
Abstract
Objectives:
Evidence suggests that post-coronavirus disease 2019 (COVID-19) is associated with reduced health-related quality of life, and up to 80% of those infected with COVID-19 may experience these symptoms. The objective of the present study was to identify the effects of individualized homeopathic medicinal products (IHMPs) against placebos in postCOVID-19 conditions.
Design:
Double-blind, randomized (1:1), two parallel arms, placebo-controlled, feasibility trial.
Setting:
D. N. De Homoeopathic Medical College & Hospital, Kolkata, West Bengal, India.
Subjects:
Sixty participants with post-COVID-19 conditions.
Interventions:
Group verum (n = 30; IHMPs plus concomitant care) versus group control (n = 30; placebos plus concomitant care).
Outcome Measures:
Feasibility issues; primary—post-COVID-19 symptoms checklist; secondary—Measure Yourself Medical Outcomes Profile version 2 (MYMOP-2); all of them were measured at baseline, and monthly intervals, up to 3 months. The intention-to-treat sample was analyzed; group differences were reported using descriptive statistics: means, 95% confidence intervals (CIs), and between group effect sizes (Cohen’s d).
Results:
Feasibility concerns showed promise; recruitment, retention, and attrition rates were 34.2%, 95%, and 5%, respectively. Group differences in both primary and secondary outcomes favored IHMPs against placebos: symptoms checklist score mean difference after 3 months: −4.2, 95% CI −4.9 to −3.4, d = 2.854 and MYMOP-2 mean difference after 3 months: −2.2, 95% CI −2.8 to −1.7, d = 2.082, respectively. Natrum muriaticum (11.7%), Pulsatilla nigricans (10%), Rhus toxicodendron (8.3%), and Calcarea carbonica (8.3%) were the most frequently prescribed remedies.
Conclusions:
IHMPs produced better results than placebos in reducing symptoms checklist scores and MYMOP-2 scores in the treatment of post-COVID-19 conditions. Definitive trials are warranted to confirm the findings.
Introduction
After the declaration of the coronavirus disease 2019 (COVID-19) pandemic, the world continues to face its devastating impact, not only on morbidity, mortality, and healthcare services but also its tremendous societal and economic consequences. 1 Sequels after the SARS-CoV-2 infection, especially dyspnea, fatigue, and mental health issues, are becoming an important burden to societies, healthcare systems, and the economy in India. 2 The consequences of previous coronavirus infections are not well understood, and it is unclear if they may be reproduced in SARS-CoV-2-infected patients. Along with pulmonary function, 3–4 COVID-19 can have an impact on one’s renal, 5 cardiovascular, neuropsychiatric, 6 and nutritional health. 7 Up to 12 months following the infection, recovered patients may experience persistent COVID-19 symptoms. The main symptom remains fatigue, but after 6 months, persistent pain starts to become increasingly severe. 8 According to study findings, post-COVID-19 patients may endure weariness, diminished functional ability, persistent respiratory symptoms, and a lower quality of life for up to 6 months following infection. 9 Fatigue, altered taste and smell, and memory and concentration issues were the most common complaints. Older age and the quantity of acute phase symptoms were predictive factors for postCOVID. 10 Fofty-two percent of the study population reported having one or more sequelae according to a survey. The likelihood of sequelae was much higher in older patients. 11 Clinical testing conducted after COVID-19 showed that 20% of patients had mild hypogeusia lasting up to 6 months, and 75% of patients had hyposomnia or anosmia. 12
PostCOVID-19 condition occurs in individuals with a history of probable or confirmed SARS-CoV-2 infection, usually 3 months from the onset of COVID-19 with symptoms that last for at least 2 months and cannot be explained by an alternative diagnosis. 13 Common symptoms include fatigue, shortness of breath, and cognitive dysfunction also others, which generally have an impact on everyday functioning. Symptoms may be new onset, following initial recovery from an acute COVID-19 episode, or persist from the initial illness. Symptoms may also fluctuate or relapse over time. A separate definition may be applicable for children. Study reveals around 1 in 5 respondents testing positive for COVID-19 exhibit symptoms for 5 weeks or longer. 14 Research reveals concerning rates of prolonged COVID-19 symptoms remaining in over 37% of people who have recovered from the virus. 15 There is evidence that patients with severe COVID-19 had significantly lower quality of life scores than those with non-severe COVID-19. 16
In a recently published randomized-controlled trial (RCT) on post-COVID-19 fatigue, individualized homeopathic medicinal products (IHMPs) demonstrated statistically significant results against placebos 17 ; however, other post-COVID-19 symptoms remained unevaluated. Thus, in the dearth of conclusive evidence, IHMPs were compared in this feasibility RCT against placebos in the treatment of post-COVID-19 conditions.
