
Abstract
Objectives:
Several studies have indicated that dietary interventions may offer protection against the development of cardiac damage in the case of anthracycline-induced cardiomyopathy (AIC). The goal of this study was to assess whether an evidence-based cardioprotective diet can be effective in preventing AIC in patients with breast cancer.
Design:
Randomized, open-label, controlled trial. The study period was set for 18 weeks, and the data were analyzed by generalized estimating equation modeling and one-way repeated measures analysis of variance.
Setting/Location:
Shahid Rajaie Hospital affiliated (Tehran, Iran).
Subjects:
Fifty anthracycline-treated patients with breast cancer.
Interventions:
Patients were randomized to receive either a 2-hour training in evidence-based cardio-protective diet or Carvedilol 6.25 mg bid.
Outcome Measures:
The primary outcome was the number of patients with abnormal left ventricular ejection fraction (LVEF) after 18 weeks.
Results:
At week 18, 12 (48%) out of 25 participants in the cardioprotective diet group had abnormal LVEF in comparison with 21 (84%) out of 25 in the carvedilol group (p = 0.007). Also, 2 (8%) out of 25 in the cardioprotective diet group compared with 7 (28%) out of 25 participants in the carvedilol group had abnormal global longitudinal strain (p = 0.066). The diet group showed significant improvements in the quality-of-life dimensions named “health change” and “general health” compared with the carvedilol group using the Short Form-36 Health Survey questionnaire.
Conclusions:
This study suggests that an evidence-based cardioprotective diet can contribute to the prevention of AIC. Although current treatments for AIC can be effective, further research is mandatory for more options.
Introduction
Breast cancer is one of the leading causes of cancer-related deaths in women worldwide. 1 Anthracyclines, a class of chemotherapy drugs commonly used in the treatment of breast cancer, have been shown to be effective in improving survival rates. However, their use is limited by the potential for cardiotoxicity, which can lead to long-term cardiac damage and heart failure. 2
There is growing evidence that diet plays an important role in the prevention of cardiovascular disease and its associated complications. A diet rich in anti-inflammatory foods, such as fruits, vegetables, whole grains, and omega-3 fatty acids, has been shown to have cardioprotective effects by reducing inflammation, oxidative stress, and endothelial dysfunction. 3,4 In addition, certain dietary patterns, such as the Mediterranean diet, have been associated with a reduced risk of cardiovascular disease and improved cardiovascular outcomes. 5 In the context of anthracycline-induced cardiomyopathy (AIC), several studies have suggested that dietary interventions may have a protective effect against the development of cardiac damage. 6 For example, a study of patients with breast cancer receiving adjuvant treatment found that women with a higher dietary antioxidant capacity had lower levels of oxidative stress markers compared with women with a lower dietary antioxidant capacity. 7
Since 1967, anthracyclines have maintained a significant role in treating various solid tumors, including breast cancer. The cytostatic antibiotics of the anthracycline class are well-known for their association with cardiotoxicity, and their occurrence is not dependent on the administered dose. AIC can be categorized into three distinct types of cardiotoxicity: (1) Acute or subacute injury, which is a rare form of cardiotoxicity that may manifest immediately after a single dose or a course of anthracycline therapy within a week of treatment. (2) Early-onset progressive chronic cardiotoxicity, which is a more common type of AIC. It leads to the development of cardiomyopathy and occurs gradually during the early stages of treatment. (3) Chronic AIC, which usually presents within a year of treatment. 8
Although treatments for AIC exist, their efficacy can be inconsistent among patients. 8 Moreover, a standardized approach to managing AIC is lacking, making it challenging to compare treatment outcomes across various patient populations. 8 It is worth noting that because of the absence of a universally accepted standard of care for AIC, its management requires a team-based and personalized approach that factors in each patient’s distinct medical history and needs. This multidisciplinary approach helps to develop a tailored prevention or treatment plan that is best suited for the individual patient. 9 The present study aimed to evaluate the potential of an evidence-based cardioprotective diet in preventing AIC in patients with breast cancer.
Materials and Methods
Study design
This study was designed as a randomized, open-label, controlled trial to investigate the efficacy of an evidence-based cardioprotective diet in preventing early-onset cardiomyopathy in female patients with breast cancer undergoing chemotherapy with anthracyclines (doxorubicin or epirubicin), in accordance with the latest universal protocols. 10 The study was conducted between January 2022 and December 2023 at Shahid Rajaie Hospital affiliated with Iran University of Medical Sciences (Tehran, Iran).
