
Abstract
Background:
Acupuncture is a widely practiced complementary and integrative health modality that has multiple clinical applications. The use of acupuncture in the United States is rapidly increasing. Although studies have shown the efficacy and effectiveness of acupuncture for various ailments, the integration of acupuncture into the U.S. health care system remains a challenge. Little is known about the factors affecting this integration.
Objective:
To provide a systematic review of the barriers and facilitators affecting the integration of acupuncture into the U.S. health care system.
Methods:
Four electronic databases were searched. Three independent reviewers were involved in the screening and data charting processes. Findings were synthesized and categorized into four levels based on the Social Ecological Model.
Results:
A total of 22 studies were included in the final review. The barriers and facilitators affecting the integration of acupuncture were mapped into four levels (individual, interpersonal, organizational, and policy). The most frequently reported barriers and facilitators were mapped into the Social Ecological Model constructs within the “Individual” level (i.e., beliefs and attitudes of acupuncture, and practical issues) and the “Organizational” level (i.e., credentialing, space and facility, referral system).
Conclusion:
This review has identified and synthesized the breadth of evidence on the barriers and facilitators to the integration of acupuncture into the U.S. health care system. Results of this review will guide future implementation studies to develop and test implementation strategies to integrate acupuncture into the U.S. health care system.
Introduction
Acupuncture is one of several treatment modalities of Traditional Chinese Medicine (TCM). 1 Acupuncture is a 3000-year-old practice that involves the insertion of very thin needles into specific points on the body for the purpose of restoring health and preventing disease. 2 Acupuncture can be used to treat a wide range of conditions. In the United States, the major reasons for the use of acupuncture are pain, depression, anxiety, headaches, arthritis, allergies, female infertility, insomnia, and frozen shoulder. 3 A meta-analysis drawing on data from 39 clinical trials and 20,827 patients showed that acupuncture is effective and has a sustained effect for treating chronic pain. 4 According to the American College of Physicians guidelines, evidence-based nonpharmacologic approaches, such as acupuncture, are recommended treatments for acute and chronic pain management. 5 Despite growing evidence supporting the efficacy of acupuncture for a range of conditions, 3,4,6 the integration of acupuncture as a complementary and integrative health (CIH) therapy into the U.S. health care system remains a challenge.
In the United States, the first acupuncture center opened in 1972; since then, the use of acupuncture has been on the rise. 7 Between 2002 and 2012, there was a sevenfold increase in the number of adults who reported using acupuncture, from 2.1 to 15.3 million, during their lifetime. 8 Recently, data from the National Health Interview survey showed that the utilization of acupuncture doubled from 2020 to 2022. 9 According to the 2023 American Hospital Association report, 21.7% (884 out of 4072) of hospitals offer CIH therapies, 10 most of them being acupuncture. The current use of CIH therapies in health care settings varies by region. New England has the highest usage, with 48.7% of hospitals offering CIH therapies, the Middle Atlantic with 36.7%, the East North Central with 33%, the Pacific with 27.4%, the South Atlantic with 22.1%, the Mountain with 21.3%, the West North Central with 16.9%, the East South Central with10.3%, and the West South-Central with 5.3%. While private insurance, as well as Medicaid and Medicare, has started to cover acupuncture, policy limits reimbursement to only a few health conditions, such as lower back pain. 11
To increase the use of acupuncture, it is important to identify what prevents uptake by health care organizations and patients and which factors support integration. There are numerous reasons that explain why acupuncture may not be adopted by the individual consumer, including a lack of awareness or knowledge of acupuncture, a fear of needles, concerns about side effects, and financial constraints. 12 With the recent incorporation of implementation science into acupuncture research, several studies 13 –16 found that patient reimbursement and affordability, lack of space or facilities in health clinics, and lack of referral systems are additional barriers that can influence the integration of acupuncture into the U.S. health care system. To the authors’ knowledge, there are no published reviews that summarize the barriers and facilitators affecting the integration of acupuncture into the U.S. health care system. To fill this gap, they completed a scoping review that was guided by the Social Ecological Model, 17 a model that allowed them to group factors according to the individual, interpersonal, organizational, and policy levels. The authors’ aim was to synthesize evidence affecting the broader integration of acupuncture into routine practice in the U.S health care system.
