
Abstract
Background:
Intraoperative anxiety is a common problem when Monitored Anesthesia Care (MAC) is used instead of general anesthesia during minor surgical procedures such as port catheter placement. Nonpharmacological anxiolytics such as aromatherapy have been studied for their effects on preoperative anxiety, but no placebo-controlled study of aromatherapy during surgeries under MAC has yet been performed.
Methods:
After IRB approval, 70 patients were randomized 1:1 to receive either a lavender/peppermint aromatherapy patch (Elequil Aromatabs®; Beekley Corporation) or a matching placebo patch. The primary outcome, time to readiness for discharge from postoperative acute care units (PACU; min), was assessed every 15 min until a modified postanesthesia recovery score for ambulatory patients (PARSAP) score of 18 or higher was reached. In the preoperative holding area, the assigned patch/placebo was activated and affixed to a folded towel placed aside the subject's head, contralateral to the side of the planned surgery. The towel and patch/placebo were discarded when the subject left the operating room (OR).
Results:
No difference was found between the treatment and placebo groups on the primary outcome of time to discharge readiness (mean [standard deviation, SD]: 82 [15] vs. 89 [21] min, respectively, p = 0.131). No difference was found between the treatment and placebo groups on the secondary outcomes of intraoperative midazolam dose, intraoperative opioid dose, intraoperative ondansetron dose, or intraoperative promethazine dose. No difference was found between the treatment and placebo groups in the proportion of subjects requiring rescue postoperative nausea and vomiting (PONV) medication in the PACU or the proportion of subjects requiring opioids in the PACU. No difference was found between the treatment and placebo groups in pain intensity in PACU, average PONV score in PACU, or patient satisfaction in PACU. PACU patient satisfaction was high for both the patch and placebo groups (35/35 [100%] vs. 32/34 [94%] “very satisfied,” p = 0.239).
Conclusions:
Aromatherapy treatment is not indicated intraoperatively to reduce anxiety or the use of antiemetics in patients requiring Port catheter placement. Trial registration: Clinicaltrials.gov, identifier: NCT05328973.
Introduction
Intraoperative anxiety is a frequent problem when Monitored Anesthesia Care (MAC) is used instead of general anesthesia during minor surgical procedures such as Port-a-catheter (Port-a-Cath) placement. 1 –3 Johansson et al. reported that 60% of the patients felt “unpleasant” during Port-a-Cath implantation insertion under local anesthesia. 4 Intraoperative anxiety is associated with a negative influence on pain perception, increased use of sedatives such as benzodiazepines (i.e., midazolam) and opioids, prolonged recovery after surgery, and unnecessary postprocedural hospitalization. Benzodiazepines such as midazolam are associated with fatigue, confusion, respiratory depression, and restlessness which limit patients' ability to actively participate in their intra- and postoperative care. 5,6
Furthermore, Chang et al. found that the use of benzodiazepines does not improve patient's satisfaction during Port-a-Cath placement. 7 Nonbenzodiazepine drugs such as dexmedetomidine can also be used to provide procedural anxiolysis. Intraoperative sedation with intravenous (IV) dexmedetomidine has demonstrated a significant reduction in postoperative opioid consumption and prolongation of postoperative analgesia when general anesthesia is avoided, as reported by Giordano et al. 8 However, dexmedetomidine can cause hypotension, bradycardia, and prolonged sedation. Due to the potential adverse effects of benzodiazepines, dexmedetomidine, and opioids, alternative nonpharmacological therapies have been studied. 1,9,10
Essential oils have a long tradition as natural products with pharmacological applications. 11 –14 Aromatherapy, the therapeutic use of essential oils extracted from aromatic plants, may offer a simple, low-risk, and cost-effective method of managing intraoperative anxiety. 15 Aromatherapy is fast-acting, noninvasive, has minimal side effects, and can be applied in multiple forms. 16 Various essential oils have been studied to reduce anxiety. 17 Linalyl acetate and linalool are molecules found in lavender which have anxiolytic effects. 18 Peppermint oil has long been valued for its antinausea effect. 19,20 Minimizing sedation, nausea, and vomiting are desirable to accelerate the recovery of patients in high-volume postoperative acute care units (PACU). Because the existing literature is equivocal for both lavender and peppermint aromatherapy, a well-designed placebo-controlled trial may help resolve some of the uncertainty regarding their clinical effect in the ambulatory perioperative setting.
To our knowledge, there have been no studies of aromatherapy conducted on subjects undergoing surgery performed under MAC, specifically for Port-a-Cath placement. Our primary hypothesis was that preoperative and intraoperative placement of an active lavender-peppermint patch (vs. placebo patch) would result in a shorter time to discharge-readiness in PACU.