The post hoc changes to the registered protocol were the change of single-blinded study to open-label one as it was challenging to keep the treatment assignments secret.
Participants
Female breast cancer patients undergoing chemotherapy with Anthracycline (no prior experience receiving anthracycline drugs), aged 18–65 years, with a left ventricular ejection fraction (LVEF) of ≥53% were included. Exclusion criteria were history of any kind of heart disease, diabetes mellitus, kidney or liver disease, history of psychiatric disease, body mass index more than 25 or less than 19, current use of ß-blockers,angiotensin-converting enzyme inhibitors or angiotensin receptor blockers, inability to adhere to the study protocol, and history of food sensitivity.
Intervention
During the 18-week study period, all participants were instructed to follow their usual care. The group assigned to the cardioprotective diet additionally received a 2-h training session led by a dietician with more than 10 years of clinical counseling based on evidence-based guidelines for a cardioprotective diet, which includes consuming fruits (4 to 5 servings per day), vegetables (4 to 5 servings per day), whole grains (>3 servings per day), fish (>2 servings per week), dairy products (2–3 servings per day), and vegetable oils 2–6 servings per day). 11 This group was also instructed to document their daily cardioprotective dietary intake regularly to track their compliance with the prescribed diet. The control group only received carvedilol 6.25 mg bid—an old drug type (ß-blocker) with promising effects on patients with AIC. 12 Meanwhile, both groups received standard chemotherapy treatment with anthracyclines. Although it is important to initiate chemotherapy promptly for patients diagnosed with cancer and it cannot be interrupted for dietary supplementation, the decision to introduce this intervention was made after participants had already received anthracycline medication, rather than before.
Sample size
With no previous studies appropriate for calculation of sample size, it was estimated that a sample size of 50 participants (25 in each group) would be sufficient to detect a 40% improvement to LVEF between the two groups, with a power of 80%, a significance level of 0.05, and a lost to follow-up rate of 10%.
Randomization
Participants were randomized in a 1:1 ratio to either the cardioprotective diet group or the carvedilol group using a free online random sequence generator (The Randomizer). 13 The randomization process employed a block randomization approach with block sizes of 4 and 6 in order to maintain similar group sizes and reduce the likelihood of chance imbalances between the treatment arms. Allocation concealment was achieved through centralized phone randomization.
Outcome measures
The primary outcome was the number of patients with abnormal LVEF after 18 weeks. Secondary outcomes included the number of patients with abnormal global longitudinal strain (GLS), quality of life (QoL) (SF-36), adherence to an evidence-based cardioprotective diet plan, and the number of patients with adverse events.
LVEF, a measure of the heart’s pumping capacity, is determined using echocardiography. It is calculated by dividing the volume of blood pumped out of the left ventricle during systole by the total volume of blood in the left ventricle during diastole. Confirmation of AIC requires a retest, with an LVEF value of less than 53% being considered an indicator of AIC. 14 In this study, the number of patients in each group with an LVEF < 53% after 18 weeks was compared.
GLS is another measure of heart function, which reflects the overall function of the heart muscle. It is determined using echocardiography and is a measure of the deformation or change in length of the heart muscle fibers during the cardiac cycle. A GLS value of more negative than −18% indicates better heart function. 15 In this study, the number of patients in each group with a GLS <−18% after 18 weeks was compared. Both LVEF and GLS were evaluated by the same cardiologist at the beginning (week 0) and at the end of the study (week 18).
QoL is a multidimensional construct that encompasses various aspects of an individual’s life that are important to their subjective experience. In this study, we used the validated Iranian version of the Short Form-36 Health Survey questionnaire (SF-36), 16 a widely used generic health-related QoL questionnaire for dietary interventions in various Iranian patients, 17 which assesses eight domains of health status including physical functioning, role limitations because of physical health, role limitations because of emotional problems, energy/fatigue, emotional well-being, social functioning, pain, health change, and general health to evaluate QoL. The scores on the SF-36 questionnaire varied from 0 (representing the poorest health status) to 100 (representing the optimal health status) for each dimension. 16 The patients completed the questionnaire at the beginning (week 0) and at the end of the study (week 18).
