
Abstract
Introduction:
This study aimed to understand health care providers’ experiences implementing the Oregon Back Pain Policy (OBPP) over time. The Medicaid OBPP expanded coverage of evidence-based nonpharmacological therapy (NPT) for back pain and restricted access to opioid therapy and interventional approaches.
Methods:
The study included six online, asynchronous focus groups with providers in February 2020 (Time 1) and August 2022 (Time 2). Analysis was conducted with a longitudinal, recurrent cross-sectional approach. Analysis occurred in three stages: (1) An immersion/crystallization approach was used to analyze Time 1 focus group data, (2) reflexive thematic analysis was used to analyze Time 2 data, and (3) longitudinal analysis was used to integrate the findings across time points.
Results:
At Time 1, 48 clinicians and 44 NPT providers participated in the study. Time 2 included 63 clinicians and 59 NPT providers. The longitudinal analysis of the focus group data resulted in four themes: (1) general awareness of the policy, (2) providers support the policy and perceive a benefit to their patients, (3) barriers to NPT accessibility, and (4) barriers to referring patients to NPT.
Conclusion:
The goal of the OBPP was to improve back pain care for Oregon Medicaid members by increasing access to evidence-based NPT and decreasing reliance on opioid medications. This study revealed that, although clinicians and NPT providers supported the policy, they faced persistent implementation challenges related to referrals, prior authorizations, coverage limitations, low reimbursement rates, and a reduced workforce for NPT providers. In some cases, implementation barriers were removed during the COVID-19 pandemic, but other challenges were more prominent during the pandemic.
Introduction
In 2016, Oregon implemented a novel policy to improve evidence-based back pain care and promote safer and more effective opioid prescribing through the state’s Medicaid program, the Oregon Health Plan (OHP). OHP is implemented through Coordinated Care Organizations (CCOs), locally governed Medicaid managed care organizations. The policy, which we will refer to as the Oregon Back Pain Policy (OBPP), expanded coverage of evidence-based nonpharmacological pain treatment modalities (NPTs), including physical/occupational therapy, acupuncture, yoga, chiropractic manipulation, massage, interdisciplinary rehabilitation, supervised exercise, and cognitive behavioral therapy, 1 while placing restrictions on acute and chronic opioid therapies for OHP recipients with back pain, emphasizing nonopioid medications as first-line, and discouraging unnecessary back surgeries and procedures. While the OBPP is a state-wide effort to improve back pain care, policy implementation was not standardized and CCOs tailored benefits to their members. CCOs varied in their standard visit limits for NPT coverage, the NPT services that would be made available, prior authorization criteria, and referral requirements. Furthermore, referring clinicians have flexibility to decide when to refer a patient to NPT, as well as which NPT service is most appropriate for a given patient.
Evidence suggests that the OBPP has been effective in increasing NPT use 2 and reducing opioid prescriptions among OHP recipients. 3,4 While these early findings are promising, providers in Oregon describe logistical and epistemological challenges implementing the policy. 5 –7
This study builds upon our findings from a cross-sectional survey study 8 fielded in 2019 and two qualitative studies 6,7 that were conducted in early 2020 to explore how OHP providers experienced the OBPP over time. Since our initial published findings, the COVID-19 pandemic occurred, and it is impossible to ignore the seismic shifts in care precipitated by this event. Research suggests that prescription opioid analgesics replaced NPT treatment for commercially insured acute and chronic pain patients 3 in the United States 9 during the pandemic, and that non-COVID-19-related health care treatment services dropped precipitously, 10 raising questions as to how the OBPP was impacted during this time. Thus, our study additionally sought to understand the experiences of Oregon providers implementing the OBPP during and post-COVID-19 pandemic (Time 2; T2), in relation to experiences before the pandemic (Time 1; T1) (see timeline in Fig. 1).