Methods
Study design and ethics
The study was a prospective, single-center, placebo-controlled, randomized controlled trial. We obtained study approval from the Institutional Review Board of the University of Texas MD Anderson Cancer Center (approval No. 2021-0994, date of approval April 26, 2022). The study was registered before any subject enrollment at https://clinicaltrials.gov/study/NCT05328973, date of registration April 14, 2022.
Participants
We conducted this study at a single tertiary-care hospital (cancer center). Patients were included in the study if they (1) were ≥18 years old; (2) were English-speaking, and (3) gave written informed consent. Exclusion criteria included (1) planned additional surgical procedures during Port-a-Cath placement (including explantation of a Port-a-Cath or other previous vascular access device); (2) subjects requiring general anesthesia or not eligible for MAC; (3) allergy or sensitivity to plants, essential oils, or any of the medications used in this study; (4) history of G6PD deficiency or atrial fibrillation; (5) inability to complete study questionnaires; (6) complete anosmia or history of intolerance to aromatherapy; (7) daily use of any opioid for 90 days or more; and (8) daily use of any benzodiazepine for 30 days.
Randomization and blinding
Subjects were randomized 1:1 using an in-house electronic randomization tool (Clinical Oncology Research CORe) to either a lavender/peppermint aromatherapy patch (Elequil Aromatabs®; Beekley Corporation) or a matching placebo patch, which was identical except for lacking aromatic essential oils. Patients were randomized as a single block. Randomization occurred within 2 h of the scheduled operating time. As the intervention consisted of an aromatherapy patch, blinding was not feasible for the subject and preoperative and intraoperative caregivers. The aromatherapy/placebo patch and the towel that was placed were discarded before the subject reached the PACU; thus, the PACU caregivers were blinded to the group assignment.
Perioperative care
The assigned active (Aromatab®) or placebo patch was activated in the preoperative holding area by opening the outer plastic envelope and then affixed to a folded towel and placed aside the subject's head, contralateral to the side of the planned surgery. Patients in the active treatment group confirmed the smell of the patch. Subjects were eligible to receive a maximum dose of 2 mg midazolam IV in the preoperative holding area just before transportation to the operative suite, depending on subject's age, physiologic condition, and patient/provider preference. The towel and Aromatab/placebo were transferred to the operating table with the subject as they arrived in the operative suite and maintained beside the subject's head throughout the surgery.
Standard physiologic monitors were placed on arrival to the operating room (OR) as per American Society of Anesthesiologists (ASA) standards. A nasal oxygen cannula or a facemask was placed to maintain adequate oxygenation, at the discretion of the anesthesia provider (Certified Registered Nurse Anesthetist and/or Physician Anesthesiologist). All Port-a-Cath placements were performed by the same surgeon (E.B.). The surgeon routinely injected local anesthetic (bupivacaine 0.25%–0.5%) around the surgical wound during the procedure and remained blinded to the treatment. The anesthesia provider administered intraoperative doses of midazolam IV or opioids IV as needed, titrating to the desired level of sedation and analgesia. Prophylactic antiemetics were not routinely given; rescue antiemetics were administered as needed during the procedure and afterward.
Postoperatively, all subjects were taken to the PACU and managed following routine clinical care. Subjects received supplemental postoperative opioids or other analgesics for breakthrough pain as necessary in the PACU. Rescue antiemetics were administered as necessary and per standard of care. In the PACU, a research fellow unblinded to the treatment assessed each subject's nausea/vomiting, pain intensity, and satisfaction.
Outcomes
The primary hypothesis was that aromatherapy could significantly reduce time to readiness for discharge from PACU (min) after surgery compared to placebo. The primary outcome, time to readiness for discharge from PACU (min), was assessed every 15 min until a modified postanesthesia recovery score for ambulatory patients (PARSAP) of 18 or higher was reached. 21 The capacity of PACU to accommodate patients immediately after surgery is crucial for efficient OR activity in a busy ambulatory surgical center. We chose time to discharge from the PACU as the primary outcome because it is influenced by postoperative nausea and vomiting (PONV) and pharmacological residual sedation. 22,23
Secondary outcomes included intraoperative midazolam use (mg), intraoperative opioid use assessed in mg of Morphine Equivalent Daily Doses (MEDD), intraoperative antiemetic use (mg), time to first occurrence of postoperative nausea or vomiting in PACU (min), rate and intensity of PONV in PACU, the proportion of subjects requiring antiemetics in PACU, rate of subjects requiring opioids in PACU, pain intensity in PACU (0–10 numerical rating scale), and subject satisfaction in PACU rated on a 5-point Likert scale from 1 (“not at all satisfied”) to 5 (“very satisfied”).