The safety of the interventions was evaluated by performing a descriptive analysis that compared the incidence of adverse events among the trial participants. The patients were provided with a form to record any adverse events experienced, including the date. They could also call the research assistant to consult about any adverse events. Also, adherence to the cardioprotective diet was evaluated using 24-h cardioprotective dietary recalls completed by the participants on a daily basis. It should be emphasized that they were only asked to recall their adherence to the specified cardioprotective dietary guidelines (i.e., fruits, vegetables, whole grains, fish, dairy, and vegetable oil) during this period, without the need to recall all their dietary intakes. We also regularly performed pill counts by gathering and tallying the returned medication bottles from the participants, enabling us to evaluate the number of pills taken and compare it to the expected amount according to the prescribed dosage and treatment duration.
Statistical analysis
Descriptive statistics were used to summarize baseline characteristics. Statistical differences between groups in the number of patients with abnormal LVEF and GLS at week 18 were analyzed by generalized estimating equation (GEE) modeling, and odds ratio and its 95% confidence interval (95% CI) were estimated. Differences in QoL on the SF-36 were analyzed by using one-way repeated measures analysis of variance. A post hoc analysis was performed to evaluate adherence to the cardioprotective diet during the study period. The significance level was set at p < 0.05. Statistical analysis was performed using Stata software (Version 11.2, College station, TX).
Ethical considerations
The study was performed in compliance with the guidelines of the Declaration of Helsinki. The protocol was approved by the Institutional Review Board of Shahid Beheshti University of Medical Sciences (IR.SBMU.RETECH.REC.1400.258), and all participants signed written informed consent before participation. This trial was registered in the Iranian Registry of Clinical Trials (IRCT20131218015860N7).
Results
This clinical study initially screened 62 female patients with breast cancer who were undergoing chemotherapy with anthracyclines. Twelve of these patients were excluded from the study for not meeting the inclusion criteria or declining to participate (Fig. 1). The remaining 50 participants were randomly assigned to either the cardioprotective diet group or the carvedilol group. No participants withdrew from the study during the trial or analysis period. Therefore, the analysis included all 50 participants, with 25 in the cardioprotective diet group and 25 in the carvedilol group. Figure 1 illustrates the enrollment, randomization, and analysis process in detail.
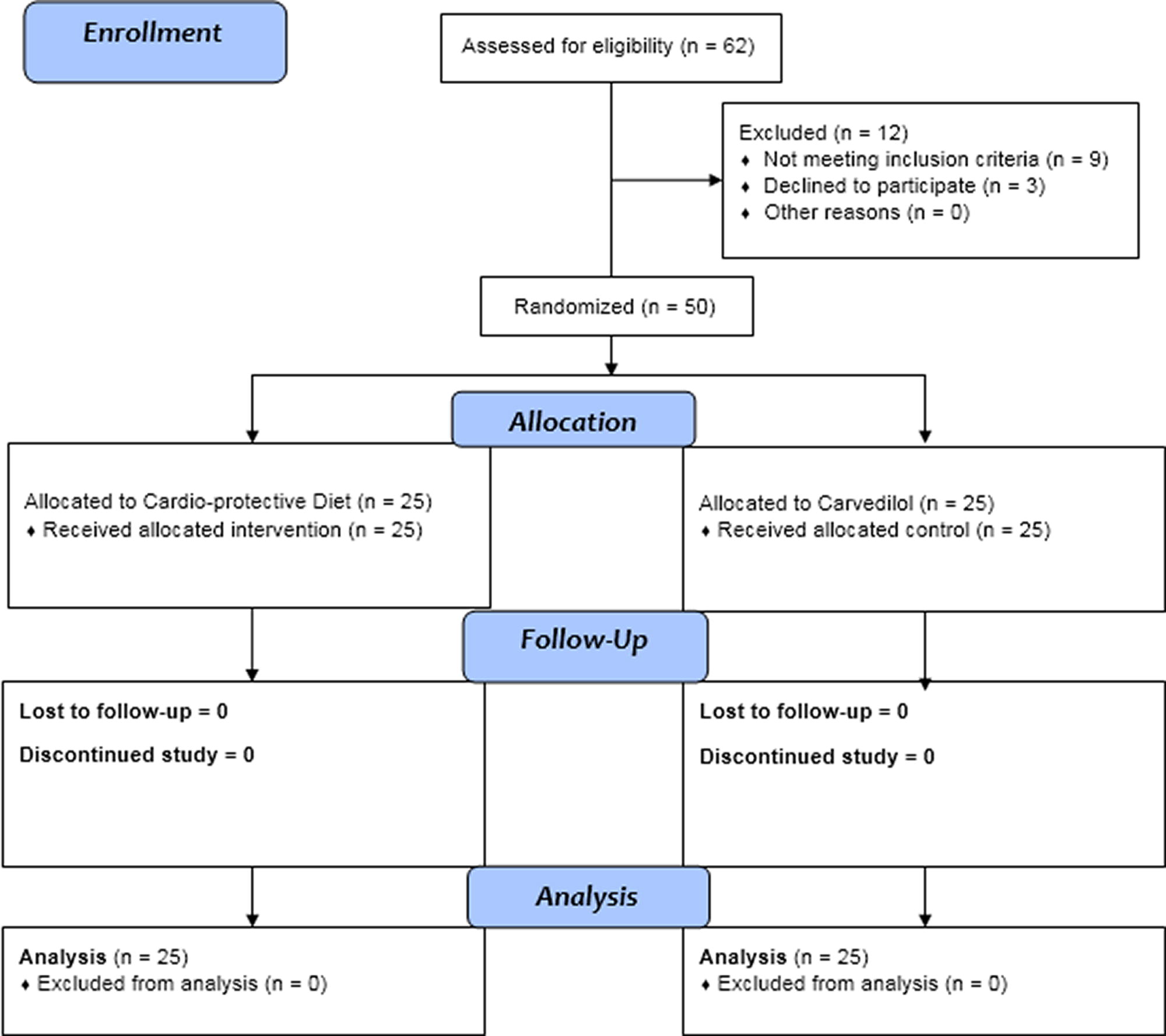
CONSORT flowchart of participants.