Materials and Methods
Trial design
This double-blind, randomized (1:1), placebo-controlled, two parallel-arms, feasibility trial was conducted at the outpatient department of D. N. De Homoeopathic Medical College and Hospital, Govt. of West Bengal, India. Based on the research, a full dissertation was submitted as the postgraduate thesis of the corresponding author to The West Bengal University of Health Sciences, Kolkata.
Ethics approval and trial registration
The study protocol was approved by the Institutional Ethics Committee (IEC) (Memo. No. DHC/Eth-45/2018/746/2021; dated October 26, 2021) and was registered prospectively in the Clinical Trials Registry—India [CTRI/2022/04/041852]. It had a secondary identifier—a universal trial number (UTN) of U1111-1276-9907.
Key components of the protocol are available at: https://ctri.nic.in/Clinicaltrials/pmaindet2.php?trialid=68226&EncHid=&userName=post%20covid-19 (Supplementary Appendix SA1).
The protocol adhered to the latest revision of the Declaration of Helsinki on human experimentation and followed the guidelines for Good Clinical Practice. 18 Before recruitment, each patient was provided with a patient information sheet in local vernacular Bengali, and subsequently, written informed consent was obtained from all the participants.
Participants
The inclusion criteria were the patients with postCOVID-19 condition—individuals with a history of confirmed SARS-CoV-2 infection, usually 3 months from the onset of COVID-19 with symptoms that last for at least 2 months, and those could not be explained by an alternative diagnosis. 13 Symptoms might have a new onset following initial recovery from an acute COVID-19 episode or persist from the initial illness. Symptoms might also fluctuate or relapse over time (ICD-10 diagnosis code: U09). The participants were of either sex or transgender, aged between 18 and 65 years, and literate patients with the ability to read English, Hindi, and/or Bengali, patients willing to participate in the study and giving written informed consent voluntarily. Exclusion criteria were the patients having pneumonia that was detected by clinically and/or radiologically, terminally or critically ill patients, SpO2 saturation below 95% at room air, any abnormality as detected by blood test (liver enzymes, lipid profile, urea, creatinine, fasting blood sugar), 19 chest X-ray and Electrocardiogram, subjects with hypertension (systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg) 20 or hypotension (systolic blood pressure <90 mmHg and/or diastolic blood pressure <60 mmHg), 21 self-reported chronic diseases, such as uncontrolled diabetes, diabetic ketoacidosis, heart disease, liver disease, and kidney disease conditions, subjects with active or untreated malignancy or recovered from malignancy, currently sufferers from asthma/chronic obstructive pulmonary disease, patients already taking any other form of treatment or willing to continue that alongside homeopathy for post-COVID-19 conditions, vulnerable population—unconscious, non-ambulatory, too sick for consultation, differently abled, mentally incompetent people, diagnosed cases of unstable psychiatric complaints or other systemic diseases affecting the quality of life, pregnant, lactating and puerperal women, self-reported immune compromised conditions, and substance abuse and/or dependence, undergoing homeopathic treatment for any chronic disease within last 6 months, and simultaneous participation in any other clinical trial.
Interventions
The participants were randomized to verum (IHMPs plus concomitant care) or control (identical-looking placebos plus concomitant care) groups. IHMPs were prescribed according to homeopathic principles in centesimal potencies (6 cH, 30 cH, 200 cH, and 1000 cH) and individualized dosages. Each dose consisted of four globules (no. 40) of cane sugar, medicated with the indicated medicine on the centesimal scale (preserved in 90% v/v ethanol), instructed to be taken orally on a clean tongue with an empty stomach; dosage and repetition depending upon the individual requirement of the cases. Participants were advised to refrain from handling the globules or from eating, drinking, smoking, or brushing their teeth within 30 min of taking the globules and were asked to suck the globules rather than simply swallowing them. The follow-up period for each participant was 3 months. The participants were also instructed to avoid consuming coffee, mint, or any food or drink of a medicinal nature for the duration of the intervention.
The control group received placebo pills, identical in appearance to the verum, for 3 months. Each dose consisted of four globules (no. forty) of cane sugar, moistened with nonmedicinal rectified spirit, and was instructed to be taken orally on a clean tongue with an empty stomach; dosage and repetition depended upon the individual requirement of the cases and was similar to that of verum.
