points on the short 6-items Mini-Mental State Examination 26 ), diagnosis of another pathology that may explain the balance disorders, a medical contraindication to physical activity, or current and regular participation in another physical activity program. An eligibility criterion had to be added during the experimental phase because of the COVID-19 pandemic: being up to date on COVID-19 vaccinations.
Volunteers were initially screened for participation eligibility based on an initial phone call, followed by a face-to-face meeting. Eligible participants were then referred to a blind evaluator for baseline assessment in the rehabilitation center and were allocated to a group.
The required number of subjects has been estimated from a previous study, 27 using the standard deviation (SD) of the BBS (SD = 7.64), and the non-inferiority margin defined as the minimum detectable change (MDC = 4.66). 27 We hypothesized that the difference between the two groups would be 0. Considering a type I error of 5% and a statistical power of 80%, 84 patients were required. 28
Randomization
Subjects were randomly allocated to one of the two study groups using a stratified block randomization procedure by an independent researcher, using R software, an allocation ratio of 1:1, and random block sizes. The randomization list was stratified according to the place of experimentation, the BBS (score > or <40 points). Subjects were informed of their assignment by phone by an investigator (R.L.d.C.) in charge of the treatments.
Interventions
Participants were randomly assigned to the experimental group to practice yoga (YOG'AVC program) or to the control group to practice conventional exercise (Fitness and Mobility Exercise [FAME] program). Both programs lasted 12 weeks and consisted of three weekly 1-h sessions. Two sessions were conducted in groups (maximum five individuals/group) during the week, and one session was performed independently at home.
The group sessions were supervised by the same physiotherapist who ensured the adaptation of the exercises and the safety of the participants. A video or paper support (at the patient's convenience) was distributed each week to be used for the independent sessions at home.
A yoga program adapted to post-stroke sequelae was developed by a physiotherapist and yoga teacher (Yoga Alliance certified). This YOG'AVC program is based on the teaching of postures (asanas), breathing (pranayama), and meditation. The practice of postures is based on the Iyengar method with the use of many supports (e.g., block, strap, chair, cushions, wall).
Particular attention was devoted to breathing during each posture. The complexity of the postures and their holding time increased over the course of the program, relative to the abilities of each participant. The structure of a session and the names of the postures that were taught throughout the program are detailed in Figure 1.
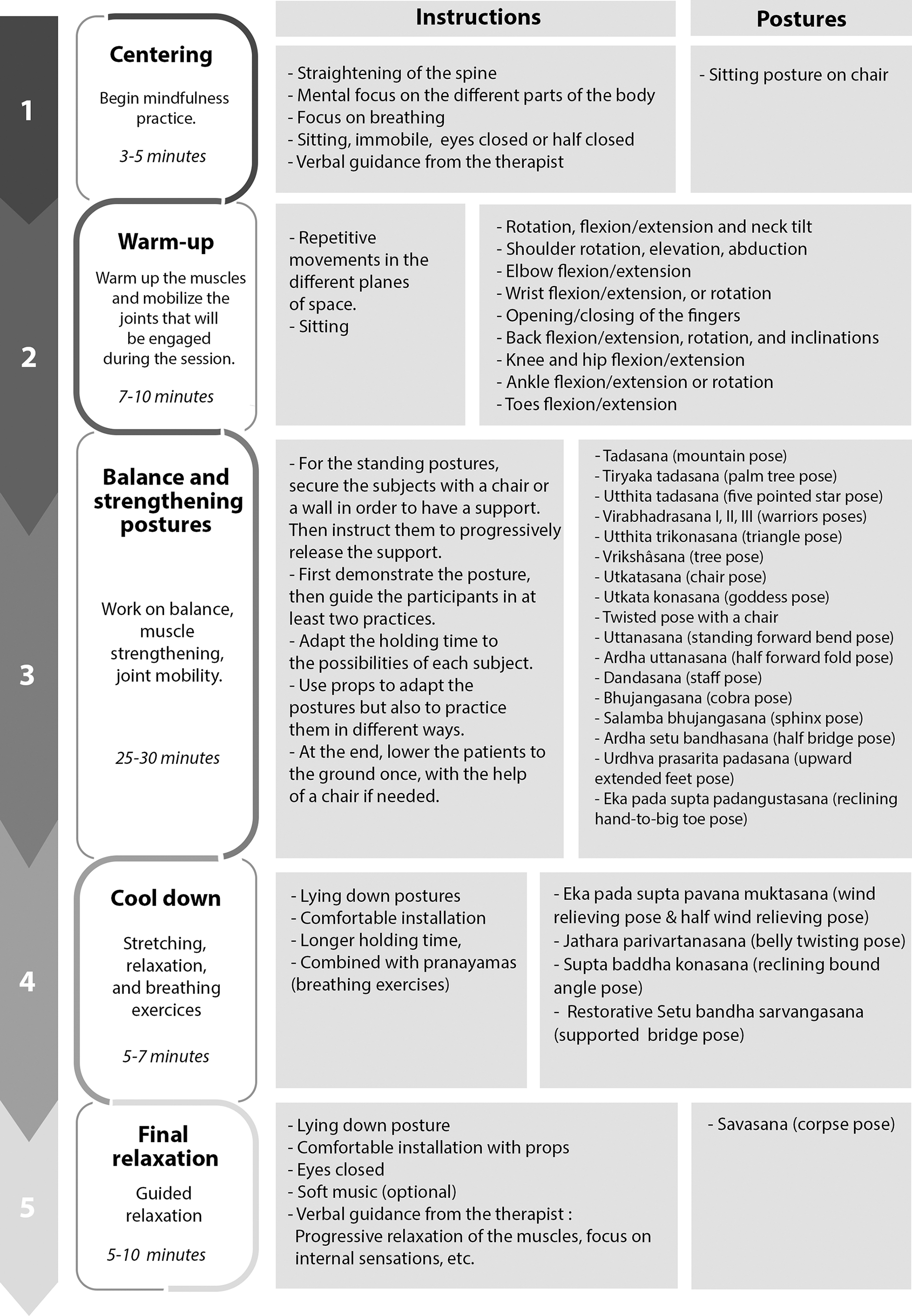