The cardioprotective diet group had a mean age of 46.96 ± 10.71 years, whereas the carvedilol group had a mean age of 51.68 ± 11.73 years. The 95% CI for the mean age in both groups ranged from 46.0886 to 52.5514. In terms of weight, the cardioprotective diet group had a mean weight of 70.24 ± 11.43 kg, whereas the control group had a mean weight of 74.84 ± 12.42 kg. The 95% CI for the mean weight in both groups was 69.1162 to 75.9598 (Table 1).
Participant Baseline Characteristics
ER, estrogen receptor; HER2, human epidermal growth factor receptor 2; PR, progesterone receptor; SD, standard deviation.
At week 18, 12 (48%) out of 25 participants in the cardioprotective diet group had abnormal LVEF in comparison with 21 (84%) out of 25 in the Carvedilol group (p = 0.007). The study also found that patients in the cardioprotective diet group had lower odds (about 66% less) of experiencing a change in LVEF compared with the Carvedilol group (p = 0.033).
Two (8%) out of 25 in the cardioprotective diet group compared with 7 (28%) out of 25 participants in the carvedilol group had abnormal GLS (p = 0.066). The study found that patients in the cardioprotective diet group had about a 36% lower odds of experiencing a change in GLS compared with participants in the carvedilol group (p = 0.183).
The study evaluated QoL using the SF-36 form, and the results are presented in Table 2. The findings suggest that the cardioprotective diet group showed a statistically significant improvement in the dimensions of “health change” (p = 0.037) and “general health” (p = <0.001) compared with the carvedilol group. However, there was no significant difference observed in other dimensions of QoL.
Different Dimensions of Quality of Life in Participants Who Received Either the Intervention or Carvedilol at the End of the Trial
A statistical division of a dataset into three equal parts.
EF, energy/fatigue; EWB, emotional well-being; GH, general health; HC, health change; PF, physical functioning; RLEP, role limitations because of emotional problems; RLPH, role limitations because of physical health; SF, social functioning.
During the study, the adherence rate to the cardioprotective diet was found to be 78% using 24-h cardioprotective dietary recalls (Supplementary Data S1). There were a few minor adverse effects such as mild abdominal cramps and mild pruritus in the carvedilol group. These effects were not significant enough to cause the patients to discontinue the trial.
Discussion
The trial found that the cardioprotective diet had a preventive effect on LVEF in patients with breast cancer with AIC compared with carvedilol, although this difference was not statistically significant for GLS. In addition, two dimensions of QoL were found to be significantly higher in the cardioprotective diet group. To our knowledge, this is the first study on the potential of cardioprotective diet therapy in preventing AIC in patients with breast cancer.