Methods
This review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analysis extension for Scoping Reviews (PRISMA-ScR). 18 The main research question governing this review was: “What is the existing evidence on the barriers and facilitators that affect the individual use and integration of acupuncture into the U.S. health care system?”
Data sources and search
The authors conducted a systematic search in Cumulative Index to Nursing and Allied Health Literature (CINAHL), Embase, PubMed, and Ovid Medline from 1976 through November 2022. They did not include China National Knowledge Infrastructure because they narrowly focused on studies relevant to the U.S. context. A search strategy was developed with an expert research librarian using the key terms, “acupuncture” and “integration.” The search strategy involved mapping subject heading terms related to the purpose of the study. Various terminologies have been used across the literature to describe the concept of implementation, such as “usage,” “implementation,” “feasibility,” and “acceptability.” A full search strategy for Medline is provided in Supplementary Data S1. The authors anticipated that the terms “barriers” and “facilitators” would only be discussed in the full text of the articles or described using other terms. They excluded “barriers” and “facilitators” in the initial search to enable a more thorough search of the published literature. To ensure a comprehensive synthesis of existing literature, the authors also manually extracted studies from review articles by screening the reference lists.
Inclusion and exclusion
Based on the definition of evidence implementation, 19 this review considered studies bridging the gap between knowledge generated through scientific research and its application in real-world health care settings. A study was included if (1) it was a quantitative or qualitative study reporting or assessing barriers and facilitators to the use of acupuncture in research clinical trials or barriers and facilitators to implementing acupuncture in real-world clinical settings in the United States and (2) it was published in the English language. Studies were excluded if they were (1) discussion papers or reviews, (2) only examining the efficacy and effectiveness of acupuncture, (3) conducted outside of the United States, and (4) conducted on animals. While the primary focus is on real-world implementation, understanding patient participation, including their beliefs and attitudes in clinical trials, provides valuable insights into the potential barriers and facilitators to the adoption and acceptance of acupuncture within the health care systems. By examining patient perspectives, experiences, and barriers in clinical trial settings, the authors can glean insights that inform strategies for effective implementation in real-world contexts. They excluded review articles in this scoping review and focused on mapping the raw data and perspectives presented in primary studies. This approach was chosen to prevent redundancy and mitigate the risk of biased interpretations.
Data extraction
All research records were imported into Covidence for screening. After deleting duplicates, two reviewers (I.A. and J.E.D.) independently screened the titles and abstracts for inclusion. Then the two reviewers met with the third reviewer (H.L.) to discuss the results and resolve any conflicts. Details of the screening and selection process are shown in the PRISMA flowchart.
A standardized charting form was developed using Microsoft Excel to identify key characteristics of each study, as well as barriers and facilitators to the implementation and use of acupuncture. For each article, the reviewers extracted information about authors, publication year, objectives, study design, study setting, intervention characteristics, barriers, and facilitators of using and implementing acupuncture. H.L. independently charted all the included articles, while I.A. and J.D. each charted 50% of the included articles. Discrepancies noted during study selection and data extraction were discussed with another author and agreement was obtained.
Synthesizing and coding results
The barriers and facilitators were mapped into four levels (individual, interpersonal, organizational, and policy) based on the Social Ecological Model. 17 The authors chose to use the Social Ecological Model because this framework provides a comprehensive understanding of factors that influence health and well-being, including people’s interactions with their physical and sociocultural environments. It can be used to integrate components of other theories and models in the future. H.L. deductively coded the extracted data by mapping determinants (i.e., barriers or facilitators) into four levels. Coded data that were mapped onto each construct were listed, presented in a tabular form, and grouped into subcategories. The synthesized results were then organized and categorized in a single level exclusively, based on the four levels.
Results
Search of the databases identified a total of 10,185 publications after removal of duplicates. From title/abstract screening, 10,150 articles were excluded, and 35 articles remained for full-text screening. After full-text screening, 22 publications were selected to comprise the set of studies to be reviewed (PRISMA flowchart in Fig. 1).
