
Abstract
Introduction:
During the COVID-19 pandemic, health care workers (HCWs) experienced increased anxiety, depression, loneliness, and other mental health issues. HCWs need additional resources to cope with the mental health impact of their work. Yoga techniques could be helpful strategies to manage different stressors during times of uncertainty.
Methods:
This prospective, single-arm, trial examined the effects of a brief pranayama yoga practice on the wellbeing of HCWs during the height of COVID-19. HCWs were recruited through announcements and institutional websites at a large major cancer center in the southern United States. A short, prerecorded, 5-min breathwork video intervention called “Simha Kriya” was provided to participants, and they were encouraged to practice one to two times daily for 4 weeks. Participants completed self-report instruments at baseline and weeks 1 and 4, including: (1) Perceived Stress Scale (PSS); (2) Brief Resilient Coping Scale (BRCS); and (3) a questionnaire assessing the experience of COVID-19 among HCWs that had five subscales. HCWs also conducted a measure of breath holding time. Paired sample t-tests and mixed-effects analysis of variance models examined changes over time.
Results:
One hundred participants consented to the study, with 88 female, 60 white, 39 worked remotely, and 27 were clinical staff. Sixty-nine participants provided data at week 1 and 56 at week 4. Participants' adherence to the breathing exercises between weeks 1 and 4 was similar, with a mean of six times per week. At week 4, there were significant decreases in the COVID-19 Distress score (p < 0.0001) and COVID-19 Disruption (p = 0.013), yet no changes in the PSS. There were also significant increases in COVID-19 Stress Management (p = 0.0001) and BRCS scores (p = 0.012), but no changes in Perceived Benefits of COVID-19 and no changes in breath holding time.
Discussion:
Brief yoga-based breathing practices helped reduce pandemic-specific stress, improved resilience, and stress management skills in HCWs.
Trial Registration Number:
NCT04482647
Introduction
During the COVID-19 pandemic, health care workers (HCWs) experienced increased anxiety, depression, loneliness, and other mental health issues. 1,2 During the beginning months of the pandemic, HCWs experienced numerous stressors and challenging working conditions that contributed to worse quality of life and mental health, including increased risk of COVID-19 exposure to themselves and their loved ones, 3 overworking, insufficient protective equipment, extended working hours, and uncertainty about the pandemic, to name a few. 4,5 The psychological distress experienced by HCWs was similar to other pandemics, such as SARS, H1N1, MERS, and Ebola. 6 Studies found HCWs needed additional resources to cope with the mental health impact of their work during COVID-19. 7 Yoga and other behavioral techniques could be helpful strategies to manage different stressors during times of uncertainty.
Yoga is an evidence-based mind–body practice that originated in India and includes various poses and breathing techniques to improve physical and mental health. The breathwork component of yoga, called pranayama, has numerous benefits to the respiratory system and overall health. 8 A systematic review of 669 studies examining the therapeutic effects of pranayama confirmed a significant benefit on cardiorespiratory/pulmonary conditions, such as bronchial asthma and chronic obstructive pulmonary disease. 8 Psychological benefits were also associated with pranayama interventions in multiple studies. 9,10 Because COVID-19 is a respiratory disease, the current study utilized pranayama for HCWs. A preliminary article reported the feasibility and subjective usefulness of this pranayama yoga intervention among HCWs. 11 Specifically, at week four, 74% of HCWs “agreed or agreed strongly” that the pranayama intervention increased feelings of relaxation and peacefulness and that they found it useful. 11
The current study examined changes in perceived stress, resilience, and COVID-19-specific factors, such as distress, disruption in activities, financial concerns, perceived benefits, perceived stress management skills, and breath holding time. We hypothesized that practicing pranayama would help HCWs cope with psychological distress and increase breath holding time during the COVID-19 pandemic.
The study was approved by The University of Texas MD Anderson Cancer Center Institutional Review Board (2020-0483).
