
Abstract
Background:
Restless legs syndrome (RLS) is frequent in patients with hemodialysis (HD) and occurs predominantly in its most severe forms. The study was conducted to evaluate the efficacy and safety of acupuncture for RLS in patients with end-stage renal disease (ESRD) at hospital-based HD center.
Methods:
This single-blind, randomized controlled trial was performed on patients with HD and RLS who were randomly assigned to the experimental group and control group. Data were collected using the International Restless Legs Syndrome Rating Scale (IRLSRS), Insomnia Severity Index (ISI), and heart rate variability (HRV) records at baseline, after the therapeutic course (12 times/4 weeks), and 1-week follow-up.
Result:
A total of 47 patients were evaluated with IRLSRS score from 11 to 30 in this study. There were 41 patients enrolled in the study based on inclusion/exclusion criteria and allocated randomly into two groups. A total of 35 participants completed the trial, including 18 subjects in the experimental group and 17 subjects in the control group. The comparison of IRLSRS and ISI showed a significant reduction between two groups after acupuncture treatment (p = 0.002, p = 0.003). The ISI after 1-week follow-up also revealed significant decrease (p = 0.003). This HRV results showed that high frequency (HF%) increased significantly (p = 0.021) and low frequency (LF%) decreased significantly in the acupuncture group (p = 0.021). The generalized estimating equation showed that the IRLSRS improved by 2.902 points (p < 0.001) in the acupuncture group compared with the control group and by 1.340 points (p = 0.003) after 1-week follow-up. There were no adverse effects observed during HD in this study.
Discussion:
The authors conclude that acupuncture could effectively improve the symptoms of RLS significantly. The results from this study provide clinical evidence on the efficacy and safety of acupuncture to treat the patients with RLS at the HD center.
Introduction
Restless legs syndrome (RLS) is a neurologic sensory disorder with symptoms involving an often unpleasant or irresistible urge to move the legs that occurs during periods of inactivity, particularly in the evenings, and is transiently relieved by movement. 1 RLS can be primary or can occur as a secondary disorder in association with medical conditions, including low iron levels, kidney failure, Parkinson’s disease, diabetes mellitus, and pregnancy. 2 Common consequences of RLS include sleep-onset insomnia, nocturnal awakenings, quality of life, depression, anxiety, and cardiovascular disease. 3
Studies in patients with end-stage renal disease (ESRD) showed a prevalence of RLS ranging from 12% to 62%, which is significantly higher than the general population. 4,5 Current drug treatments, such as dopaminergic drugs, have been widely used for RLS. While some previous studies have shown initial improvement in symptoms, longer-term and clinical studies have reportedly shown that treatment effectiveness decreases over time, and dopaminergic augmentation has been reported to be the main cause of treatment failure for RLS. 6,7 Nonpharmaceutical methods, such as acupuncture, also known as complementary and alternative therapies, are safer and have fewer complications than the pharmaceutical methods. 8 –10
Acupuncture is a part of the ancient practice of traditional Chinese medicine (TCM). 11 Recent studies reported that acupuncture stimulation of certain meridian points could be used to manage numerous symptoms and treat various diseases. 12,13 Needles may be manipulated in various ways, including spinning, flicking, or moving up and down relative to the skin according to acupuncture skills. TCM indicates that acupuncture stimulation elicits de qi, a compound of unique sensations. 14 It is believed that de qi may be an important variable in the studies of the mechanism and efficacy of acupuncture treatment. In addition, acupuncture might involve neurobiologic mechanisms such as central sensitization, neurotransmitters, neuroinflammation, and the spinal and supraspinal mechanisms. 15 –17
Few randomized clinical trials have shown the benefits of acupuncture on the treatment of HD patients with RLS. 18 The purpose of this study is to examine the additive effect of medical acupuncture on controlling the symptoms of RLS in a single-blind, randomized, and controlled study. Their study focused on evaluating the efficacy and safety of acupuncture in patients with HD for RLS at a hospital-based HD center.
Materials and Methods
Study design and setting
This trial was a randomized, single-blind, and placebo-controlled study. This trial was conducted at the HD center in Changhua Christian Hospital (CCH), Taiwan from November 2019 to October 2021. The study was approved by the institutional review boards of the CCH, Taiwan. The registration ID for this prospective study at the ClinicalTrials.gov was NCT04356794. Written informed consent was obtained from all patients.
