
Abstract
Introduction:
The study aimed to pilot test a well-being curriculum for KL2 scholars to be used across the Clinical and Translational Science Award consortium.
Methods:
Between November 2022, and May 2023, 36 KL2 scholars from 25 hubs participated in the program. The General Well-Being Index for U.S. Workers and the Patient Reported Outcomes Measurement Information System (PROMIS-29) were completed by scholars before and after the program.
Results:
Postparticipation, there was a trend of improvement in the domains of well-being, sleep, anxiety, and fatigue.
Conclusion:
Implementing a virtual synchronous well-being curriculum allowed the scholars to connect across the consortium and improve their well-being.
Introduction
The unprecedented circumstances of the COVID-19 pandemic thrust the concept of the well-being of scientists and trainees to the forefront of discussions on the clinical and translational science workforce. Although mounting literature has documented the role of occupational stress in science career choice, research productivity, and retention, 1,2 the immediate effects of the pandemic on the well-being of trainees and early career faculty motivated training program directors to determine how well-being topics should be incorporated into training. 3
A working group focused on well-being was formed within the NIH-funded Clinical and Translational Science Award (CTSA) consortium to address this question. A goal of the working group was to develop and pilot test a virtual synchronous curriculum for CTSA-funded junior faculty of the career development KL2 program to provide strategies to support well-being and resilience and to offer implementation strategies for future training curricula.
Well-being is a multifaceted construct encompassing health and happiness, what people think and feel about their lives, and their overall satisfaction with life, such as the quality of their relationships, their positive emotions and resilience, the realization of their potential, and feelings of joy. 4 Poor sleep/insomnia and anxiety have negative impacts on health and well-being and are associated with lower happiness. 4,5
Mindfulness training has been shown to improve mental distress and subjective well-being in medical and psychology students, 6 however, there are no dedicated programs for early career researchers. The Stress Management and Relaxation Training—Relaxation Response Resiliency Program (SMART-3RP) is an evidence-based resiliency program designed to promote adaptation to stress and enhance individual resiliency. 7 This program has been administered virtually to frontline health care workers and reduced COVID-19-associated distress and improved resiliency. 8
Here an adaptation of the SMART-3RP administered to KL2 scholars across the CTSA consortium and the initial results of this pilot program are described. The authors hypothesized that it would be feasible to implement the program and that participants would be able to improve their overall stress reactivity, sleep, anxiety, and fatigue and engage in positive lifestyle behaviors. The authors also hypothesized that the curriculum would provide peer support to address shared challenges.
Materials and Methods
The well-being integration working group was tasked to design and pilot a virtual synchronous well-being curriculum for KL2 scholars across the CTSA consortium. The curriculum was based on the SMART-3RP 7 and was adapted for KL2 scholars with a focus on health and research uncertainty, job transitions, isolation, and financial and family challenges. Eight weekly sessions were held for 90 min each and included ∼45 min of unstructured time to allow scholars to interact and build a peer network. The program was grounded in relaxation response elicitation, mindfulness, cognitive behavioral therapy, and positive psychology. Details on the individual sessions are summarized in Figure 1. The curriculum was administered by two trained facilitators.