Materials and Methods
This was a prospective, single-arm, trial conducted at a comprehensive cancer center in the southern United States, and details of the procedures were published elsewhere, 11 and is registered with ClinicalTrials.gov (NCT04482647). Participants were hospital employees recruited through internal employee announcements and institutional websites. Exclusion criteria included: (1) Epilepsy; (2) brain aneurysm; (3) pregnant or trying to get pregnant; (4) brain bleeding in the past year; (5) greater than 70 years of age; or (6) recent abdominal surgery and not yet cleared for exercise. After answering screening questions, eligible participants were given information about the study procedures, and electronic consent was obtained. Self-reported outcome measures were completed at the time of study recruitment, and on a weekly basis for 4 weeks after starting the study. Surveys were completed using participants personal/work electronic devices and stored on a Research Electronic Data Capture (REDCap) database.
Simha Kriya yoga
Participants were given access to a video with detailed instructions of the breathing practice developed by the Isha Institute of Inner Sciences. The “Simha Kriya” meditation practice was chosen because it is easy to learn and can be completed within 5 min. Briefly, it consisted of three components: (1) Forced exhalation with tongue sticking out (dog-like breathing) for 21 times at a normal pace; (2) forced exhalation with tongue rolled upward for 21 times at a normal pace; and (3) breath retention for 30–60 sec. This was followed by a 2-min meditation for a total of 5 min. Participants were asked to do the breathing practices one to two times daily for 4 weeks. Written instructions were provided and the PI (S.N.) provided weekly support sessions through zoom based on feedback of the participants who started early on. The study team's email was available to all participants to ask any questions.
Adherence
To measure adherence, participants kept a record of their practice each day reporting when, how many times a day, and how many days a week they practiced, throughout the 4-week study period.
COVID-19-specific stress among HCWs
Participants completed the COVID-19 Practical and Psychosocial Experiences (COVID-PPE) questionnaire. 12 The measure was adapted from items from existing measures assessing the impact of pandemics (e.g., H1N1), major stressors, such as the September 11th attacks, hurricanes and other national disasters, and instruments commonly used to assess relevant constructs, such as distress, social support, and benefit finding. 13 –15
For this study, we used a modified version using 27-items that are part of five subscales measuring how COVID-19 impacted the participants in the areas of: (1) Distress (11 items); (2) disruptions to daily activities and social interactions (4 items); (3) financial hardship (4 items); (4) perceived benefits (4 items); and (5) perceived stress management skills (5 items). Participants were asked to rank statements on a Likert-like scale (from 1 to 4) from “strongly disagree” to “strongly agree.” The internal consistency of the PPE subscales ranged from α’s = 0.609 to 0.894. 12 Psychometric analyses suggested that there was insufficient evidence to combine items into a single overall total impact score, therefore, the individual subscales and individual questions are reported.
The Perceived Stress Scale-4
The Perceived Stress Scale-4 (PSS-4) measures nonspecific, appraised ongoing stress. It has four items with scores ranging from 0 to 4 that ask perceptions about the ability to manage ongoing challenges. Scores range from 0 to 16 with higher scores indicating more stress. 16
Brief Resilient Coping Scale
The Brief Resilient Coping Scale (BRCS) includes four items: (1) I look for creative ways to alter difficult situations; (2) regardless of what happens to me, I believe I can control my reaction to it; (3) I believe I can grow in positive ways by dealing with difficult situations; and (4) I actively look for ways to replace the losses I encounter in life. 17 The participants rated each item on a 5-point scale ranging from 1 = strongly disagree to 5 = strongly agree.
Breath holding time
At baseline and the end of each week, participants were asked to use the stopwatch on their smartphones to count how many seconds they could hold their breath. Participants were told to first empty their lungs as much as possible with an extended exhalation pulling in their diaphragm using abdominal breathing. They then inhaled fully extending their diaphragm out and started timing how many seconds they could hold their breath and recorded that number. After a 2-min rest period they repeated the process and recorded the second number.
Statistical analysis
The original sample size for feasibility was set at N = 50. With a sample size of 50, the study had 80% power to detect a difference in mean of 0.404 standard deviation (SD) units between baseline and a time point after baseline, using a paired t-test with a 0.050 two-sided significance level. However, within the first 2 days of recruitment over 70 HCWs showed interest in the study. To support more HCWs, the sample size was expanded to N = 100. With N = 100, the difference in mean SD units detectable dropped to 0.283.