A YOG'AVC session and taught postures.
The control group was invited to participate in more conventional exercise sessions based on the FAME program. All information about this program is available on the fameexercise.com website. It was specifically designed for people living with post-stroke sequelae. The sessions consist of a warm-up, functional strengthening exercises (e.g., sit-stand on chair, wall chair exercise), balance exercises (e.g., forward or side lunges, balance standing with one foot close together or on one leg), agility and fitness exercises (e.g., up and down a step, walking), and ends with a cool-down (stretching) phase.
As the program progresses, the number of repetitions, sets, or duration of hold time can be gradually increased, in accordance with participants' progress. The effectiveness of this program has been demonstrated in previous randomized controlled trials. 12,13,29
Assessment procedure
The patients were assessed three times during the study: before treatment (T0), after treatment (T1), and 3 months after the end of treatment (T2). All assessments were performed in a blinded mode by two evaluators who assessed the same subjects at each assessment. These evaluators had no contact with the participants other than during the evaluations, and the participants were instructed never to mention their treatment in front of them.
Our primary outcome was balance assessed by the BBS. This scale is reliable, valid, and often used for assessing balance in stroke patients. 27,30 Self-perceived balance confidence was assessed by the Activities-specific Balance Confidence Scale–Simplified (ABC-S). The reliability and validity of the French version of this questionnaire have been established. 31 Functional mobility was assessed by the timed up and go test (TUG) and the 6-minute walk test (6MWT). 27,32
The TUG is based on the performance of a functional task, and a score in seconds is established. Gait performance was assessed by the 6MWT, a walking test with a score in meters. These tests are reliable and valid for a chronic stroke population. 27,32 The muscular strength of the lower limbs was evaluated by measuring the maximum isometric force of knee extension with a hand-held dynamometer (Microfet2®; Hoggan Health, Salt Lake City), 33 which is a reliable and valid method in a stroke population. 34
State and trait anxiety were assessed by the State-Trait Anxiety Inventory. The reliability and validity of the French version of this questionnaire have been established. 35 Depression was assessed by Beck's Depression Inventory (BDI). The reliability and validity of the French version of this questionnaire have been established. 36 The Reintegration to Normal Life Index was used to assess quality of life. It was developed to quantitatively assess the degree to which individuals who have experienced a disabling illness are able to reintegrate into the activities of daily living within the community.