Participants
Subjects who voluntarily signed a consent form underwent the trial according to the study design. Patients were eligible for inclusion if they met the following criteria: (1) informed consent to participate in the study; (2) between the ages of 20–80 years; (3) a score from 11 to 30 on the International Restless Legs Syndrome Rating Scale (IRLSRS, correspondence between moderate and severe RLS); (4) a history of chronic renal failure treated with regular and continuous HD for at least 3 months; (5) no acupuncture treatment in the last one month; (6) no taking drugs for RLS, such as dopamine agonists, benzodiazepines, opioids, and gabapentin at the time of this study.
The exclusion criteria were as follows: (1) an unwillingness to continue to participate in the study; (2) vascular access in the leg area, such as an arteriovenous shunt; (3) the presence of peripheral neuropathy and vascular problems in the lower extremities; (4) a history of other motor disorders, such as Parkinson’s disease, dyskinesia, and dystonia; (5) with an artificial cardiac pacemaker; (6) pregnancy or breastfeeding; (7) taking any sleeping or sedative medication.
Randomization and allocation concealment
After initial assessments, subjects will be assigned to 1 of 2 groups with a 1:1 allocation ratio according to a computer-generated randomization list. The group each subject is allocated to will be concealed in sequentially numbered sealed opaque envelopes. The envelopes will only be opened after the subject has completed baseline clinical assessments. Randomization allocation will be concealed from the physician, subjects, and evaluators.
Interventions
This study evaluated the efficacy of acupuncture treatment compared with the control group, and to evaluate the feasibility of large clinical trials. In the hopes of decreasing the subject dropout rate, the trial was designed to only 5 weeks (4 weeks for treatment and 1 week for follow-up). The experimental group received total 12 acupuncture treatments which was performed thrice per week for 4 weeks. Based on the theory of TCM and clinical literature on acupuncture therapy for the obese, the acupoints were as follows: ST36 (Zusanli), GB34 (Yanglingquan), SP10 (Xuehai), SP6 (Sanyinjiao), BL57 (Chengshan), KI7 (Fuliu), and LIV2 (Xingjian). All acupoints were localized according to the WHO Standard Acupuncture Locations. Treatment was performed by licensed acupuncturists who have at least 5 years of experience in acupuncture. The acupuncture points were stimulated by needle insertion, then manipulations of twirling, lifting, and thrusting performed for de qi sensation (a compositional sensation, including soreness, numbness, distention, and heaviness). Each acupuncture treatment lasted 20 min.
The control group received sham acupuncture by pasting seed patches at nonacupoints. The nonacupoints were displaced by 1 cm from correct acupoints of experimental group. The therapist did not perform any massage or press stimulation to prevent acupressure effect.
Outcome measurements
The primary outcomes were the evaluation of IRLSRS and the Insomnia Severity Index (ISI). The IRLSRS was developed by the IRLS Study Group to assess the severity of a patient’s RLS symptoms. Ten questions are listed in the questionnaire, and the sum of the item scores is graded from 0 (none) to 40 (very severe). 19 The other questionnaire is ISI designed as a brief screening tool for insomnia. The seven-item questionnaire asks respondents to rate the nature and symptoms of their sleep problems using a Likert-type scale. The sum of the item scores is graded from 0 (no clinically significant insomnia) to 28 (severe). 20
The second outcomes were the parameter change of heart rate variability (HRV) in the HD patients with RLS. This study monitored physiological parameter changes before, after acupuncture treatment, and follow-up. Blood pressures, heart rate (HR), and HRV were measured using an ANSWatch® monitor developed by Taiwan Scientific Corp./Ledron Technology Corp., Taiwan. The HRV was analyzed in both time and frequency domains to give rise to parameters that are linked to the low frequency component (LF), the high frequency component (HF), and the LF/HF ratio, and the standard deviation of adjacent peak-to-peak intervals which represents the total HRV activity(ms) and root mean square of the successive differences (RMSSD) is one of a few time-domain tools used to assess HRV. The successive differences of neighboring RR intervals were all analyzed based on the international standard. To avoid interference from the environment, both meridian energy 2-level and HRV were recorded with subjects in a recumbent position after a 15-min rest. All evaluations were conducted before the trials, after the treatment, and 1-week follow-up after the last treatment.