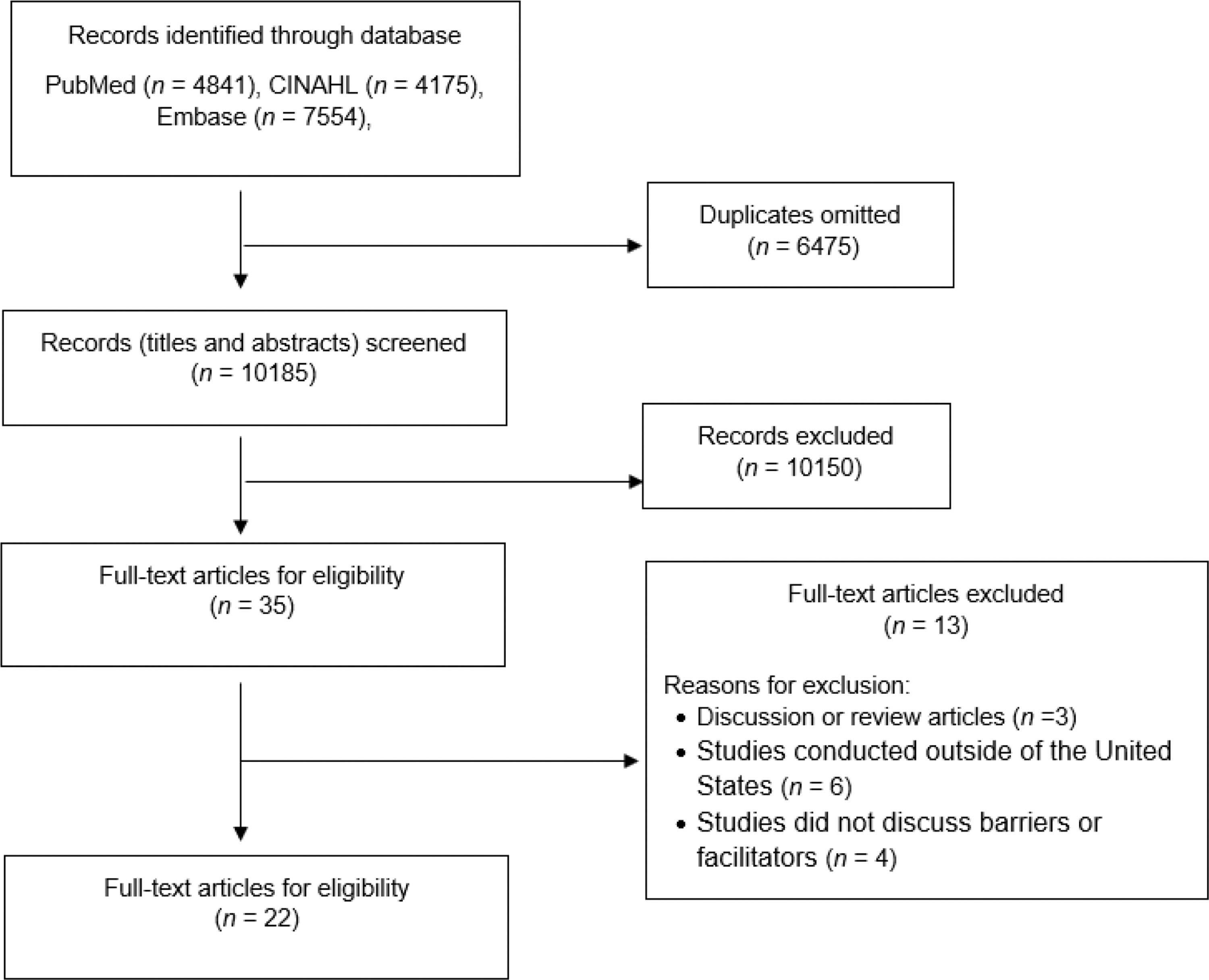
Study selection process.
Characteristics of included studies
The included publications employed the following three types of research methods: quantitative (n = 13), qualitative (n = 5), and mixed methods (n = 3). The authors only included and reviewed studies in the United States because the implementation process was expected to vary by each country and policy. Most of the studies discussed barriers and facilitators related to using an acupuncture intervention (n = 19), battlefield acupuncture (n = 1), group acupuncture and yoga (n = 1), and cognitive behavioral therapy and acupuncture (n = 1). The majority were conducted with patients (n = 13). Some studies also included other stakeholders such as physicians and health care providers (n = 7) and acupuncturists (n = 2). Table 1 shows a summary of the characteristics of the included studies.