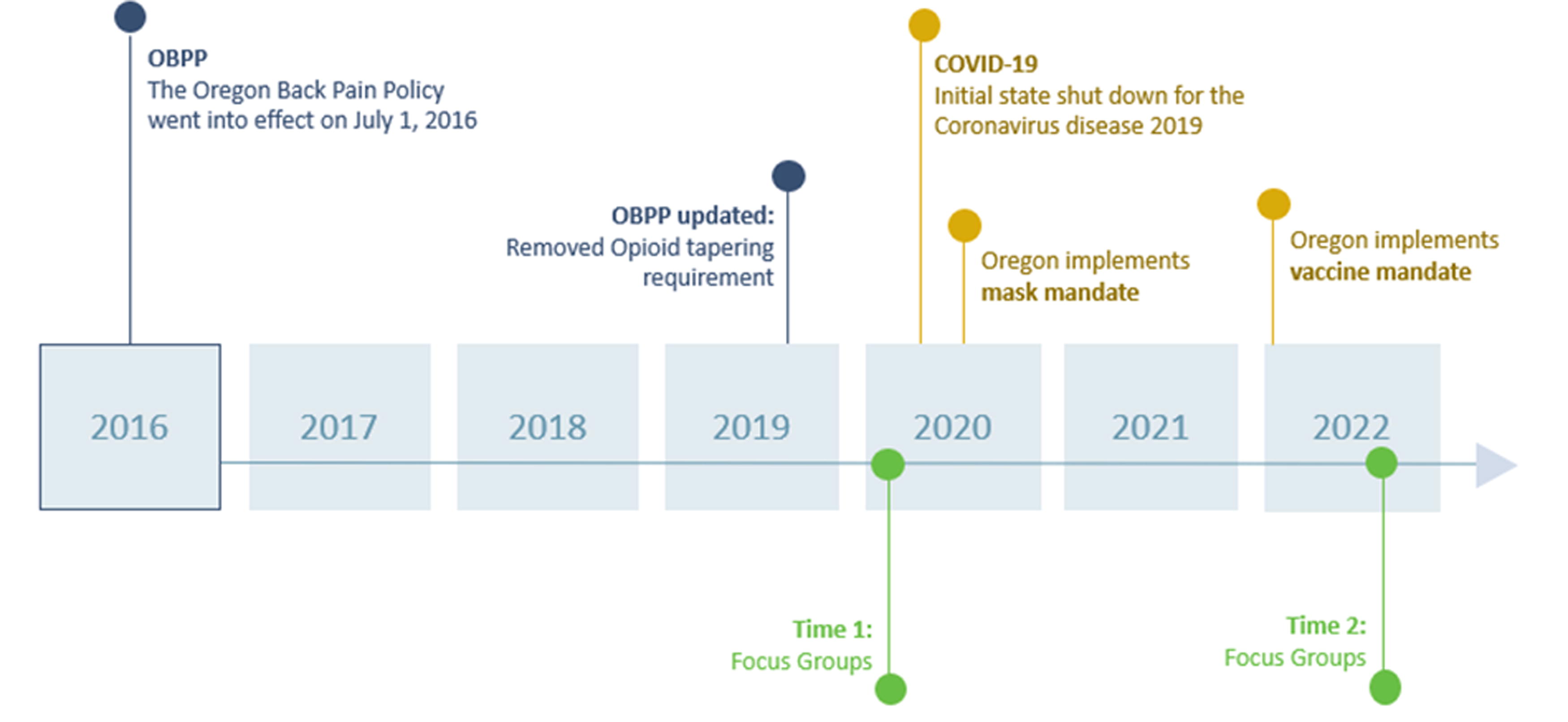
Longitudinal study design.
Materials and Methods
Methods for T1 have been previously described. 6 –8 We conducted six asynchronous online focus groups (AOFGs) consisting of two sections (see Table 1) for T2. For each section, we developed parallel but distinct focus group guides appropriate for the groups’ members, structured around T1 focus group guide sections, with the addition of topics related to challenges to and facilitators of back pain over time and during the COVID-19 pandemic. The study was approved by the OHSU Institutional Review Board (IRB#18725).
Focus Group Sections at Time 2
In Oregon, naturopathic doctors are primary care providers by statute and have a broad scope of practice, including prescribing controlled substances.