Irrespective of the allocated codes, all the randomized participants received standard advice on nonpharmacological management, that is, the patients were advised to continue COVID-19-appropriate behavior (using masks, hand, and respiratory hygiene), physical distancing, drinking adequate amounts of warm water (if not contraindicated), regular household work if health permitted, mild/moderate exercises like the daily practice of yoga asana, pranayama, meditation, and breathing exercises, daily morning or evening walk, balanced nutritious diet, having adequate sleep and rest, self-measurement of blood pressure and blood sugar (especially if hypertensive and diabetic), pulse oximetry (if medically advised) for dry cough or sore throat, saline gargling, and steam inhalations. 22 The duration of care was 3 months. All medicines and sundry items were procured from a Good Manufacturing Practice certified firm (Hahnemann Publishing Company Private Limited, Kolkata, West Bengal, India). The duration of therapy was 3 months. Both medicines and placebos were repacked in identical glass bottles and labeled with code, name of medicine, and potency and were dispensed according to a random number list. The coded bottles were accessible to the blinded pharmacist only, not to the participants. A single medicine was prescribed on each occasion, considering the presenting symptom totality, clinical history, constitutional features, and repertorization by appropriate repertories using HOMPATH ZOMEO 3.0® software when required. Materia medica was consulted and consensus was arrived at among three homeopaths for the final selection of the medicine and dosage. Provision was made to change the medicines or potencies and adjust the dosage in subsequent visits, in compliance with homeopathic principles. Several of the homeopaths possessed a Master’s degree in homeopathy, with more than 20 years of teaching experience and practicing classical homeopathy. The other prescribers were postgraduate trainees of the institution. All the homeopaths involved were affiliated with the state council. Compliance with the advice was assured by reminders to the participants in weekly phone calls and at every follow-up visit by the research assistants. Returned globules were counted to check the consumed dosage and were recorded in the drug accountability log.
Outcome measures
In this pilot trial, feasibility issues were examined, including recruitment, randomization, treatment, assessment of outcomes, follow-up, retention and attrition, the time needed to collect and analyze data, and shortlisting of the most frequently indicated medicines. The primary outcome measure was the postCOVID-19 symptoms checklist score, which was derived from the World Health Organization’s document on clinical case definition of post-COVID-19 condition 13 and from the international cohort study by Davis et al. (2021). 23 The secondary outcome measure was the Measure Yourself Medical Outcomes Profile version 2 (MYMOP-2)—suitable for patients who present with symptoms related to their physical, emotional, or social condition. It is patient-administered, problem-specific, and includes daily activity and general well-being at the same time. 24 It consists of “symptom 1” (domain 1), “symptom 2” (domain 2), “activity” (domain 3), and “well-being” (domain 4). It is also concerned with the “duration of suffering,” “history of previous medication,” and “any dependence on medicines” in the initial assessment. The follow-up part is concerned with “symptom 3,” which may have appeared in the meantime, and “any medication” for newly appeared symptoms. A noncommercial (academic) yearly license for using the MYMOP-2 questionnaire was obtained from Meaningful Measures® through email twice on September 28, 2021, and September 2, 2022.
Timeline
The outcome data were recorded at baseline and every month up to 3 months.
Sample size
In the absence of relevant published data and absence of the minimal clinically important difference (MCID) of the post-COVID-19 checklist score enabling formal sample size calculation, a medium effect size (Cohen’s d = 0.5) was assumed favoring IHMPs against placebos after 3 months of intervention. To detect a statistically significant difference between two independent means of post-COVID-19 symptoms checklist score using the unpaired t-test after 3 months of intervention, a trial with 128 (64 × 2) participants would have provided 80% power based on a two-sided significance level of 5%. Provision for a 10% attrition rate would further inflate the target sample size up to 140 (70 × 2). However, achieving such a large sample size seemed to be quite improbable in this project owing to time constraints and feasibility issues. Achieving a sample size of 60 (30 × 2) seemed probable and satisfactory for this trial. However, post hoc calculation revealed achieving 100% power, thereby providing ample opportunity to avoid a type 2 error.