Characteristics of Included Studies
CBT-I, cognitive behavioral therapy for insomnia; FQHC, federally qualified health center; PCOS, polycystic ovary syndrome; RCT, randomized controlled trials; UCSF, University of California San Francisco.
Barriers and facilitators
A summary of barriers and facilitators is presented in Table 2. Findings are organized according to the four levels of the Social Ecological Model.
Summary of Barriers and Facilitators
Individual level
Knowledge and attitudes
The most pervasive barrier to the use of acupuncture as a treatment option was a lack of knowledge and awareness of acupuncture (n = 6). 12,13,16,20,21,25 Lack of awareness was also a factor for physicians and other allied health professionals (n = 1) 21 and patients who were medically underserved (n = 1). 20 Three studies showed that both providers and the general population were unaware of evidence supporting the use of acupuncture (n = 3). 12,16,25 Negative perceptions and beliefs about acupuncture arose when people did not have a clear understanding of acupuncture (n = 2). 23,24 Participants reported having fears about the side effects of acupuncture (n = 1). 12 In one cross-sectional study, 4.7% of breast cancer survivors expressed concerns about whether acupuncture would interfere with their conventional treatment plan (n = 1). 12 Because of the lack of knowledge about acupuncture (n = 1), 13 some clinicians were uncertain when to refer patients to acupuncture during the trajectory of a disease and treatment. 27 In one qualitative study, African American participants expressed their negative attitudes toward placebo and worried that their condition might worsen if they were randomized to a placebo group (n = 1). 23
There are several factors that appear to facilitate the uptake of acupuncture, such as describing its reported benefits (i.e., reduced reliance on medication, noninvasive with minimal side effects) (n = 3), 15,20,23 increasing awareness and change in attitude (n = 2), 13,26 educating participants about the role of acupuncture (n = 1), 27 and providing well-documented evidence in support of acupuncture (n = 1). 26 Two studies from primary care settings (n = 2) addressed knowledge gaps by showing patients a short audiovisual and providing written materials to introduce acupuncture. 14,23 Other studies used patient testimonials about their experiences with acupuncture to support education of patients (n = 2). 23,25
Acceptability
Dislike or fear of needles (n = 4) was the most commonly cited reason affecting the acceptability of acupuncture as a treatment option. 12,15,23,25 Lack of interest or refusal to try acupuncture was another barrier (n = 2). 16,29 Results from one quantitative survey showed that even when physicians referred patients to acupuncture for pain management, 5.6% of them refused to try it. 16 Findings from another quantitative survey showed that lack of interest in acupuncture was a significant barrier toward participation in acupuncture trials among breast cancer survivors. 29
One qualitative study showed that openness was a characteristic associated with acceptability by patients attending a family medicine clinic (n = 1). 15 Similarly, openness affected the willingness of hospital providers and staff to learn about acupuncture (n = 1). 30
Previous experience
When people received acupuncture for chronic low back pain, osteoarthritis, weight management, palliative care, and pain management, and reported they benefited from acupuncture, felt better in a more holistic way, physically and psychologically, they were more likely to continue to get acupuncture (n = 3). 20,23,27
Practical issues
Travel difficulty due to distance (n = 2), 23,29 treatment time burden or difficulty fitting acupuncture treatments in with a demanding job and home responsibilities (n = 5), 12,13,15,23,29 and transportation and limited parking (n = 6) 12,20,23,29,32,33 were commonly cited barriers to the use or continued use of acupuncture. Findings from a qualitative study of six people with sickle cell disease showed that unpredictable acute pain episodes negatively affected attendance at appointments (n = 1). 33 When flexible scheduling, including evening sessions (n = 5), 14,26,29,32,33 childcare (n = 1), 29 and free parking (n = 2), 23,33 was provided, people were more likely to continue to use acupuncture. 35
Social determinants of health
Other barriers were lack of ability to find acupuncturists (n = 3) 12,20,34 and challenges faced by low socioeconomic and/or immigrant or minority people, such as stress and mental health issues (n = 1). 26 When satellite acupuncture clinic sites 23,29 were added, including a clinic that opened near an inner city hospital, 30 more people were able to access these services enabling medically underserved patients to more easily receive treatment (n = 3). 23,29,30 When an urban hospital collaborated with an externship site, including inviting students and faculty from an acupuncture school to conduct acupuncture at an urban hospital (n = 1), 30 it resulted in lower cost of care and enabled the collaborative care to be affordable to a medically underserved population.