Participants and procedures
In our quantitative work, 2 we found it was difficult to capture the use of some therapies covered under the policy (e.g., yoga, CBT) because the related codes in claims data are nonspecific and/or not consistently co-coded with a back pain diagnosis. For alignment, we focused our qualitative work on the four services that were consistently identifiable for Medicaid recipients with back pain: acupuncture, chiropractic treatments, massage, and physical therapy. Recruitment and participant selection strategies were parallel to those used for the T1 study. 6,7 Participants were recruited by email through contact lists from state accreditation boards for the relevant professions for five of the focus groups. We used a random number generator to select participant emails for recruitment. Since doctor of chiropractic (DC) board lists were unavailable, we recruited DCs by invitation through a monthly newsletter from their local professional association. An initial email and follow-ups were sent to providers between August and September 2022. The email described the purpose of the study and included an invitation to complete an eligibility screener survey online using REDCap. 11 To be eligible, NPT providers had to be (1) independently credentialed to provide care to OHP patients or be affiliated with an OHP credentialed provider and (2) have provided treatment to OHP patients with back pain since COVID began in March 2020. Prescribing clinicians had to have provided treatment to OHP patients with back pain since COVID began in March 2020.
At T2, 4,650 NPT providers (excluding DCs) and 4,378 prescribing clinicians were invited to participate in the study, and 211 NPT providers and 208 clinicians completed the eligibility screener. Of those, a respective 57% (n = 120) and 80% (n = 167) were eligible and invited to participate in a focus group and 49% NPT providers (n = 59) and 38% prescribing clinicians (n = 62) went on to participate in the focus groups. Participants received a $75 e-gift card for participation.
Data collection
The eligibility screener survey at T2 included items to assess eligibility and demographic characteristics. The AOFGs were conducted online using QualBoard, a platform that allows individuals to sign in during a participation window and join the discussion using an assigned pseudonym. AOFGs were chosen to allow participants to both respond to questions and explore, reflect, and build on each other’s experiences in the back pain practice environment, enabling the research team to access a wide variety of responses more efficiently than through interviews. 12 We opted to use AOFGs, as the anonymity allows data collection around sensitive topics 13 and the ability to engage when convenient 14 is an appealing advantage for data collection from health care professionals with demanding schedules. 15
Each AOFG included 12–20 participants. This group size was selected based on previous team’s experience conducting AOFGs, 16 in which we found the online format allowed dynamic engagement within this range. Two trained qualitative researchers with experience conducting focus groups with health care providers (K.L. and M.G.) co-moderated the groups, and the principal investigator (E.C.) and co-investigator (C.L.) observed the groups. Transcripts were uploaded into NVivo (version 12) for data analysis.
Analysis
Descriptive analyses were performed on the eligibility screener, and demographic characteristics of the focus group participants are described below. Qualitative data analysis was conducted with a longitudinal recurrent cross-sectional approach 17 to highlight policy changes from the initial to maintenance phase of policy implementation. Analysis occurred in three stages: (1) An immersion/crystallization approach 18 was used to analyze T1 focus group data, (2) reflexive thematic analysis (RTA) 19,20 was used to analyze T2 data, and (3) longitudinal analysis was used to integrate and compare the findings from both time points. A full description of the analytic approach used for T1 is reported elsewhere. 6,7 The RTA for T2 included five phases: (1) data familiarization, (2) generating initial codes, (3) generating themes, (4) reviewing themes, and (5) defining and naming themes, which are described in detail below. Finally, we created sequential matrices (tables) to facilitate a longitudinal analysis to compare the thematic data between T1 and T2 focus groups cross-sectionally.
For the T2 RTA, all transcripts were read by the research coders (D.F., K.L., and M.G.), who drafted memos, entered margin notes, and discussed data insights with the team. Team members (A.C., D.F., and M.G.) added codes, revised definitions, and discarded codes during weekly meetings. Next, coders (A.C., D.F., K.L., and M.G.) applied codes to all data. Coded data were then used to construct themes, or units of meaning across data. We built themes by grouping codes that formed meaningful patterns. 20 Themes were discussed in bimonthly qualitative team meetings by the entire team and included discussions of the researchers’ positionality to the data to bring awareness to and limit sources of bias. Themes were then fine-tuned and named. Finally, results were written into article form and edited over a series of monthly meetings by all co-authors.