The reliability and validity of this questionnaire have been established. 37 Adherence to the program (T0–T1) was measured directly by the percentage of group sessions completed, the percentage of independent home-based sessions reported as completed, and, between T1 and T2, the mean number of sessions completed per week (i.e., collected using a logbook).
Statistical analysis
Statistical analyses were performed by a biostatistician using R software version 4.0.5. The intention-to-treat (ITT) population contains all the randomized patients. The per-protocol (PP) population contains patients who completed at least 80% of the planned sessions between T0 and T1. To analyze the non-inferiority, the lower or upper limit, as adapted of the 95% confidence interval (95% CI) of the difference of evolution from baseline between the groups, was compared with the non-inferiority margin (mean in case of normality, median computed by bootstrap with 10,000 repetitions otherwise).
The margins of non-inferiority selected were based on the MDC or the minimal clinically important difference (MCID) of each scale available in the literature (Table 1). When several MDC or MCID were found, the one based on the population most similar to this study was selected. 27,38 –41 For psychological variables, a superiority analysis was performed, based on the ITT population.
Non-Inferiority Margins
6MWT, 6-minute walk test; ABC-S, Activities-Specific Balance Confidence Scale–Simplified; BBS, Berg Balance Scale; COPD, chronic obstructive pulmonary disease; MCID, minimal clinically important difference; MDC, minimum detectable change; TUG, timed up and go test.
The median evolution since baseline was compared between groups by a Mann-Whitney-Wilcoxon, as scores were not following a normal distribution. The 95% CI around the median differences were computed. In a post hoc analysis, the evolution from T0 to T1 and T2 within each group was tested with a paired Student's t-test in cases of normality and a paired Wilcoxon test otherwise. A significance threshold of 5% is used for all analyses.
Results
Participants
The recruitment lasted from March 2021 to February 2022 and the follow-up period extended to September 2022. A total of 55 volunteers responded to the recruitment campaign (Fig. 2). Of them, 36 individuals were randomized in 2 groups (Table 2). During the treatment phase, four patients (two in each group) prematurely discontinued participation for medical reasons unrelated to the treatments. At follow-up (T2), six patients (three in each group) were lost to follow-up.

Participant flow diagram.
Baseline Demographic and Clinical Characteristics of Participant (Intention-to-Treat Population)
6MWT, 6-minute walk test; ABC-S, Activities-specific Balance Confidence Scale–Simplified; BBS, Berg Balance Scale; BDI, Beck's Depression Inventory; BMI, body mass index; FAME, Fitness and Mobility Exercise; IQR, interquartile range; RNLI, Reintegration to Normal Life Index; SD, standard deviation; STAI, State Trait Anxiety Inventory; TUG, timed up and go test.
In the ITT population, attrition at T1 was quite low (89% of available patients in each group) and acceptable at T2 (72% of available patients in each group). In the PP population, the number of patients at T1 was acceptable (72% and 67% of patients included in the YOG'AVC group and FAME group, respectively), but attrition was higher in the FAME group at T2 (50% of patients not present in the analysis).The sample size initially calculated (n = 84) was not reached due to a lack of resources to continue the study.
However, taking into account the actual data from our sample (BBS: SD of 6.5 and difference between groups of 1.5), the power calculation allows us to estimate that at T1 we have enough subjects for our main outcome (power = 0.83), but not at T2 (power = 0.75).