Interpersonal
Health care providers reported that given their limited time with patients, it was difficult to fully explain and promote acupuncture to patients during busy clinical hours (n = 2). 13,27 A pilot study that integrated acupuncture and yoga into chronic pain treatment plans showed that communication issues such as language barriers(n = 1) 26 were problematic and resulted in difficulties in communication. A quantitative study reported that intracultural communication and use of different medical terms by primary care providers and acupuncturists can influence the integration of acupuncture (n = 1). 14
When effective communication and positive relationships between patients and acupuncturists were noted (n = 2), 24,26 patients had more satisfaction with treatment and felt that acupuncture was more effective. When bilingual staff and translation services were provided (n = 1), 26 it facilitated the implementation of acupuncture within a community health center. When free acupuncture was offered to hospital staff (n = 1), 35 trust, defined as a smooth working relationship, was enhanced. Trust between patients and acupuncturists was developed by working in culturally nuanced ways with non-English-speaking patients (n = 1) 35 and adapting language and culture when communicating with patients of different backgrounds (n = 1). 35 One quantitative study showed that when acupuncturists were optimistic about treatment effectiveness and communicated this to patients, they were more likely to have satisfaction with acupuncture. 24
Organizational
There were several organizational factors that influenced the integration of acupuncture into medical treatment. First, there were not enough trained and qualified acupuncturists (n = 4) to provide acupuncture services in family medicine clinics, 15 academic hospitals, 22 and community health centers, 14,26 Second, when community health centers, 14 family medicine clinics, 15 a cancer center, 13 and a teaching hospital 16 did not have the space or facilities (n = 4), providing acupuncture was not possible. Also, when hospital human resources were unfamiliar with the credentialing process and the procedures necessary to process the paperwork for the hiring of acupuncturists (n = 4), 13,14,36,37 it inhibited the availability of acupuncture services.
Two studies conducted in a cancer center and a community health center reported that they did not have detailed referral systems to refer patients for acupuncture (n = 2). 13,14 A quantitative study showed that lack of malpractice insurance coverage and problems with billing and coding issues were barriers to integrating acupuncture into clinical practice (n = 1). 36 A qualitative survey study of pain medicine fellowship directors showed that many academic centers do not have qualified teaching personnel to provide formal didactic education to pain medicine fellows (n = 1). 22 The study’s conclusion was that group acupuncture can be a good model to treat chronic pain among underserved patients; however, community health centers did not offer group acupuncture (n = 1). 26
There were several facilitators that could promote the integration of acupuncture. When credentialing and privileging procedures were streamlined (n = 4), 14,15,30,37 it facilitated acupuncturists practicing in health care settings. When institutional leadership was supportive and made acupuncture central to their mission (n = 4), 15,21,27,30 acupuncture had higher acceptability and greater utilization in hospital practices. Having champions that advocated for acupuncture and its benefits, leadership “buy-in” increased. 15 When standardized and uniform electronic health record (EHR) codes were developed (n = 2), 14,37 it facilitated communication among acupuncturists and medical providers, and normalized acupuncture as an important aspect of care. When providers were easily able to make referrals for acupuncture care (n = 2), 14,26 it increased patients’ awareness of acupuncture.