Finally, we conducted the longitudinal analysis by mapping the themes identified in both T1 and T2 analyses into categories based on apparent similarity. These groupings were summarized with a central theme that captured the longitudinal nature of separate themes.
Results
Demographic characteristics of the 122 participants at T2, relative to T1, are presented in Table 2. The RTA findings from T2 resulted in four themes: (1) general awareness of the policy, (2) continued support of the policy and perceived effectiveness of NPT for back pain, (3) barriers to NPT accessibility, and (4) barriers to referring patients to NPT (Table 3). In the section to follow, we present the results from T2 and contextualize the findings relative to T1. Findings from the longitudinal analysis are summarized in Table 4.
Participant Characteristics
Some providers were dual credentialed.
Emergent Themes, Subthemes, and Supporting Quotes at Time 2
NPT, nonpharmacological therapy; OBPP, Oregon Back Pain Policy; CCO, Coordinated Care Organizations; OHP, Oregon Health Plan.
Longitudinal Analytic Findings: Themes at Time 1 and Time 2
NPT, nonpharmacological therapy; OBPP, Oregon Back Pain Policy.
Theme 1: General awareness of the OBPP
Most participants (79%) said they were “fairly familiar,” or “familiar” and “very familiar” with the policy (Fig. 2), a greater proportion than reported at T1.8

Level of familiarity with the OBPP at Time 2. OBPP, Oregon Back Pain Policy.
Consistent with T1, we observed ongoing knowledge gaps related to policy elements outside the providers’ specialty area at T2. For example, several clinicians shared that while they were aware of the policy’s restrictions around opioid prescribing, they were unaware of the specific NPT covered by the OBPP. Participant 86 (MD) shared, “The coverage of the policy and in particular the services that are part of coverage were new to me.” Likewise, while NPT providers were mostly aware of the policy’s expanded coverage of NPT, they lacked clarity on the specifics related to opioid prescribing restrictions. For example, Participant 12 (ACU) said, “I was not familiar with the doctors’ guidelines how to reduce opioids.”
Theme 2: Providers support the policy and perceive a benefit to their patients
Consistent with findings from T1,6,8 NPT providers at T2 reiterated that the policy’s expanded access to NPTs was good for their patients. Providers described how expanded NPT coverage has improved their ability to care for their patients and that the policy had improved patient’s quality of life. For example, Participant 73 (MD) shared, “When patients have been able to establish and receive [NPT] care, they are very happy with it and it has been helpful.”
Congruent with T1,7 clinicians at T2 said that most of their patients were receptive to trying NPT. Still, a few clinicians described a small subset of patients who are reluctant to try NPT, and these clinicians described how they used OBPP as a backbone to facilitate conversations with their patients. For example, Participant 64 (DO) shared:
“[The OBPP is] very useful actually… . When patients push for more/outside of standard of care, I try to talk to them about evidence-based care and if they still push—I can fall back on the hard policies here so they don't get upset with me.”
Theme 3: Barriers to NPT accessibility
NPT providers described several ongoing barriers to providing care, including delays associated with prior authorization (PA) and referrals, congruent with T16. For example, Participant 90 (ND) shared, “The referral process takes a long time so patients often have to wait weeks before they can receive treatment.” However, unlike T1, T2 providers described how one CCO in Oregon lifted the PA and referral requirements for initiating NPT care under this policy during the COVID-19 pandemic. Providers impacted by lifting the PA requirement expressed unanimous support and enthusiasm, describing how it allowed them to focus more on treating patients. For example, Participant 14 (ACU) shared, “Without prior auth which greatly reduced the paperwork and acupuncturist could more focus on the treatment.”
NPT providers at T2 describe how visit restrictions in coverage hampered the effectiveness of their practice, a sentiment that is consistent with T1. For example, Participant 96 (ND and ACU) said, “… for patients who utilize multiple ‘alternative’ modalities, 30 visits combined total for Acu, PT and chiropractic for a year does not get them very far if the condition is chronic.” Others described frustrations with getting coverage for NPT visits at all. For example, Participant 27 (LMT) shared, “Many [of my patients] only receive 6 visits which isn’t enough to help with pain management.”