With regard to adverse events, before the beginning of the sessions (T0), one participant in the experimental group was hospitalized for a stroke recurrence, and one participant in the control group reported suffering from a disabling rheumatic disease that prevented him from participating in the sessions. During the experimental phase (T0–T1), one participant in the YOG'AVC group had two hallux-valgus operations and one participant in the FAME group was hospitalized for an appendicitis crisis. During the follow-up phase (T1–T2), one participant in the YOG'AVC group died of heart failure while gardening.
Physical variables
Regarding physical variables, we hypothesized the non-inferiority of the YOG'AVC over the FAME program. For this type of analysis, both populations were studied, so Table 3 shows the ITT and PP analyses. In both the ITT and PP populations, the YOG'AVC program was not inferior to the FAME program at T1 or T2 for the BBS, the ABC-S, the TUG, or the 6MWT.
Evolution of Physical Variables Since Baseline (T0) in Post-Treatment (T1) and Follow-Up (T2) in Intention-to-Treat and Per-Protocol Population
↗: the score increases in case of improvement.
↘: the score decreases in case of improvement.
6MWT, 6-minute walk test; 95% CI, 95% confidence interval; ABC-S, Activities-specific Balance Confidence Scale–Simplified; BBS, Berg Balance Scale; FAME, Fitness and Mobility Exercise; ITT, intention-to-treat; Pop., population; PP, per-protocol; SD, standard deviation; TUG, timed up and go test.
For the maximum isometric knee extension force on the healthy side at T1, the 95% CI was higher than the non-inferiority margin, but at T2 the lower limit was inferior to this margin (in the ITT and PP populations); on the affected side at T1 and T2, the 95% CI was higher than the non-inferiority margin in the ITT population, but not at T2 in the PP population.
Psychological variables
Regarding psychological variables, we hypothesized the superiority of YOG'AVC over the FAME program. For this type of analysis, the ITT population was the more important. The YOG'AVC program was not significantly superior to the FAME program in improving anxiety, depression, or reintegration into normal life (Table 4).
Evolution of Psychological and Social Variables Since Baseline (T0) in Post-Treatment (T1) and Follow-Up (T2) in Intention-to-Treat Population
Significant results are in bold.
↗: the score increases in case of improvement.
↘: the score decreases in case of improvement.
95% CI, 95% confidence interval; BDI, Beck's Depression Inventory; FAME, Fitness and Mobility Exercise; IQR, interquartile range; RNLI, Reintegration to Normal Life Index; SD, standard deviation; STAI, State Trait Anxiety Inventory.
The additional analysis of the intra-group evolution also showed that patients following the two programs showed an improvement in these criteria at post-treatment (T1). However, after follow-up (at T2), only the FAME group still showed a statistically significant change in trait-anxiety and depression, in ITT population (Table 5). But in the PP population, both groups significantly change the trait-anxiety (i.e., YOG'AVC: p = 0.01; FAME: p = 0.05) and depression (YOG'AVC: p = 0.03; FAME: p = 0.02).
Participant Compliance (Intention-to-Treat Population)
FAME, Fitness and Mobility Exercise; IQR, interquartile range; SD, standard deviation.
Compliance
During the experimental phase (T0–T1), compliance with the group sessions was high and similar in the two groups with an overall median of 91.7% (Table 5). However, the home sessions were less well attended with an overall average compliance of 57.0%. During the follow-up phase (T1–T2), the overall median was 0.5 sessions per week, with no significant difference between groups.
Discussion
The primary objective of this study was to investigate the non-inferiority of the YOG'AVC program compared with the FAME program in improving balance in chronic post-stroke patients. Non-inferiority was demonstrated in both the ITT and PP analyses.
Patients in both groups improved their scores on the BBS, although these improvements did not exceed the MDC of the scale, which may raise questions about the efficacy of the two therapies. However, if we look at the individual evolution of the participants between T0 and T1, 31% of the patients in each group showed an improvement above the MDC. The BBS score at T0 in these 31% was 41 ± 7, whereas the mean of the other patients was 48 ± 11.