Statistical analysis and sample size
We observed from preliminary data on subjects treated with standard of care that the mean PACU duration was 66.5 min with a standard deviation (SD) of 20.7. Accordingly, a power calculation revealed that the inclusion of 31 subjects in each treatment arm would provide 80% power to detect a difference of 15 min in mean time to readiness for discharge from PACU after surgery using a two-group t test with a two-sided Type I error rate of 0.05 (nQuery+nTerim 4.0). A reduction of 15 min was considered substantially important to facilitate bed availability in a busy PACU. 24 Enrollment was planned for 70 subjects, anticipating that this would yield at least 31 eligible and treated subjects in each group.
Subjects' demographics, treatment, and clinical outcomes were summarized through descriptive statistics. Fisher's exact test or chi-square test was used to evaluate the association between two categorical variables. Wilcoxon rank sum test was used to compare location parameters of continuous distributions between subject groups. Statistical software SAS 9.4 (SAS, Cary, NC) was used for all analyses. A p < 0.05 was considered statistically significant.
Results
From May 12, 2022 to March 8, 2023, 35 subjects were enrolled in each group; intraoperative and PACU data were partially lost for one subject in the placebo group because of an administrative error after randomization (Fig. 1). The mean age (SD) of participants was 52 years. Most participants (N = 54, 77%) were female, and 96% (N = 67) had an ASA physical status of 3. Most participants scored in the normal range for anxiety (N = 60, 87%) and depression (94%) on the hospital anxiety and depression scale (HADS). 25 Few subjects reported any preoperative intermittent use of opioids (N = 4, 6%) or benzodiazepines (N = 2, 3%).
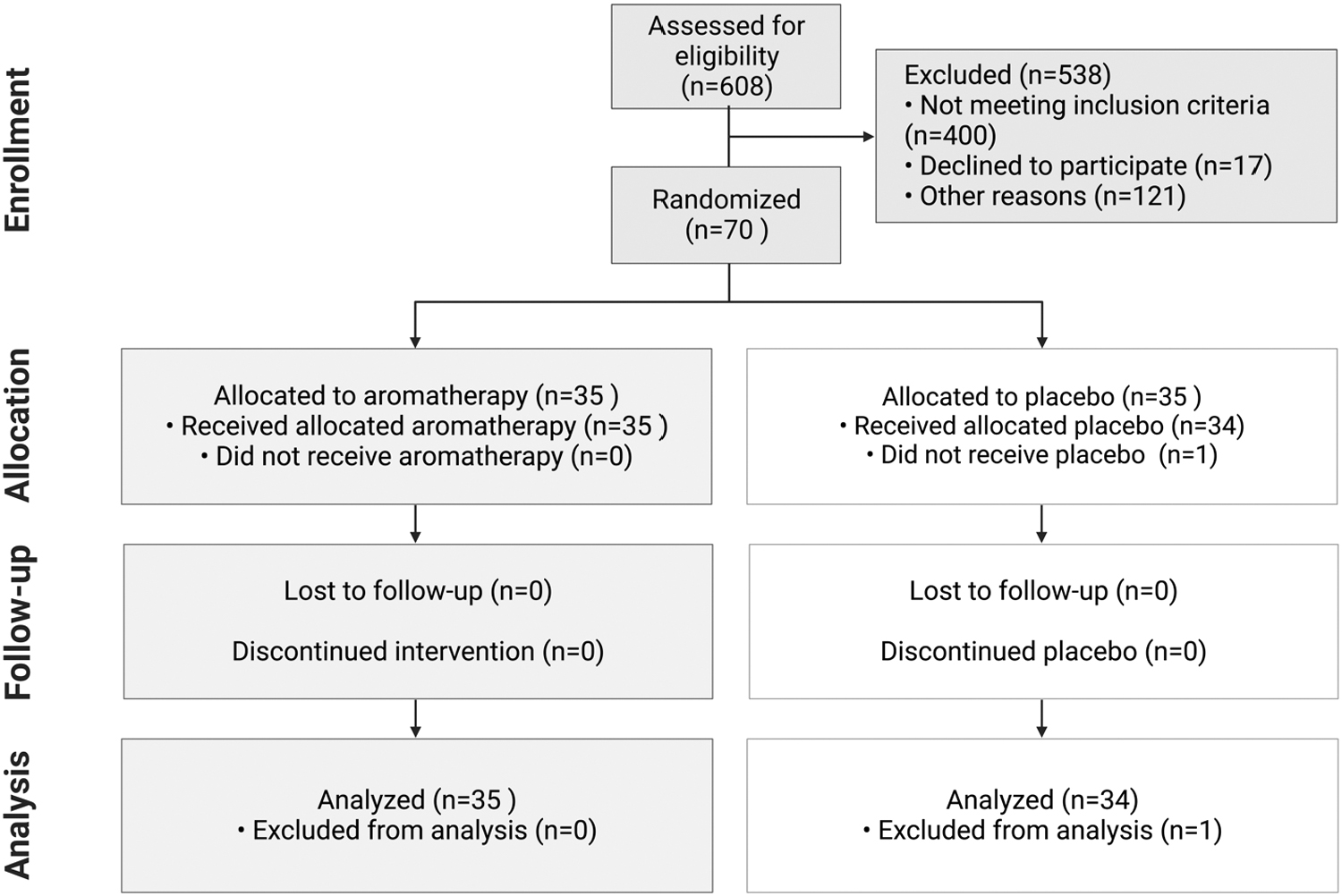
Study flowchart.