Frequencies at baseline and follow-up and completion percent were used to describe participant demographics. Survey scores were summarized as mean with SD at each time point. Mixed-effects analysis of variance models related each survey item to time point (baseline and 4-week time point postintervention), blocking on a subject to control for repeated measures and missing data bias. An expanded mixed-effects model set of analyses related each survey item to an interaction between time and work status (remote work/in person), and between time and clinical/nonclinical staff, with changes between time points, work status, and clinical/nonclinical status, and assessed by Hommel-adjusted contrasts.
A 95% level of statistical confidence was assumed in all statistical testing. All statistical modeling was performed using R statistical software version 4.2.2 (R Core Team, 2022).
Results
Participant characteristics
Study participants took part in this research from July to November 2020. Detailed participant characteristics can be found elsewhere. 11 Briefly, there was enthusiasm to take part in the study, with 217 participants showing interest in participating. The first 90 participants were recruited within 1 month, and 100 participants within 2 months. At baseline, 88 were female, 60 were white, 71 were educated with a master's degree or higher, 39 worked remotely, and 27 were clinical staff. Of the 100 participants consenting to the study, 2 withdrew before the baseline, leaving 98 participants. At weeks 1 and 4, 69 and 56 participants provided data, respectively (Fig. 1). A greater percentage of people who worked remotely completed the follow-up assessments compared with nonremote workers (p = 0.025). There were no other statistically significant differences on any other demographic or psychosocial baseline measure comparing participants with and without follow-up data.
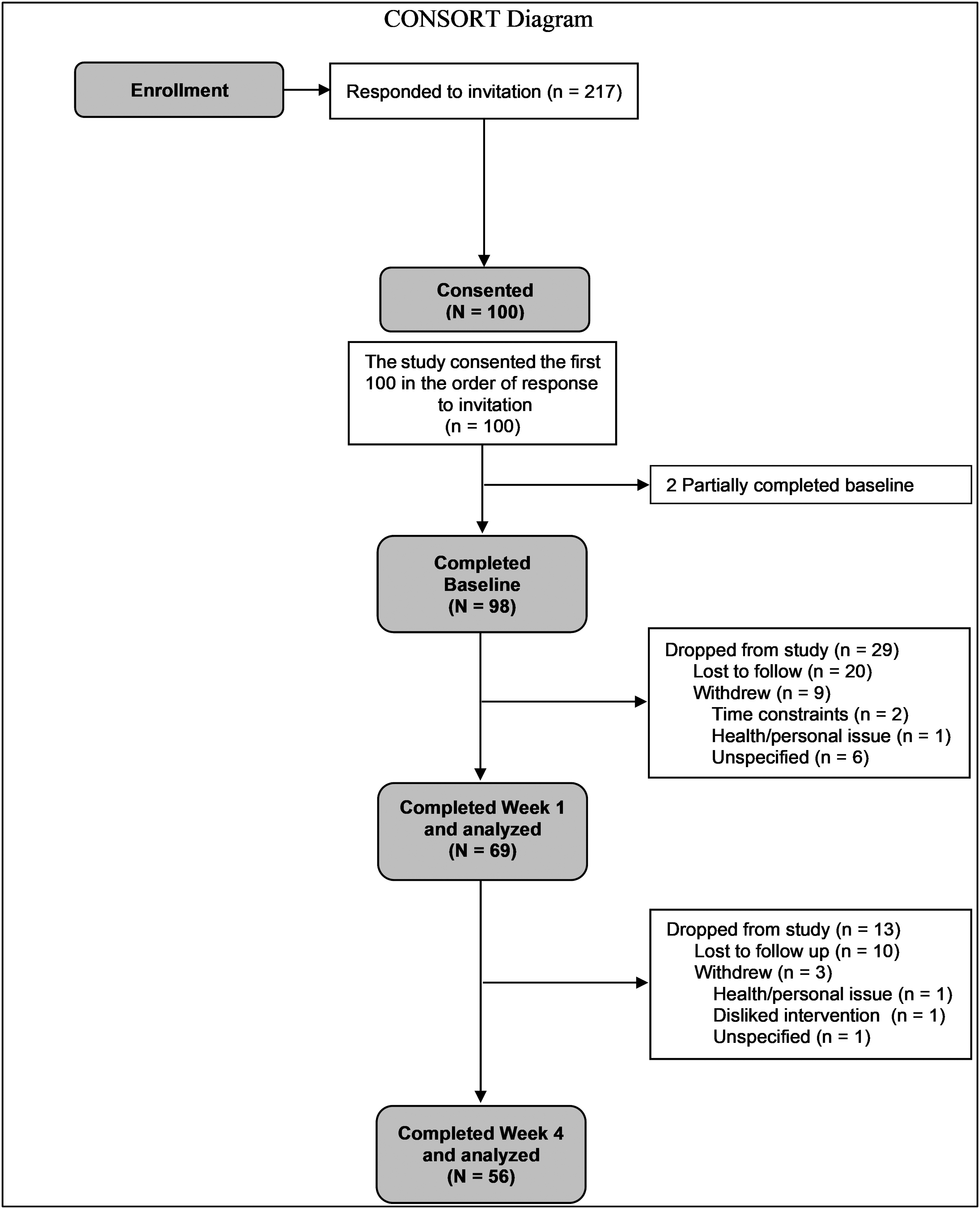
CONSORT diagram.
Adherence to the yoga breathing practice
During week 1, 48% of the participants indicated they practiced the breathing exercises two or more days per week, 5% practiced three or more days per week, 14% did not practice, and 33% did not report their practice. During those practice days, 70% indicated they practiced three or more times a day. The mean total breathing sessions in week 1 was 6 sessions, with a range of 0 to 15 sessions. During week 4, 48% practiced the breathing exercises on two or more different days during this final week of data collection, with 2% practicing 4 days per week, 16% not practicing at all, and 33% did not report their practice. Fifty percent indicated they practiced three or more times a day on the days breathing exercises were performed. Participants practiced a mean total of six breathing exercises during week 4, with a range of 0–14 practice sessions. Paired sample t-tests comparing weekly practice frequency and daily practice did not reveal any statistically significant differences between weeks 1 and 4.