There are two types of strategies to prevent AIC: primary and secondary prevention. 18 Primary prevention is the preferred approach and can reduce the risk of cardiac damage during cancer treatment. The American Society of Clinical Oncology guidelines, endorsed by the American Heart Association, recommend several primary prevention strategies during cancer treatment. 19 Previous research suggests that cardiovascular risk can be reduced through interventions such as maintaining appropriate weight, following a heart-healthy diet, getting enough exercise, and avoiding tobacco exposure. 20 The observed significant improvement in LVEF among the group that followed the cardioprotective dietary recommendations may be attributed to their diligent effort in adhering to a heart-protective regimen, which has the potential to control weight.
ß-Blockers are commonly used to treat AIC because they can block the progression of heart disease through the neurohormonal cascade. Carvedilol, in particular, has been used for primary prevention because of its additional antioxidant activity. 21 However, early clinical studies on using ß-blockers during chemotherapy to prevent AIC in adults have had mixed results. One such study, called the Carvedilol Effect in Preventing Chemotherapy-Induced Cardiotoxicity, compared carvedilol to a placebo in 192 women with breast cancer and found that carvedilol did not affect the early reduction of LVEF. 22 Other similar studies also did not find significant differences in LVEF between the carvedilol and placebo groups after chemotherapy. 23 –25 It appears that the cardioprotective diet is more effective than a commonly used approach in preventing AIC. However, it is important to note that a direct comparison of the effectiveness of different interventions for preventing or treating AIC is difficult since there is a lack of consistent criteria to diagnose or grade AIC, and the underlying mechanisms of AIC are complex.
Several limitations should be considered when interpreting the results of this study. The main limitation is that the study was open-label, which may have introduced bias into the results. Another limitation of the study was the absence of cardioprotective dietary recalls for patients in the carvedilol group. This lack of cardioprotective dietary recall data may have introduced bias into the results, especially for patients who potentially consumed a substantial amount of the cardioprotective diet during their treatment period. Lack of a nutrition analysis program was another shortcoming that should be addressed in future studies. It would be valuable for future studies to incorporate pre- and posttest measurements of cholesterol levels or antioxidant markers as objective indicators of dietary adherence, or to use random phone calls for dietary recalls. These objective measures can provide a more robust assessment of the impact of the dietary intervention and help validate self-reported dietary data, thereby enhancing the validity and reliability of the findings.
However, the study’s findings suggest that a cardioprotective diet may have the potential as a preventive approach for AIC in female patients with breast cancer. Furthermore, the finding that two dimensions of QoL were significantly higher in the cardioprotective diet group could be an important consideration when developing treatment plans for patients with breast cancer. The study can provide useful information for designing future clinical trials to investigate the potential of the cardioprotective diet or other dietary interventions for preventing AIC in patients with breast cancer. Therefore, larger, randomized studies are needed to further investigate the potential of the cardioprotective diet or other dietary interventions for preventing AIC in patients with breast cancer.
Conclusions
The cardioprotective diet has the potential to contribute to the development of novel diet-based approaches to prevent chemotherapy-induced toxicities in patients with breast cancer. The findings of this study may also have broader implications for the use of diet-based interventions in cancer prevention and treatment. Overall, while the current treatments for AIC can be effective in improving cardiac function and reducing the risk of heart failure, there is a need for further research to identify new and more effective treatment options for this condition.
Footnotes
Acknowledgments
The authors would like to be grateful to the patients who participated in this research.
Confirmation Statement
All of the authors declare that they are employed at an academic or research institution as researchers or faculty members where research or education is the primary function of the entity.
Authors’ Contributions
Conception and designing of study (A.A., M.M.M., G.H.); data collection (M.K., F.F.); data analysis (H.M., M.P., H.C.); article drafting (A.A., M.M.M., H.R., M.K., F.F., M.P., G.H.); critical revision (A.A., H.C., M.P., G.H.); supervision (A.A., G.H.); all the authors read and approved the final version of the article.
Authorship
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this article, take responsibility for the integrity of the work as a whole, and have given their approval for this version to be published.
Author Disclosure Statement
The authors declare that there is no competing interest.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Data S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.