Sample size
In the hopes of decreasing the subject dropout rate, the trial is designed to only last 5 weeks. The minimum sample size for estimating the difference in the mean change in activity level of HF% between the experimental and control groups was with an effect size of 0.80. Based on the a priori calculation in the statistical software G*Power 3.1.9.2, it was determined that a minimum total sample size of 52 would be needed in the independent samples t test to show a significant difference. Assuming a dropout rate of 15%, the desired sample size for this study was 62 subjects.
Safety
Participants should report any adverse events experienced, including discomfort or bruising at the sites of needle insertion, nausea, or feeling faint after treatment.
Statistical methods
All analyses were performed on the per-protocol population of participants who had completed whole trail. Participants’ demographic information and levels of major measured variables were analyzed by descriptive statistics. The generalized estimating equation (GEE) to fit a linear regression model was used to analyze longitudinal data of the two acupuncture modes for each clinical index across the 2 data collection points that yield robust standard errors estimated in the model. A value of p < 0.05 was regarded as statistically significant for the above statistical analyses.
Results
A total of 47 patients were evaluated with IRLSRS score from 11 to 30; 41 patients were enrolled in the study based on inclusion and exclusion criteria and allocated randomly into two groups. One group is the experimental group with acupuncture treatment (n = 20), and the other is the control group by pasting seed patches at nonacupoints (n = 21). Three patients in the experimental group dropped out of the study because they could not tolerate the pain of acupuncture. In the control group, three subjects did not end the study (two were because of the poor response of the treatment, one is a conflict with other physical treatments prescribed for concomitant diseases). A total of 35 patients (the control group, n = 18; the experimental group, n = 17) who completed the study were analyzed. A flow diagram of the study is shown in Figure 1.
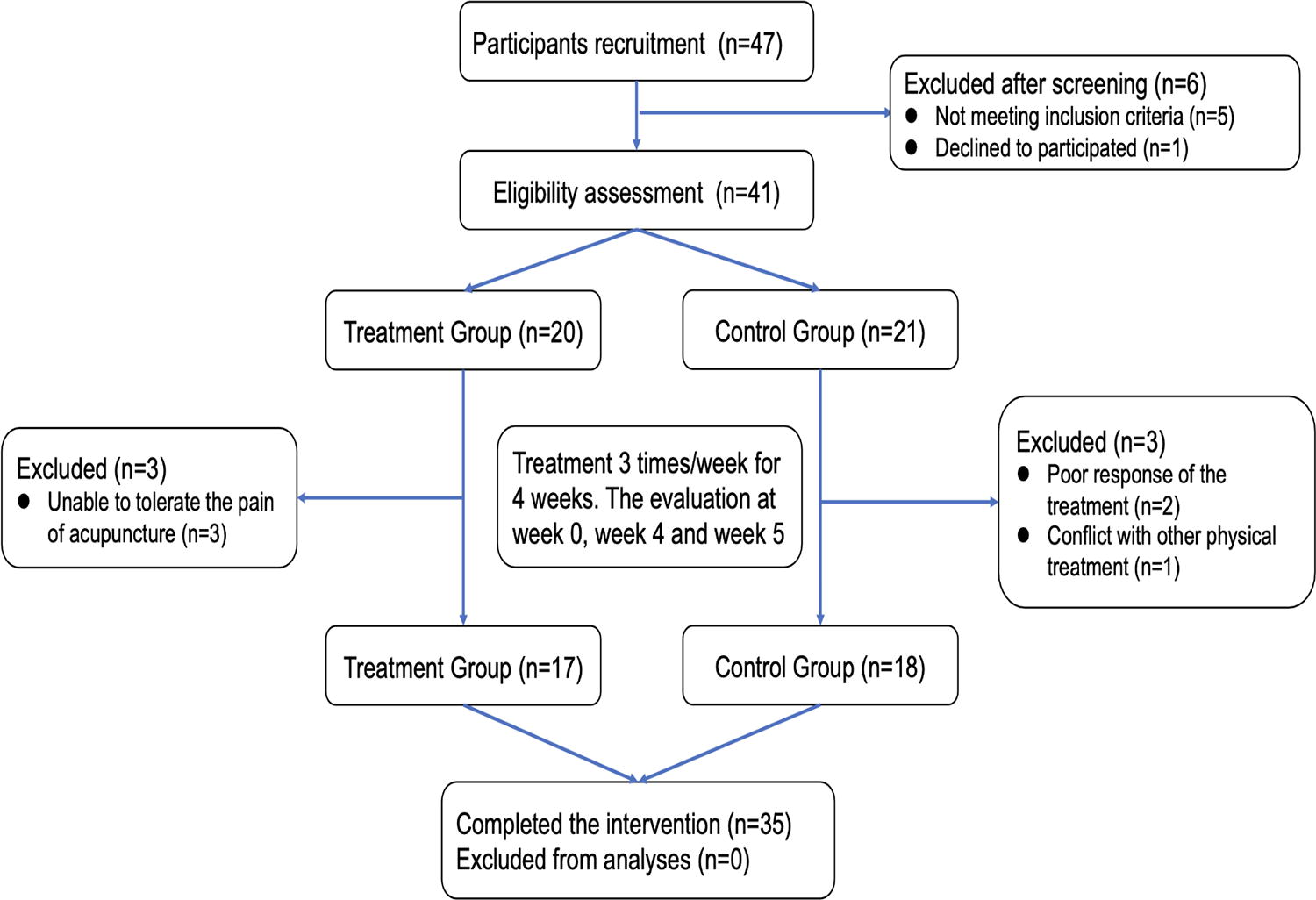
CONSORT flow diagram of enrollment, randomization, and treatment.