No demographic differences were found between groups (Table 1) in preoperative baseline demographics, including the HADS. No difference was found between the active and placebo groups on the primary outcome of time to discharge readiness (mean [SD]: 82 [15] vs. 89 [21] min, p = 0.131). The requirements of midazolam and antiemetics were not significantly different (Table 2). The aromatherapy and placebo groups did not differ in the proportion of subjects requiring rescue PONV medication in the PACU (aromatherapy: 0/35 [0%] vs. placebo: 1/34 [2.94%], p = 0.492) or in the proportion of subjects requiring opioids in the PACU (aromatherapy: 2/35 [5.71%] vs. placebo: 3/34 [8.82], p = 0.767).
Baseline Demographics and Clinical Characteristics
ASA, American Society of Anesthesiologists; BMI, body mass index; MEDD, morphine equivalent daily dose; NSAIDs, nonsteroidal anti-inflammatory drugs; PONV, postoperative nausea and vomiting; SD, standard deviation.
Summary of Primary and Secondary Outcomes
MEDD, morphine equivalent daily dose; PACU, postoperative acute care units; PONV, postoperative nausea and vomiting.
Pain intensity in PACU (aromatherapy: 0.33 [1.0] vs. placebo: 0.54 [1.1], p = 0.089), average PONV score in PACU (aromatherapy: 0 [0] vs. placebo: 0 [0.1], p = 0.324), or satisfaction in PACU (aromatherapy: 35/35 [100%] vs. 32/34 [94%] “very satisfied,” p = 0.239) was not significantly different between the treatment and placebo groups. The rate of adverse events was similar between both arms (aromatherapy: 1 [2.9%] vs. placebo: 2 [5.9%], p = 0.61).
Discussion
This is the first clinical trial investigating the effect of aromatherapy in clinically relevant outcomes in patients undergoing Port-A-Cath placement. The active aromatherapy patch demonstrated no advantage over the placebo patch; no difference was found in either primary or secondary outcomes. Although we observed a 7 min reduction in length of stay in PACU in favor of the aromatherapy group, we considered the difference not clinically relevant. At least two considerations should be made about the lack of effect of our study intervention. First, the duration of exposure before entering the OR was not controlled and was typically short in duration (2–5 min). This can explain the lack of effect of aromatherapy in our study. A longer duration (30 min) was effective in animal studies. 26
Second, patients received oxygen supplementation during the procedure via a facemask, which might have limited the adequate exposure to the active components of the aromatherapy patch. Future studies should investigate other application methods of essential oils, such as lotions underneath the nostrils.