Outcomes from the yoga breathing practice on HCWs during COVID-19
Mixed-effects ANOVAs comparing baseline to 4-week scores revealed significant decreases in the COVID-19 Distress score (p < 0.0001) and COVID-19 Disruption (p = 0.013), with significant increases in COVID-19 Stress Management (p = 0.0001) (Table 1). Furthermore, there was also a significant increase in the BRCS scores (p = 0.012). There were, however, no significant differences between pre- and postintervention for the COVID-19 Financial Hardship, COVID-19 Benefits measure, and the PSS, or for breath holding time.
Baseline and 4-Week Postintervention and Mixed Models Outcomes
Some scales had missing values with sample size at baseline ranging from 97–100 to 50–56 for the 4-week follow-up.
COVID-19 item scores range from 0 to 4 and were averaged together for subscale scores.
SD, standard deviation.
mCONSORT 2010 Checklist of Information to Include When Reporting a Randomized Trial
© 2010 Schulz et al. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. 22
We strongly recommend reading this statement in conjunction with the CONSORT 2010 Explanation and Elaboration for important clarifications on all the items. If relevant, we also recommend reading CONSORT extensions for cluster randomized trials, noninferiority and equivalence trials, nonpharmacological treatments, herbal interventions, and pragmatic trials. Additional extensions are forthcoming: for those and for up-to-date references relevant to this checklist, see www.consort-statement.org
Individual items
To explore which specific questions were driving the changes from baseline to week 4 for the COVID-PPE Distress, Disruption, and Stress Management scales, as well as the BRCS scales, individual items were examined. Mixed-effect ANOVAs on the individual items of the COVID-PPE Distress scale revealed that participants had improvements on 9 of 11 items, including feeling significantly less anxious about getting COVID-19 after the intervention compared with before (mean change [MC] = −0.3, p = 0.001), less worried about infecting others (−0.6, p = <0.0001), less worried about a family member or close friend getting or dying from COVID-19 (MC = −0.3, p = 0.017), and less worried about themselves dying from COVID-19 (MC = −0.3, p = 0.002). Participants felt less out of control over how COVID-19 will impact their life (MC = −0.5; p = 0.006) and reported significantly less feelings of sadness or depression (MC = −0.4; p = 0.002), and social isolation (MC = −0.4; p = 0.008) after the intervention.