The baseline characteristics of the participants in the experimental and control groups are shown in Table 1. The IRLSRS and ISI of the participants were as follows: in the control group, average IRLSRS was 22.3 ± 2.9 and mean ISI was 14.6 ± 1.8; and in the experimental group, average IRLSRS was 21.9 ± 2.8 and mean ISI was 14.3 ± 2.1. There was no significant difference between two groups in IRLSRS and ISI baseline assessment.
Baseline Participant Characteristics
p-Value by independent t test or Chi-square test if needed.
BMI, body mass index; DM, diabetes mellitus; Hb, hemoglobin; HF%, high frequency; HTN, hypertension; HRV, heart rate variability; IRLSRS, International Restless Legs Syndrome Rating Scale; ISI, Insomnia Severity Index; LF%, low frequency; LF/HF, sympatho-parasympathetic balance index; SD, standard deviation; SDNN, standard deviation of NN intervals.
The comparison of parameters of HRV after acupuncture stimulation and follow-up is tabulated in Table 2. The experimental group exhibited significant differences in post-treatment HF% and LF% (p = 0.021). There was no significant difference in parameters of HRV observed in the follow-up period.
Parameters of Heart Rate Variability After Acupuncture Stimulation and Follow-up Between the Control Group and the Experimental Group
p-value by Independent Samples t test.
Values represented as mean ± SD.
Follow-up: 1 week follow-up after post-treatment.
p < 0.05.
HF%, high frequency; HRV, heart rate variability; LF%, low frequency; LF/HF, sympatho-parasympathetic balance index; SD, standard deviation; SDNN, standard deviation of NN intervals.
The comparison of IRLSRS and ISI of study participants after acupuncture stimulation and follow-up is tabulated in Table 3. The comparison of IRLSRS and ISI showed a significant reduction between two groups after acupuncture treatment (p = 0.002, p = 0.003). The ISI after 1-week follow-up also revealed significant decrease (p = 0.002). However, the variation of IRLSRS showed no significant difference after 1-week follow-up (p = 0.100). The changes in IRLSRS and ISI before treatment, after treatment, and 1-week follow-up are shown in Figure 2.