Several facilitators at the logistic level were reported. When group acupuncture was provided in community-based locations (n = 2), 32,34 it increased the frequency of treatments, reduced the cost of acupuncture, and reduced access barriers. When hospitals and acupuncture schools were in close proximity to one another (n = 1), 30 it facilitated the integration of a faculty-supervised student acupuncture clinic into an urban hospital. When acupuncture was provided in the primary care setting (n = 1), 14 patients found acupuncture services to be more acceptable in their home medical clinics. A pilot study (n = 1) in veterans showed that if acupuncture was provided in a more-relaxing environment, that each patient had a separate room for acupuncture, acupuncturists were the same gender as the patients, or acupuncture was provided in large quiet rooms and the rooms had dimmed lights, it was helpful. 32
Policy
Cost (n = 8) 12,13,20,21,27,30,34,36 and lack of health insurance reimbursement (n = 6) 12,14,16,26,28,30 prevented patients from accessing acupuncture and providers from recommending it. Policy changes at the institutional level, such as formulating new and revised pain assessment and management standards that require provision of nonpharmacologic therapies for pain treatment, are important (n = 1). 26 Creating career enhancement incentives for acupuncturists (n = 1) 26 is an important internal facilitator for the implementation of acupuncture into community health centers. When policy changes at an external level occurs, such as reducing the costs of acupuncture (n = 5), 14,21,28,30,34 and improving insurance coverage for acupuncture through the Centers for Medicare and Medicaid emerge value-based reimbursement models (n = 2), 13,26 access to acupuncture increases.
Discussion
This review synthesized available evidence and used the Social Ecological Model to categorize the various barriers and facilitators related to and affecting integration of acupuncture into the U.S. health care system. Only a few implementation studies of acupuncture have been conducted to test the integration of acupuncture into the U.S. health care system. Therefore, this review examines both the combined barriers and the facilitators for the use of acupuncture by individuals and the integration of acupuncture into the U.S. health care system. Considering the barriers and facilitators across the four levels, the individual and organizational levels were most frequently reported. The results of this study will guide future implementation studies to optimize strategies to effectively implement acupuncture into real-world practice, and ultimately influence policy changes.
Understanding individual needs and barriers is essential
There are numerous reasons why acupuncture may not be adopted by individuals, including a lack of awareness or knowledge of acupuncture, fear of needles, concerns about side effects, and financial constraints. 12 Several studies show that increasing awareness and education about the benefits of acupuncture lead to increased utilization uptake. 20 When access to affordable and convenient acupuncture services is offered, people use it. 30
Having a comprehensive understanding of the history, philosophy, and terminology of acupuncture, as well as how it works, what it feels like, possible side effects, and evidence supporting its use, is foremost to its acceptance by patients and health care providers. For patients, effective strategies should be implemented to enable their understanding of the benefits and side effects of acupuncture. Using audiovisual material briefings to provide knowledge of acupuncture in primary care settings has been shown to be beneficial. 14,23 For patients who like to talk with and learn from one another, having them watch other patients’ testimonials to learn about their experiences with acupuncture is also a beneficial strategy. 23,25 For patients who have temporary worsening of symptoms or feel fatigued after acupuncture, 38 it is important to educate them in advance that both of these are common following acupuncture. These symptoms are part of the healing process and a positive sign that the acupuncture is working. 39 For health care providers, Bhandiwad 14 noted that many health care providers may be unaware of the current evidence supporting the use of acupuncture and may not understand its unique philosophy and terminology. This lack of understanding may impact their willingness to refer patients for acupuncture. Educating providers on the current evidence supporting acupuncture, teaching them acupuncture terminology, and offering indications for acupuncture and referrals are important strategies to increase health care provider awareness. Educating health care providers about acupuncture can lower opioid prescribing and lessen depersonalization of patients. 40 If providers are suspicious or have biases regarding the use of acupuncture, educating them on the evidence that validates acupuncture as an effective medical therapy can change their attitudes and therefore increase their likelihood of referring patients.
Trust, good communication, and support are indispensable
Health care providers, including acupuncturists, play an important role in communicating information about acupuncture to their patients. Most patients are willing to listen to and trust their providers. Street et al. 24 found that acupuncturists’ communication of optimism about treatment can greatly increase patients’ satisfaction and have therapeutic value. Health care providers can use patient-centered communication strategies to engage patients in discussions about acupuncture. 41 Shared decision-making, making conscious word choices, and explaining various aspects of acupuncture (e.g., what to expect, what happens when acupuncture is administered) and not just how effective the intervention is may increase acupuncture use.
Building trust is not only vital between patients and acupuncturists, but it is also important between acupuncturists and health care providers and staff. Sometimes, it is easier to build trust between people with the same racial and ethnic background. Having a racially and ethnically diverse health care team will facilitate the understanding of the needs of diverse patient populations. Providing a free acupuncture session for health care providers is a key strategy to establish trust between acupuncturists and other health care providers. 35 By experiencing the intervention, they can tell their patients about the positive effects of acupuncture, create camaraderie, and increase staff willingness to actively support the use of acupuncture.