NPT providers also described challenges related to low reimbursement rates at T2, consistent with findings from T1.6 In addition, T2 participants described how challenges related to low reimbursement rates were exacerbated by the pandemic. For example, many NPT providers had to reduce the volume of patients they saw in a day to accommodate COVID-19 cleaning protocols that required spacing out the timing of patient appointments. In addition, some acupuncturists who previously saw several patients at one time in a group setting were required to move to treat one patient at a time during the pandemic. As such, providers were billing for a lower volume of patients and expressed frustration that reimbursement rates, already low, were not increased, which would have offset the reduced volume.
Theme 4: Barriers to referring patients to NPT
At both time points, clinicians expressed varying levels of perceived effectiveness of NPT across modalities. At T2, like T1,8 clinicians widely agreed on the effectiveness of physical therapy. For example, Participant 115 (NP) shared the belief that, “PT has the greatest amount of evidence-based studies showing short and long-term benefit. This should be a first choice when available,” and Participant 81 (MD) said, “I use evidence-based medicine. PT is supported by good evidence.” In contrast, some clinicians expressed skepticism about chiropractic treatment at T2, a sentiment also shared at T1.7 For example, Participant 115 (NP) stated, “I would recommend against chiropractic referrals regardless as there is no evidence-based studies showing actual benefits.”
Clinicians continued to face logistical challenges related to referring patients to NPT due to limited Medicaid credentialed NPT providers in Oregon, a finding consistent over time. 7 For example, Participant 12 (ACU) said, “I’d say credentialing the practitioners is the biggest barrier- more credentialed providers-we can see more OHP clients.” The lack of NPT providers and associated challenges with referring patients were exacerbated during the COVID-19 pandemic. For example, Participant 129 (PA) described, “I have run into several brick walls getting patients to find providers who will take their OHP and also have bandwidth in their schedules since covid.”
Discussion
Despite the early successes of the OBPP, challenges remain. The OBPP was first implemented in 2016 alongside other opioid restriction policies and practice guidelines in the state and nationwide. 3,4 It was a one-of-a-kind Medicaid policy that included the novel expansion of coverage to NPT for back pain. Successful implementation of the OBPP includes a prescribing clinician referring to NPT and patient accessing the services, in conjunction with decreased use of opioids for back pain. While early evidence suggests the policy was successfully implemented to some degree—opioid prescriptions decreased, 3,4 while NPT increased post policy 2 —there is notable room for improvement. For example, although NPT use increased post policy, our previous studies have demonstrated racial and rural disparities in NPT uptake 2 and a lack of awareness of the policy and implementation challenges that impede successful referrals. 6,7 This study used a recurrent, cross-sectional approach to explore providers’ experiences implementing the OBPP over time, illuminating ongoing challenges in implementing the policy, as well as facilitators of implementation.
This study identified continuing implementation challenges of the OBPP six years into policy implementation. Continuing challenges include the high administrative burden for NPT providers that limits treatment effectiveness (e.g., delays in access due to prior authorization, annual visit limit restrictions) and Medicaid reimbursement rates that are too low to sustain a financially sustainable practice, a concern shared among health care professionals nationally. 21,22 Clinicians in our study found it difficult to locate OHP-credentialed NPT providers in Oregon, a trend seen at the national level where there is a decline in Medicaid credentialed health care providers. 23 In Oregon, this means that providers cannot refer patients for back pain treatment, and thus, the policy cannot be implemented in full. Providers described how these preexisting issues were exacerbated during the pandemic due to COVID-19 policies that limited the number of patients NPT providers could treat daily.
Overall, clinicians in our study expressed a high degree of enthusiasm for NPT, a finding that mirrors existing evidence, 24 –27 but their perspectives of effectiveness of NPT varied by modality. Clinicians in our study tended to favor physical therapy over chiropractic care, even though both have demonstrated moderate levels of effectiveness for back pain. 1,28 These beliefs, not rooted in evidence, may be barriers to the implementation and subsequent impact of policies like OBPP. These findings suggest that continuing education programs and policy awareness campaigns targeting providers should disseminate evidence of effective care for back pain to allow for the policy to be implemented more uniformly across NPT modalities.