Participants reported significantly fewer changes in sleep (MC = −0.5; p = 0.0004) or eating (MC = −0.4; p = 0.016) after the intervention. There were no changes in negative feelings about the future, and difficulty concentrating.
Examination of the four individual items that make up the COVID-19 Disruption subscale, participants reported significant reduction in disruptions in day-to-day social interactions with family and/or friends (MC = −0.3; p = 0.042) and significantly fewer problems performing their daily routine (MC = −0.4; p = 0.019), with no differences for ability to adequately care for family and friends, and conflict with household members. Similarly, examining the five individual items in the Perceived Stress Management subscale revealed that participants reported significantly increased ability to practice relaxation techniques when feeling stressed about COVID-19 (MC = 0.7; p < 0.0001), as well as to re-examine negative thoughts and gain a new perspective when concerned about COVID-19 after the intervention (MC = 0.2; p = 0.027). Participants also reported increases in giving themselves the care and tenderness they need when going through a hard time (MC = 0.5; p < 0.0001). However, there were no differences for changes in recognizing stressful thoughts and situations, and seeking information and planning for concerns about the virus.
On the four BRCS questions, participants reported being significantly better at dealing with difficult situations (MC = 0.3; p = 0.01) and more able to look for ways to replace losses encountered in life (MC = 0.2; p = 0.049), with no differences in finding ways to change difficult situations, and ways to replace losses in life.
We also examined the outcomes by whether people worked mainly remote versus in person and clinical staff versus nonclinical staff. The effects of the intervention did not vary by either work category. Adherence to the intervention at week 4 was examined as a possible predictor of outcomes and there were no consistent associations between frequency of pranayama practice with outcomes.
Adverse events
There were zero serious adverse events or adverse events reported during the study. However, one participant withdrew from the study because they disliked the intervention (Fig. 1).
Discussion
Despite the increased interest, limited studies exist on helping HCWs improve coping strategies. 18 This secondary analysis of a yoga-based breathing intervention for HCWs found significant reductions in COVID-19-related distress and COVID-19 disruptions among HCWs during the COVID-19 pandemic. There were also significant increases in the ability to engage in stress management and participants reported improvements in resilience as measured by the (BRCS). However, we did not find any changes in perceived stress or breath holding time. Although the changes for some of the outcomes were small, it is notable that, at the individual question level, numerous questions related to COVID-19-specific distress and disruptions improved. This suggests pranayama practice is helpful during difficult times. Surprisingly, there was no association between frequency of practice with any of the outcomes. This may be due to most participants only practicing 2 days a week and the practice itself being brief. Future research should examine varying the frequency and length of exposure per week balanced against concerns in maintaining adherence.
These findings are consistent with a study conducted in health care professionals examining pranayama's effects on the mental health of frontline HCWs exposed to COVID-19. 19 In this trial, 123 HCWs were randomized to a control group and 127 HCWs to a pranayama intervention group. There was a significant reduction in perceived stress in the pranayama group compared with the control group and improved perceived quality of life, especially in psychological domains, yet no differences in wellbeing. 19 Another prior pranayama study administered bhastrika (a different yogic breathing practice) in healthy elderly subjects and compared them with a stretching control group. 20 The yoga breathing group showed significant increases in pulmonary function and a significant decrease in a marker of cardiac sympathetic modulation and sympathovagal balance of heart rate variability. Another study using Sudarshana kriya yogic breathing combined with specific movements, found that the practice lead to lower anxiety, depression, stress, and increased optimism. 21 These studies had a longer intervention duration, a more vigorous practice, instruction was conducted in-person, and adherence rates were high.