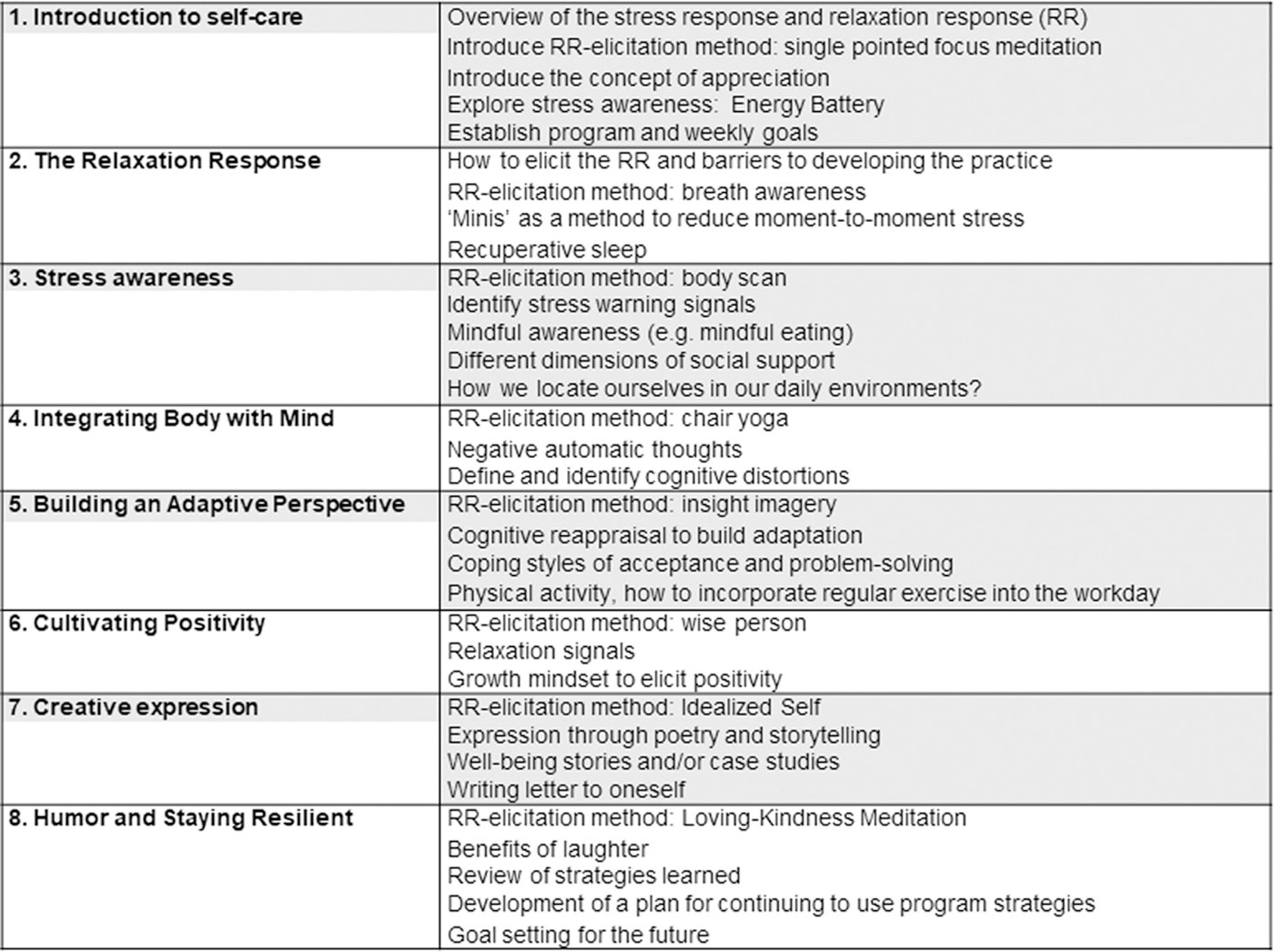
Curriculum overview.
In August 2022, an e-mail was forwarded to KL2 program directors asking them to survey their KL2 scholars to gauge their interest in participating in the curriculum. Interested scholars were assigned to one of two cohorts based on their schedule availability. The two cohorts occurred virtually and synchronously at a mutually agreed-on time conducive to participation across the continental United States (and Puerto Rico). Cohort 1 ran from October to December 2022, 1 pm Eastern Daylight Time (EDT)/10 am Pacific Daylight Time (PDT), and cohort 2 ran from March to May 2023, 5 pm EDT/2 pm PDT.
Program evaluation
Online pre- and postsurveys (REDCap) were pretested for content and online functionality by the working group members. Both pre- and postsurveys included the general well-being index (WBI) for U.S. workers 9 and the Patient Reported Outcomes Measurement Information System (PROMIS-29). 10,11
Data analysis
Ratings for specific items were converted, and quantitative outcome measures were scored. Data from the first and second cohorts were combined. Descriptive statistics (frequency; mean ± SD) were calculated for participant demographics and pre- and post-WBI and PROMIS-29 health domain scores. To interpret health-related quality of life on the PROMIS-29, scores were compared with the norms available from the general population 12 and interpreted as within normal limits or reflecting a mild, moderate, or severe decrease or increase.
Due to the small sample, nonparametric statistics were used to compare pre- and post- within-group differences; specifically, separate Wilcoxon-signed rank tests were used, with significance set at p < 0.05. Quantitative statistical analyses were performed using SPSS (v.29, IBM, Armonk, NY).
IRB approval
The project was reviewed and determined to not meet the criteria for human subject research as defined by Mass General Brigham Institutional Review Board (IRB) policies and Health and Human Services regulations set forth in 45 CFR 46
Results
Forty-one KL2 scholars expressed interest in participating in the curriculum, and 36 scholars from 25 hubs were able to participate: 15 in the first cohort and 21 in the second cohort. Five participants were not able to participate due to time constraints from competing personal or professional demands. Participant demographics are summarized in Table 1.
Participant Demographics (n, %)
DVM, doctor of veterinary medicine; MD, medical doctor; PhD, doctor of philosophy.
Impact of the program
Of the KL2 scholars who completed the curriculum, 36 (100%) completed the baseline survey and 11 (31%) finished the postsurvey.
For the WBI, there was a trend toward improvement in well-being after completion of the curriculum (Table 2). For pre-WBI scores, 17% of participants had scores of ≤1 point (low risk), 33% had scores between 2 and 4 points (medium risk), and 50% scored ≥5 points (high risk). For post-WBI scores, 18% of participants had ≤1 point, 64% had scores between 2 and 4 points, and 18% scored ≥5 points.
Pre- and Postintervention Scores on the Well-Being Index and the Patient Reported Outcomes Measurement Information System 29-Item Profile
p ≤ 0.05.
n/a, not applicable; PROMIS, Patient Reported Outcomes Measurement Information System; SD, standard deviation; WNL, within normal limits.
Although there were no statistically significant differences across the health domains in the pre-PROMIS-29 weighted scores and post-PROMIS-29 weighted scores (p ≥ 0.079), the group mean and median for sleep disturbance improved, and anxiety and fatigue improved compared with the general population 12 (Table 2).