It is likely that improvement beyond the MDC is easier to achieve when the participants' initial scores are low and they have more margin for improvement. Paranjape and Gore also found significant improvement in the group that practiced yoga postures and the group that practiced conventional exercises. 16 In their study, these improvements on BBS averaged 8 points, thus greater than the MDC.
Their sample had initial scores with a median around 40, whereas the median for our sample was 50. Also, Schmid et al. demonstrated in their pilot study that a significant improvement above 6 points on the BBS was possible in a population with an average initial score about 41 points and practicing a yoga program. 42 It is, therefore, possible that the margin of improvement was smaller for our population, which explains why the majority of our participants did not show improvement above the MDC.
As for the FAME program, Pang et al. had a population similar to ours (baseline BBS score around 47 points) and the post-treatment improvement was also below the MDC. 12 Therefore, future studies investigating the improvement of functional balance with the BBS should focus on including more patients with a score below 40 points. Similarly, our results on the self-perceived confidence in balance (ABC-S) and functional mobility (TUG and 6MWT) demonstrated the non-inferiority of the YOG'AVC program.
However, the average improvement in both groups did not exceed the MDC of ABC-S scale and the TUG. Interestingly, the result of the TUG in the YOG'AVC group (ΔT2–T0 in ITT population: −2.7 sec) was close from the MDC (3.2 sec), but not the FAME group (ΔT2–T0 in ITT population: −0.2 sec). Further, for the 6MWT, the median difference of the YOG'AVC group (ΔT1–T0 in ITT population: 37.5 m) exceeded the MCID (30.5 m) whereas the FAME group was close (ΔT1–T0 in ITT population: 23.5 m).
This clinically relevant improvement is very encouraging as walking abilities are essential in the prevention of sedentary lifestyles. 10 Schmid et al. 14 and Immink et al. 15 also showed an improvement in walking (during 6MWT) in their yoga groups. It is possible that this improvement was related to muscle strengthening. 43 As regards our results on quadriceps strength on the healthy side and the affected side, in post-treatment (T1) the non-inferiority of the YOG'AVC program was confirmed but the improvement was no greater than the MCID in the two groups.
However, this could not be confirmed at T2 because the mean in the FAME group continued to increase more consistently than in the YOG'AVC group. This can be explained by the smaller sample size at T2 and the very heterogeneous results of the participants. Indeed, the analysis of the individual evolution of the participants showed a relatively homogeneous improvement in muscle strength in post-treatment (T1), but not at the follow-up (T2).
This difference is probably related to the physical activity that continued between T1 and T2. Although no significant difference in activity compliance was found between the groups, we cannot conclude that the two groups maintained the same level of physical activity over this period. Indeed, we focused only on the practice of FAME or YOG'AVC sessions, but patients were able to practice other types of physical activity (e.g., walking, gardening, etc.).
In addition, it seems relevant to note (during the T0–T1 period) that the face-to-face group sessions were much more followed (91.7%) than the home-based sessions (57%). Lack of motivation to practice the home-based sessions was the most frequently reported reason (63%), which is consistent with previous studies. 10,44
The practice of group exercise, structured and supervised by a professional, has been found to be an important factor of adherence as well. 10,45 Indeed, the possibility of meeting other stroke survivors—thus benefiting from psychological and social support—and the benefit of professional support in guiding and facilitating the physical activity were the most frequently reported motivators. 10
The hypothesis that the YOG'AVC program might be more effective than the FAME program in improving the mental health and social reintegration of the participants could not be confirmed since no difference in evolution between the groups was demonstrated at post-treatment (T1) or at the 3-month follow-up (T2). In addition, in post-treatment (T1), both groups significantly improved their state and trait anxiety, depression, and reintegration to normal life scores.
Results after the 3-month follow-up (T2) are more uncertain, as intra-group analyses differ according to the population analyzed (ITT or PP). Regarding anxiety score in a previous study, Immink et al. found a clinically significant decrease in the trait anxiety score (8 points) of their yoga group, without being able to demonstrate a significant difference with the inactive control group. 15
In our study, the YOG'AVC group showed a median improvement of 7 points in post-treatment, which is very close to this clinically significant improvement, whereas the FAME group showed a median change of only 4 points. Regarding depression, Immink et al. did not find significant improvement over time or difference between groups, but we did not use the same score.