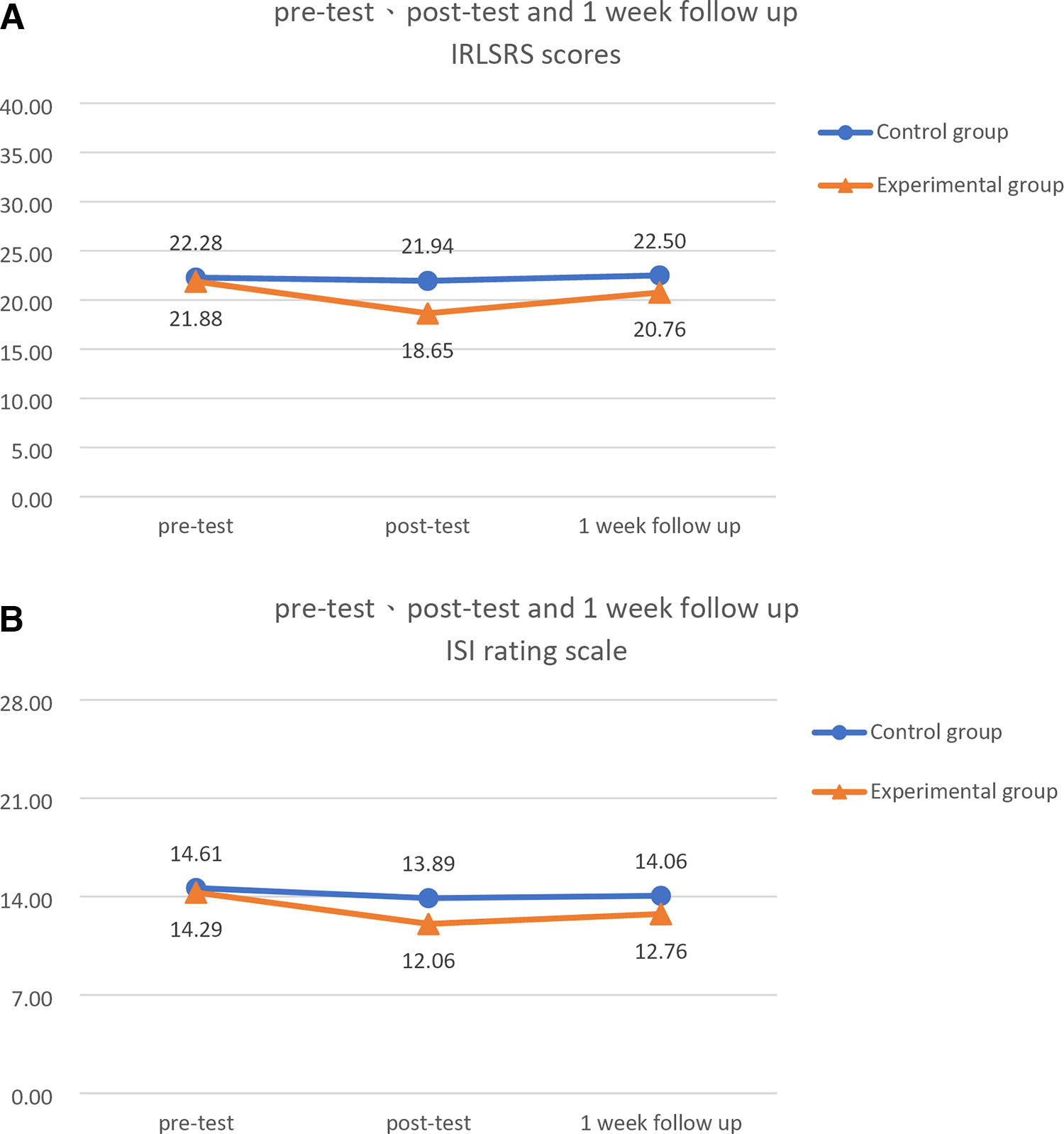
The changes in IRLSRS and ISI before treatment, after treatment, and 1-week follow-up. IRLSRS, International Restless Legs Syndrome Rating Scale; ISI: insomnia severity index.
Comparison of IRLSRS and ISI of Study Participants After Acupuncture Stimulation and Follow-up Between the Control Group and the Experimental Group
p-value by independent samples t test. Values represented as mean ± SD.
p < 0.05.
p < 0.01.
IRLSRS, International Restless Legs Syndrome Rating Scale; ISI, Insomnia Severity Index; SD, standard deviation.
Table 4 revealed GEE Model results. It reveals that using acupuncture as an intervention resulted in an improvement of 2.902 points in the IRLSRS score compared with that of the control group, achieving statistical significance (p = 0.000). After one week, the improvement was 1.340 points, still achieving statistical significance (p = 0.003). Therefore, acupuncture effectively alleviated restless legs syndrome. In addition, acupuncture resulted in an improvement of 1.513 points in the ISI score compared with that of the control group, achieving statistical significance (p = 0.006). However, the two groups did not exhibit a significant difference in their 1 week follow-up.
Generalized Estimating Equation Model
The authors used the adverse event record to assess the safety. During the administering of acupuncture, some participants withdrew due to the pain caused by acupuncture. However, none stopped kidney dialysis due to acupuncture or experienced adverse effects or accidents. Neither physical examination nor laboratory tests revealed any adverse changes after additional treatment in either group at the end of the study. Therefore, administering acupuncture could be a safe treatment in patients during dialysis.