Organizational changes
Many barriers at the organizational level have been identified, including a lack of space or facilities in health clinics, 13 –16 a lack of referral systems, 13,14 and a lack of credentialing and privileging procedures. 13,14,36,37 However, few studies have investigated how acupuncture can be successfully integrated into health care settings. Therefore, dedicated resources, such as leadership support, space and facilities, credentialing, as well as the EHR system, should support the integration process. This will allow organizations, health care providers, and staff to familiarize and adapt to their use.
Health care administrators such as chief executive officers and chief financial officers should be aware of the benefits and take steps toward the integration of acupuncture into health care settings. Based on identified barriers and facilitators, several implementation strategies can be tested during the integration process. The authors recommend establishing a hospital credentialing process for physicians who are board certified in medical acupuncture through the American Board of Medical Acupuncture and credentialing licensed acupuncturists for hospital privileges. 14 Adapting acupuncture to current space allocations and health care providers’ schedules will enable logistical and administrative changes to be made that foster the growth of acupuncture services within a health care setting. 14 It is also important to formalize referral pipelines from the traditional health system to community practices (i.e., acupuncturists with private practices in the community and traveling acupuncturists administering care to community groups). For the EHR, the standardization and adoption of uniform EHR codes will enable acupuncture referrals and billing to occur. 14,37 Templates in the EHR will also facilitate effective communication among acupuncturists and health care providers and normalize documentation of acupuncture and other TCM modalities. The Osher Center for Integrative Medicine at the University of California San Francisco has developed a template housed in the Epic Community Library to support the interprofessional communication between Chinese Medicine practitioners and other providers. 31 Also, requiring health care providers to participate in a systematic training program where they are taught the fundamentals and use of acupuncture from experienced and well-qualified acupuncturists will foster acupuncture referrals and the establishment of acupuncture services within a health care setting. 37
Acupuncture clinics tend to be concentrated in upper-income neighborhoods. Few acupuncture clinics are located in underserved communities. 42 As most people receive health care in their local communities, satellite integrative services or community nursing homes can be sites for providing acupuncture. Community-based group delivery models can be used to lower costs. 34 One study showed that it was feasible and acceptable to deliver acupuncture in a community-based group for medically underserved populations. 26 More research is needed to study the implementation of acupuncture in medically underserved populations who often receive their health care at federally qualified health centers or community clinics.
Policies are slowly changing
The trend toward private insurance coverage of acupuncture, especially for pain-related conditions, is increasing. In 2020, the Centers for Medicare and Medicaid Services (CMS) started to cover acupuncture for Medicare patients with chronic lower back pain. 11 A total of 23 state Medicaid programs have mandated acupuncture coverage for some conditions. Even though Medicare, Medicaid, and some private insurance companies have started to cover acupuncture, they currently are limited in their reimbursement for just a few health conditions. Medicare only covers chronic lower back pain. In Ohio, the Medicaid program only covers migraines, neck pain, cervical pain, shoulder pain, and acute postoperative pain. Rhode Island Medicaid requires frequent emergency department visits to qualify for coverage. 11,43 Private insurance coverage for acupuncture improves patients’ access to care and increases beneficial outcomes. 44 However, some insurance companies claim that lack of providers, lack of evidence for clinical efficacy, and low cost–benefit ratio are some of the main challenges preventing the integration of acupuncture. 45 To minimize these claims and promote insurance coverage, efforts are needed to gather and disseminate evidence on the efficacy of acupuncture. Conducting cost–effectiveness analyses of acupuncture for various health conditions is an important component for providing insurance companies with the evidence needed to reimburse for acupuncture services. Also, efficacy trials can focus more on long-term symptom control and the broader impact that acupuncture has on overall health.
In addition, the minuscule rate of payment by the CMS for patients receiving acupuncture for low back pain with Medicare coverage is unsustainable for acupuncturists, as it fails to cover the costs associated with providing quality care. Consequently, this financial strain can impact the viability of private practices and other organizational levels within the acupuncture community, limiting their capacity to deliver consistent and effective treatment to Medicare patients. This issue underscores the need for policy reforms or adjustments to ensure that reimbursement rates align more closely with the actual costs of providing acupuncture services at the market, thereby facilitating improved access to care for patients with Medicare and Medicaid while sustaining the viability of acupuncture practices.