Inhalation aromatherapy molecules act on olfactory receptors in primary olfactory neurons; upon activation of olfactory neurons, an action potential is generated and propagated via the olfactory tract, which projects from the lateral olfactory stria to the amygdala, a key structure of the limbic system involved in behavior and emotions. 27 Likely antianxiolytic mechanisms include interaction with N-methyl-D-aspartate (NMDA) or GABAA receptors, voltage-dependent sodium channels, voltage-dependent calcium channels, and glutamatergic and cholinergic neurotransmission. 27 Linalyl acetate and linalool are molecules found in lavender. The former has sedative actions, while linalool is considered a sedative, an NMDA antagonist, and an inhibitor of serotoninergic targets. 28,29 Yuan et al. proposed that both molecules also exert anti-inflammatory effects by inhibiting the activation of NF-kB and the release of proinflammatory cytokines (i.e., TNF-a, IL-1B, and PGE2). 30
The sedative effects of lavender aromatherapy have been assessed in multiple clinical studies. A meta-analysis by Perry et al. showed a lack of conclusive evidence to indicate aromatherapy for the treatment of preoperative anxiety. 31 However, more recent studies have shown promising results. For instance, Wotman et al. demonstrated a reduction in preoperative anxiety in ambulatory surgery patients treated with aromatherapy undergoing procedures in general otolaryngology. 32 A major limitation of the study was the lack of a placebo arm. Fayazi et al. had consistent findings in a randomized, placebo (water) controlled study on patients undergoing heart and abdominal surgery. 33 On the contrary, Trambert et al. also found a significant reduction in postprocedure anxiety levels in patients undergoing breast biopsies who received lavender-sandalwood aromatherapy. 34 Comparable results were reported by Jaruzel et al. in a pilot observational study of breast cancer patients and by Beyliklioğlu and Arslan in a randomized controlled trial. 35,36
Kim et al., in a study of acupuncture needle insertion, found that subjects who inhaled lavender oil for 5 min demonstrated decreased anxiety, less needle insertion pain, and Bispectral Index (processed electroencephalogram) changes suggestive of sedation. 37 Although using different molecules, Ni et al. showed decreased preoperative anxiety scores after using an ultrasonic aroma diffuser with either Bergamot essential oil or water vapor. 38 A randomized controlled trial assessed similar outcomes, such as recovery times and doses of sedatives used during a colonoscopy under the influence of either cherry-scented oxygen or regular oxygen, without finding any difference. 39
Peppermint oil has active molecules such as menthol and menthone. Grigoleit and Grigoleit found that menthol and menthone, the main constituents of peppermint oil, appear to act as smooth muscle relaxants through calcium channel blockade when the oil is orally ingested. 40 As an inhaled vapor, peppermint oil likely acts through another mechanism, such as by influencing neurotransmitter release at the chemoreceptor trigger zone of the medulla. 41 Hines et al., in a systematic review, found that aromatherapy appeared to be no better than placebo in preventing nausea, although there was some evidence that patients who had received aromatherapy required fewer antiemetic medications. 42 The quality of the included studies was moderate to very low, however. 42
More recently, Ahmadi et al. found peppermint oil aromatherapy effective in reducing nausea after abdominal surgery. 43 Maghami et al. found that peppermint oil aromatherapy effectively reduced nausea after open-heart surgery, although the peppermint oil was delivered via an in-line nebulizer in patients who remained intubated, limiting the study's generalizability. 44
Our study is generalizable to a large population of patients who undergo Port-a-Cath placement under MAC, however, it has limitations. First, patients and caregivers were not blinded to the treatment. Had any outcome difference been found, it could have been attributable to expectancy effects from lack of blinding; preoperative and intraoperative caregivers, surgeon, anesthesia providers, and subjects could easily determine group assignment. In addition, once in PACU, patients typically verbalized their treatment allocation, making blinding difficult. Second, although care was taken not to transfer any aromatherapy odors from the OR to the PACU, given the oily nature of the patches, some lingering aromas may have been occasionally transferred, thus blinding in the PACU was likely inconsistent. Third, it could be argued that the duration of the exposure to the aromatherapy effects was not sufficient to achieve sedation, as demonstrated by similar use of midazolam in both groups of patients.
Fourth, other methodologies for delivering aromatherapy and the scents used should be used in future studies. For example, eucalyptus (Eucalyptus globulus) has traditionally been used because of its anxiolytic and analgesic properties. 12,45,46 Finally, we were underpowered to detect small to detect small or medium effect sizes in our primary outcome.
In conclusion, the use of a combination lavender/peppermint patch produced no demonstrable outcome differences between groups; it is possible, although unlikely, that use of single-aroma patches would have produced outcome differences.
Footnotes
Acknowledgment
The authors thank Lei Feng, MS, for the statistical support.
Authors' Contributions
N.B.: conceptualization, methodology, and writing-original draft; D.S.C.: investigation, data curation, and writing—review and editing; J.J.G.-L.: investigation, data curation, and writing—review and editing; E.B.: investigation and writing—review and editing; C.H.: conceptualization, methodology, and writing—original draft; A.S.: investigation; J.P.C.: conceptualization, methodology, supervision, validation, and writing—original draft.
Author Disclosure Statement
The authors have no financial conflicts to disclose.
Funding Information
Tabs and placebos were donated by Beekley Corporation.
Supplementary Material
Supplementary Data
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.