Discussion
Their study was designed to demonstrate that patients with HD and RLS can benefit from the application of acupuncture. In this study, instead of recruiting participants from outpatient clinics of acupuncture, the authors cooperated with nephrologist in order to enroll patients with RLS at HD center. Clinically the authors found that patients with HD must maintain the lying down posture during hemodialysis. Therefore, all the acupoints the authors chose in this study were at the lower limbs and based on TCM meridian system, so patients could maintain a relatively comfortable position and without interruption during hemodialysis. This study is the first one to apply acupuncture to treat patients with RLS at HD center.
The results of this study indicated that acupuncture could effectively alleviate symptoms in patients with HD and RLS. After the acupuncture treatment session, the symptoms of RLS were improved using the assessment scales, including IRLSRS and ISI. Then, after 1-week follow-up, the effect persisted despite a rise in the IRLSRS score. Acupuncture was also found to alleviate insomnia, but its effect decreased after 1-week follow-up. In addition, ISI of the control group improved during placebo treatment, but also decayed after 1-week follow-up. This could be attributable to the placebo effect in the control group.
HRV is an ordinarily assessed indicator for autonomic nervous system (ANS) dysfunction and is an important noninvasive marker for estimating cardiac autonomic function. 21 –23 In disorders concomitant with ANS dysfunction, such as diabetes mellitus (DM), congestive heart failure, and ESRD, a decrease in HRV is habitually found, with abnormal HRV being contemplated an independent risk factor for mortality. 24,25 Several lines of evidence suggested that patients with RLS have ANS abnormalities. 26,27 Recent studies indicated that a decreased HRV is usually found in HD patients accompanied with abnormal HRV, which is considered an independent risk factor for mortality. 28 –30 The LF power and LF/HF ratio were significant in patients with RLS. 31 This study reported that elevated sympathetic activity might be beneficial in relieving RLS symptoms. 32 However, their results indicated that HF% increased significantly in experimental group (from 47.9 ± 22.0 to 66.2 ± 18.4, p = 0.008). Therefore, this study inferred that the improvement in a patient with RLS might have been caused by a change in autonomic nervous activity, mainly the enhanced parasympathetic activity.
However, there were some limitations of this study. First, small sample size, which may result in the statistical bias of the baseline and outcome assessments. The authors calculated the original estimated enrollment total sample size as 62 subjects. However, the authors actually enrolled 35 participants because COVID-19 pandemic influenced the project’s recruitment. Second, the relatively short intervention and follow-up period in this trial is another limitation. Further studies with a greater sample size and longer follow-up duration should be conducted. Third, this study was not designed as double-blind trail. Considering that acupuncture is well-known, it is difficult to carry on blinded study about acupuncture. To minimize the bias from this, the authors used seed patches as sham acupuncture method. The authors tried to convince the participants in control group that they were also receiving placebo treatment by pasting the seed patches near the acupoints. Thus, the biases due to this unblinded approach cannot be ruled out. For further research, larger sample studies are needed to prove the long-term effects of acupuncture. Prospective, multicenter cohort studies and multivariate statistical analysis can also be performed to provide a more practical and rigorous clinical research model for acupuncture clinical trials.
Conclusion
The authors conclude that acupuncture could effectively improve the symptoms of RLS significantly. The results from this study provide clinical evidence on the efficacy and safety of acupuncture to treat the patients with RLS at the HD center. However, further larger studies are needed to replicate the findings of this study.
Footnotes
Acknowledgments
The authors thank all of the colleagues who helped contribute to this study. The authors are grateful to the anonymous reviewers for their valuable comments. The authors thank the Changhua Christian Hospital, Taiwan for the grant support. This study was supported by program grants from Ministry of Science and Technology, Taiwan (NSTC112-2320-B-039–043), and China Medical University Hospital, Taiwan (DMR-111–197, CMU111-S-42, DMR-112-003, DMR-HHC-112-10, CMU112-S-25).
Ethics Approval and Consent to Participate
The Changhua Christian Hospital Ethics Review Board (IRB No: 170217).
Authors’ Contributions
All authors read and approved the final article.
Author Disclosure Statement
The authors declare that they have no competing interests with respect to the current trial.
Funding Information
No funding was received for this article.