In our study, although both groups had median scores already reflecting mild depression (i.e., a score between 10 and 18 points on the BDI) at baseline, a significant improvement in both groups was demonstrated in post-treatment. Thus, our results indicating an improvement in the psychological state of both groups seem globally encouraging.
It is possible that they result from different factors such as the social aspect of the group sessions where some participants created strong relationships. The improvement in physical criteria could also have helped to reduce anxiety and depression since patients were able to gain more confidence in themselves and their abilities. Thus, these two programs share common points in that they offer physical activity adapted to the motor impairment of the participants, with group sessions that allow the creation of social relationship and reassuring supervision through the presence of a therapist.
However, they also have notable differences in exercise approaches. In yoga, participants are asked to focus on their bodily sensations, to become aware of the positioning of their body in space, which requires significant concentration; the postures are maintained statically with muscles in isometric contractions and a solicitation of the deep postural muscles.
In conventional exercises, the movements are performed in a more mechanical way, but with different modalities of muscular contraction (isometric, concentric, eccentric) and with a more functional purpose. In yoga, a concentrated state of mind is required in each exercise, and physically intense postures are alternated with gentler postures, which allows one to work constantly during the session but leaves little time for discussion.
In conventional sessions, intense standing exercises are interspersed with seated breaks and participants can more easily discuss. It is possible that the YOG'AVC program results in greater joint mobility since the postures work on maximum joint ranges, whereas the FAME program is perhaps more effective for working on endurance since the participants are much more in movement. Future studies may focus on the differences that exist between these programs.
For the moment, we have been able to show their similarity to improve balance, functional mobility, muscular strength, mental health, and reintegration into normal life of patients with stroke. From a clinical point of view, to choose the intervention that is most appropriate for a patient, it is probably appropriate to consider their desires and expectations.
The main limitation of this study was the sample size, which was smaller than expected. Still, as the difference observed between the two groups was higher than expected and favorable to the yoga intervention, most of our objectives have been met. It is, however, indisputable that the low number of patients is a limit to the possibility to generalize the results observed, and that we can reach a definitive conclusion from this study.
Second, although we included participants with a BBS score of less than 51 points, with the aim of ensuring a margin of improvement at least equivalent to the MDC (4.66 points), it is likely that a lower margin or using other scales with lower ceiling effect would have been more relevant. Also, our sample contained a small number of truly anxious or depressed patients, as this was not an inclusion criterion. Future studies with a sufficient sample of patients with more severe anxiety or depression should be better able to determine the effectiveness of these programs to improve mental health.
Finally, the proposed interventions were only feasible for patients with a sufficient degree of functional recovery (see inclusion criteria) and without a significant cognitive disorder, and as a result, they are not generalizable to all patients with stroke.
Conclusions
Despite these limitations, this study showed that an adapted yoga program was not inferior to a conventional physical activity program in improving balance, functional mobility and muscle strength in patients with post-stroke sequelae. In addition, both interventions appeared to have the potential to improve the mental health and quality of life of the participants.
Hence, both programs can be offered to patients with chronic post-stroke sequelae. The sessions can be offered in a rehabilitation center as well as in non-rehabilitation facilities, as minimum equipment is required to perform the exercises. Improvement seems possible within 3 months of regular practice. On the other hand, it seems that patients are less compliant when the sessions are practiced independently, which highlights the value of pursuing group practice over time.
Footnotes
Acknowledgments
The authors would like to acknowledge the contribution of Mr. Thouin and Mr. Vallois-Da Cuhna who graciously completed their role as blind evaluators.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Authors' Contributions
R.L.d.C. and J.C. designed and conceptualized the study, collected and interpreted the data. S.V. participated in the design of the study and carried out the statistical analysis of the data. All authors read and approved the final manuscript.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study received financial support from the association “France AVC Normandie.”
Supplementary Material
Supplementary Material S1 CONSORT Checklist
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.