Although overall perceived stress did not change in this study, providing HCWs with effective strategies for managing the extra stress associated with the pandemic was valuable. The pranayama practice was delivered at the height of the pandemic, modifying overall perceived stress was not the main goal and would be difficult to change with this brief intervention. However, reducing the distress and disruption specific to COVID-19, providing extra coping skills and resilience was achieved.
There are several limitations to this study. The trial was single-arm, so it is not clear if these changes would have taken place due to the passage of time. However, even at the time the last participant provided their 4-week follow-up data in November 2020, there was still substantial uncertainty in the world and the stress and workload remained the same or higher than at baseline. Most participants (88%) were women, so the findings may not represent the larger population of HCWs. In addition, of the 217 participants who expressed interest, 100 consented, with only 56 providing data at week 4. The only difference noted between those who did and did not provide the follow-up data was remote versus in-person work. This may be due to the greater work flexibility inherent to remote work versus in person. Loss to follow-up was common in other yoga/meditation studies in HCWs. 19 Providing more opportunities to engage with the program may have improved adherence, however, we did not measure barriers to adherence. While the self-paced, self-guided study design was useful for quick dissemination, participants may have benefited from a live video-based class with an instructor.
They may have also benefited more from a longer program. This practice lasted 5 min, including the 2-min meditation. Although the shortness of the program may decrease efficacy, this needs to be balanced against the burden of a longer practice, and the substantial workplace demands expected of HCWs, where adherence may be lower. This was also a self-selected group of participants, so their interests could have aided participation in the intervention and potentially accentuating the outcomes of participants who completed the study. Numerous statistical analyses were conducted without adjustment for multiple comparisons. Yet, we acknowledge that these were secondary analyses, and the main aim of the trial was feasibility of delivery and adherence during a pandemic. 11 Due to a lack of funding, we could not carry out more objective lung capacity measures, such as spirometry. The breath holding time outcome is not a sensitive measure of lung function and is subject to self-reporting biases.
Despite these limitations, the study has several strengths. The study was designed, launched, and conducted during a global pandemic to address stress among HCWs. The study was conducted at a large comprehensive cancer center and was delivered online, giving flexibility for participants. The online data collection minimized both participant and researcher time collecting data over the phone. The online support through zoom calls was convenient and adherence friendly for study participants. The pranayama practice was brief, which HCWs can use any time, even during a short break in the workplace.
Conclusions
Overall, the study found that a brief pranayama practice provided online can reduce pandemic-specific stress, disruptions, and lead to improvements in both resilience and stress management skills among HCWs. A 5-min Simha Kriya yoga breathing and meditation practice is quickly learned and applied. Cost-effective and fast relaxation practices can aid HCWs to relieve psychosocial stress and burnout, suggesting a need for further large-scale trials.
Footnotes
Acknowledgments
The authors thank the MD Anderson staff for participating in the study and the Palliative, Rehabilitation, and Integrative Medicine department for their support and advice. The authors would also like to thank Jewel Ochoa for her support with study design and data collection.
Ethics Approval
The study was approved by The University of Texas MD Anderson Cancer Center Institutional Review Board (2020-0483). Participants provided written informed consent electronically through the REDCap data base before participating in the study.
Authors' Contributions
R.W.W. contributed to the analysis, interpretation of data for the work, draft/edit the article, preparing the article for publication, and final approval of the version to be published. S.M. contributed to the conception or design, draft/edit the article, preparing the article for publication, and final approval of the version to be published. R.E. contributed to study coordination and preparing the article for publication. V.V. contributed to draft/edit the article. E.B. contributed to the conception or design, and final approval of the version to be published. B.S. contributed to the conception or design, edit the article, and final approval of the version to be published. L.C. contributed to the conception or design, analysis, interpretation of data for the work, draft/edit the article, and final approval of the version to be published. S.N. contributed to the conception or design, study coordination, analysis, interpretation of data for the work, draft/edit the article, and final approval of the version to be published.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Partial funding was provided by the Duncan Family Institute for Cancer Prevention and Research and by the Richard E. Haynes Distinguished Professorship for Clinical Cancer Prevention (Lorenzo Cohen), The University of Texas MD Anderson Cancer Center.