While our study identified barriers to OBPP implementation that persisted over time and during the COVID-19 pandemic, facilitators were also illuminated. Our findings suggest that clinician perspectives and practices are more aligned with the policy at T2 than T1. Specifically, clinicians were more likely to be familiar with the OBPP overall, aware of at least some NPT coverage, and more confident in the evidence of NPT in treating back pain. Clinicians described how they use the NPT evidence base, especially PT, and the policy’s guidelines to facilitate conversations with patients. This finding is consistent with earlier work showing that clinicians appreciate standardized opioid prescribing guidelines to support decision-making in clinical encounters. 29 This is especially important with regard to conversations around opioids and tapering, which have been proven to be challenging for patients and clinicians. 30 –33 An additional policy facilitator was revealed during the COVID-19 pandemic when one CCO temporarily lifted the PA requirement. NPT providers were enthusiastic about this change and described how it relieved them of an administrative burden—one described by providers at both time points—and created more time for them to focus on treating OHP back pain patients.
Limitations
Those who volunteered to participate in a study of the OBPP may be biased toward those who tend to feel strongly about the OBPP or back pain treatment, rather than those with diverse perspectives of the policy, which may skew results to the more extreme positive or negative viewpoints. Although the demographic panel of these study participants is racially homogenous, they represent providers in Oregon 34 and nationally. 35 Notably, due to variations in the NPT services covered by the OBPP by CCO and insufficient numbers of local NPT credentialed providers, not all NPT services (e.g., yoga) were discussed by participants. Our findings are limited to the more frequently utilized services that were discussed at length, including acupuncture, chiropractic manipulation, and physical therapy. Finally, while our longitudinal recurrent cross-sectional approach illuminates patterns over time, we did not collect data from the same sample of providers, so this study is limited in the extent to which we can assign differences to variation between provider groups versus the effect of time and the pandemic on policy implementation.
Conclusions
The goal of the OBPP was to reduce reliance on opioid and expand access to evidence-based NPT for back pain through Oregon’s Medicaid program. This longitudinal follow-up study revealed that 6 years post implementation, OR providers continue to express support for the policy and experience benefits from it. However, they have faced persistent challenges in implementing the policy in practice, including challenges with referrals and a shortage of OHP-credentialed NPT providers to refer to. In the future, payer policies that expand coverage to new services may consider implementing systems and services to facilitate referral pathways and decrease the administrative burden on providers who already face low reimbursement rates. Policies of this kind should be rolled out with input from service provider stakeholders to define minimum benefit standards, streamline administrative load to optimize participation and availability, and boost the workforce. In addition, the pandemic’s stressors are unlikely to be singular; future pandemics and other health threats will make it critical to adapt and be capable of sustaining a wide variety of NPTs in times of system crisis.
Footnotes
Acknowledgments
The authors thank Rani George who engaged in discussion and review of this article. The authors express appreciation to research participants who contributed their time and opinions to this project.
Authors’ Contributions
M.G.: Methodology, validation, formal analysis, resources, data curation, writing—original draft, writing—review and editing, visualization, supervision, and project administration. A.C.: Validation, formal analysis, data curation, and writing—review and editing. C.L.: Conceptualization, methodology, investigation, resources, writing—review and editing, and funding acquisition. K.L.: Methodology, software, validation, resources, data curation, writing—review and editing, and project administration. D.F.: Resources, data curation, and writing—review and editing. E.C.: Conceptualization, methodology, investigation, resources, writing—review and editing, supervision, and funding acquisition.
Author Disclosure Statement
C.L. reports grants from National Institute on Drug Abuse (NIDA/NIH) for this research and a contract with the Kaiser Permanente Health Research Institute for an advisory role of a research study on this back pain policy. C.L. previously served as the Associate Medical Director of the Health Evidence Review Commission and is currently employed as the Medical Director of a Coordinated Care Organization. The remaining authors have no conflicts of interest to declare.
Funding Information
This work was supported by the National Institutes of Health, National Institute on Drug Abuse (R01 DA047323-01A1).