Qualitative feedback
Four participants (11%) provided qualitative feedback about their overall experience that was positive. One participant noted, “I enjoyed being made more aware of practices to induce mindfulness and to take the time to cultivate that in myself. I am continuing to practice these exercises and give myself grace and permission to take time for myself and not to have to do everything all at once.” Another participant described the benefit of the support they felt from others with similar shared experiences, “Great interface to connect with people in similar positions from all over the nation to discuss the reality of our work-related stressors. It helps to realize that we are not alone and we share much of the same concerns. While only an 8-week program, the weekly face time helped create a sense of community and comfort. THANK YOU!”
Discussion
This study aimed to implement and pilot test a virtual synchronous well-being curriculum for KL2 scholars, the first across the CTSA consortium. The results demonstrate interest among KL2 scholars in well-being support, and the feasibility of implementing the virtual synchronous curriculum at a national level. The results also showed that scholars derived benefits from participation in the program. Well-being, sleep, anxiety, and fatigue seemed to be more positively impacted. The number of participants with a high risk of poor quality of life on the WBI decreased from 50% to 18%.
Sleep increased and anxiety and fatigue decreased on the PROMIS-29 demonstrating a plausible benefit of the curriculum. Qualitative feedback indicated that participants found the curriculum to be worthwhile. They enjoyed connecting with others in similar roles, creating a sense of community, and discussing stressors and concerns. These findings from the pilot program support its feasibility and acceptability and the basis for future studies.
For each cohort, the program was initiated after what for most is considered the “summer break” (early fall) and “winter break” (beginning of the calendar year). The KL2 scholars were simultaneously instructing medical students, residents, fellows, and other trainees, managing their research and laboratories, and performing clinical work. It is plausible that as the weeks progressed, the stressors of instruction, grading, mentoring, research oversight, and conducting their research and their clinical work were increasing. Therefore, improvement or no change in some of the outcomes might reflect a positive impact of the program by providing the scholars with tools and strategies to manage better or dampen stressors that would have previously impacted their well-being.
The qualitative results of this study are consistent with other literature describing a benefit to early career researchers from peer networks that provide support through discussion of shared experiences and challenges. 13,14 Specifically, the scholars were able to have dedicated and intentional time to interact with one another from across the country; at the same time, the curriculum provided a structured venue for the scholars to discuss issues that were common and meaningful between them.
Notably, a new message is emerging within the literature that early stage investigators urge organizational leadership and mentors to prioritize well-being and support participation in well-being activities within the workday rather than infringing upon time after work. 15 Among the scholars who expressed interest, five could not participate due to competing personal and professional demands. Otherwise, well-being programs become less accessible to individuals with extraprofessional responsibilities.
Limitations
This study had the following limitations. First, the small sample size and the low postsurvey response rate, which limited the ability to demonstrate statistical significance in the analysis. However, as this was a pilot study, the authors focused on feasibility of administering a well-being curriculum virtually across the CTSA consortium. Another limitation is the lack of randomization and a control group. Inclusion criteria on baseline measures showing poor well-being or health-related quality of life were not defined; thus, the impact of the intervention likely rendered a ceiling or floor effect.
Unfortunately, presurvey levels could not be controlled because the small sample size required nonparametric statistics for the analysis. The authors recognize that organizational-level factors are a vital component of overall occupational well-being, and this study only intervened on individual-level factors, possibly limiting the overall impact.
Conclusion
The feasibility of adapting and piloting an eight-session synchronous well-being curriculum across the CTSA consortium from which participants benefited was demonstrated. The next step will be to further evaluate whether the program is scalable for implementation among a larger cohort of scientists and physician scholars and to perform a randomized study with a control group.
Footnotes
Acknowledgments
The authors thank Olga Brazhnik, PhD, for her dedication to elevating the discussion of well-being in the clinical and translational workforce, and the KL2 scholar participants for their active participation in the curriculum, and Rebecca Laird for assistance with data management.
Disclaimer
This study is solely the authors' responsibility and does not necessarily represent the official views of the NIH, NCATS, or CLIC.
Authors' Contributions
Conceptualization of the study was carried out by M.A.B., D.H.M., L.M.D., and S.N.P. Methodology was done by G.R., L.M.D., J.A., A.E.S., S.M., D.H.M., and M.A.B. Formal analysis was carried out by G.R. Investigation was done by L.M.D., D.H.M., J.A., A.E.S., S.M., G.R., S.N.P., and M.A.B. Writing—original draft was taken care by G.R., L.M.D., S.N.P., D.H.M., and M.A.B. Writing—review and editing was by G.R., L.M.D., J.A., A.E.S., S.M., S.N.P., D.H.M., and M.A.B. Supervision was carried out by D.H.M. and M.A.B.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded in part by the University of Rochester Center for Leading Innovation and Collaboration (CLIC) and the CTSA coordinating center funded by NCATS (U24TR002260); KL2TR002542, K24DK109940 (Bredella); UL1TR004406 (Pusek); R34DA057150; P30AI073961; R25DA028567 (Duthely).