To improve health care policy coverage of acupuncture, acupuncture leaders can work together to review scientific evidence, develop guidelines, and make recommendations about the use of acupuncture. The National Comprehensive Cancer Network guideline is a good prototype that promotes broader coverage of drugs and biologics during cancer treatment. 46
Limitations
There are several limitations of this review. In their search protocol, the authors used different terms to describe integration, implementation, and usage for the initial search. Due to the large number of articles that were included in this review, they had to screen each article by title and abstract. Therefore, relevant studies might have been missed or excluded. Also, this review combined barriers and facilitators for the use of acupuncture by individuals and the integration of acupuncture into health care settings. The authors expanded the scope of this review by including studies that discussed barriers and facilitators to participating in acupuncture trials, or attitudes regarding the use of acupuncture. They included any quantitative or qualitative study reporting the application and evaluation of any enabling strategy aimed at addressing barriers and facilitators to the use and implementation of acupuncture in the United States. In addition, the authors only searched studies in four common databases. Other important databases, such as Alt Health Watch, could have been explored to broaden the scope of the search and capture additional relevant information. In future studies, expanding the search to include Alt Health Watch could certainly enhance the comprehensiveness of the investigation.
In this review, half of the studies used mixed methods to identify barriers and facilitators. Half of the studies evaluated the feasibility of implementing acupuncture treatment as the primary aim and covered barriers and facilitators in the Discussion section. Only one implementation study was guided by an implementation framework. Research in the implementation of acupuncture is an area that is underdeveloped. Therefore, the authors can only summarize their results based on the current state of the literature, which may influence the quality of this review. However, this scoping review is important. It will serve as a foundation as well as reinforce the need for future implementation studies in acupuncture. More studies are needed that use implementation frameworks, such as the Consolidated Framework for Implementation Research, to identify the determinants for the implementation of acupuncture and to develop implementation strategies in real-world health care settings.
Summary
Given the growth of patient usage of acupuncture, acupuncture efficacy research studies, and payer coverage, 47 further understanding of the barriers and facilitators for improving access to acupuncture services and increasing its utilization is important. Implementation studies that test multilevel implementation strategies are urgently needed to promote the integration of acupuncture into the current U.S. health care system. Results of this study can be used to optimize strategies to effectively implement acupuncture into clinical practice, and ultimately influence policy changes.
Footnotes
Acknowledgment
The authors thank Dr. Rebecca Raszewsk, biomedical librarian and informationist, at University of Illinois Chicago, for her assistance in conducting the literature search.
Authors’ Contributions
H.L., J.E.D., and I.A. were responsible for data acquisition, interpretation, and drafting the article. J.M.S. and C.L.P. critically revised the work for important intellectual content. O.D., A.D.B., L.B., M.O.E., M.R.K., T.-Y.L., M.W.M., V.A.D.M., R.E.M., N.S., D.J.W., and A.Z.D. were included in the article drafting, validating, and also critically revised the work. All authors provided final approval of the version to be published and agree to be accountable for all aspects of the work.
Author Disclosure Statement
The authors have nothing to disclose and have no conflicts of interest.
Funding Information
This work was supported within the National Institutes of Health (NIH) Pragmatic Trials Collaboratory through the NIH HEAL Initiative under award numbers UG3 AT011265 and UH3AT011265 administered by the National Center for Complementary and Integrative Health (NCCIH). The work received logistical and technical support from the PRISM Resource Coordinating Center under award number U24 AT010961 from the NIH through the NIH HEAL Initiative. This work was also supported by Grant Numbers K24 AT011995 from the NCCIH and the National Institute of Neurological Disorders and Stroke (NINDS), R34 AT012084 from NCCIH, R21 CA277153 from the National Cancer Institute (NCI), R01 HD091210 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), and R01 NR020376 from the National Institute of Nursing Research (NINR). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NCCIH, NINDS, NCI, NICHD, NINR, or the NIH or its HEAL Initiative.
Supplementary Material
Supplementary Data S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.