Randomization
With a restriction of six permuted blocks of fixed size 10 and maintaining a 1:1 distribution between groups, an impartial third party used StatTrek random number generator (https://stattrek.com/statistics/random-number-generator.aspx; last accessed October 19, 2021) to centrally generate a list of 60 random numbers. Participants were thus divided evenly between the verum and control groups (1:1), thereby minimizing selection bias. The potential of the block randomization method to homogenize the data by removing unwanted variables and creating a uniform distribution of the important outcome-related parameters was another benefit. Once a participant was allocated to one code, it remained unaltered throughout the intervention of 3 months; thus, no cross-over was permissible. This random number table was supplied to the blinded pharmacist to distribute medication. Similar-looking amber-colored glass vials were categorized as “1” or “2” by another independent third party, denoting either identical-appearing drugs or placebos. Once the trial was over and the dataset was frozen, the codes were broken.
Blinding
The participants, treating physicians, pharmacists, outcome assessors, and data entry operators were all kept blind. By asking the participants which group they thought they were in, blinding was verified both before and throughout the study. After arriving at the final prescription, the case records were kept with the research assistants confidentially. The prescribed medicines were not disclosed to the participants, rather were written on a piece of paper, sealed inside an opaque envelope, and handed over to the blinded pharmacist who was responsible for dispensing the prescribed medicines from the coded vials and maintaining allocated codes following the random number chart.
Allocation concealment
The blinded postgraduate trainees and the registration counter staff screened, enrolled, and assigned serial numbers to the participants. To decide on a course of treatment, the blinded homeopaths interviewed the patients. Consequently, the random number sequence was kept a secret from the trial recruiters as well as the treating physicians to achieve allocation concealment.
Statistical methods
The intention-to-treat (ITT) approach was followed; every randomized patient was entered into the final analyses. Missing values were replaced by predicted values from a linear regression model. Data distribution was examined by histograms, Q-Q plots, and Shapiro–Wilk tests; no significant departure from normality was identified. Baseline confounders were presented using descriptive statistics. Group differences and intragroup changes were reported using descriptive statistics: means and 95% confidence intervals (CIs). The effect sizes were presented in terms of Cohen’s d (small effect, 0.2; medium effect, 0.5; large effect, 0.8). All statistical calculations were run using the Statistical Package for Social Sciences (version 20.0; IBM Crop., IBM SPSS Statistics for Windows, Armonk, NY, US, USA).
Adverse events
The participants were instructed to report any harm, serious adverse event, unintended effect, and unpleasant aggravations (homeopathic, medicinal, or disease symptoms), either over the phone or directly to the outpatients. These were treated with acute medicines (“rescue remedies”) dispensed in unblinded form.
Trial reporting
This trial was reported following the two guidelines—the recommendations for reporting data on homeopathic treatment (RedHot) and the CONSORT extension for pilot and feasibility trials were followed (Supplementary Appendix SA2-A3). 25–26
Results
Participant flow
A total of 175 patients were screened according to the prespecified inclusion and exclusion criteria. One hundred and fifteen were excluded for various reasons; 60 met the eligibility criteria and were enrolled subsequently. Baseline sociodemographic, laboratory parameters, and outcome data were obtained, and the patients were randomized to either IHMPs plus concomitant care (verum; n = 30) or identical-looking placebos plus concomitant care (control; n = 30). The outcome data were recorded at baseline and every month up to 3 months. During treatment, 3 dropped out and 57 completed the trial.
Recruitment
From the end of April 2022 until mid-July 2022, a total of 60 patients were enrolled in the trial. Follow-up of the last enrolled participant was completed by mid-October 2022.
Baseline data
The distribution of the sociodemographic factors, symptoms, and laboratory parameters has been presented in Tables 1-4.
Comparison of the Sociodemographic Characteristics and Symptoms Between Groups at Baseline (n = 60)
Continuous data presented as means ± standard deviations;
Categorical data presented as absolute values (percentages).
IHMPs, individualized homeopathic medicinal products.
Comparison of the Laboratory Parameters between Groups at Baseline (n = 60)
Continuous data presented as means ± standard deviations.
IHMPs, individualized homeopathic medicinal products.
Comparison of the Primary Outcome Measure Between Groups (n = 60)
CI: confidence interval; IHMPs, individualized homeopathic medicinal products; SD: standard deviation; SE: standard error.
Comparison of the Secondary Outcome Measure between Groups (n = 60)
CI, confidence interval; IHMPs, individualized homeopathic medicinal products; SD, standard deviation; SE, standard error.
Numbers analyzed
Outcomes from 29/30 participants in the IHMPs group and 28/30 participants in the placebo group were complete, respectively, the remainder dropped out of the trial. The data from 60 participants (IHMPs: n = 30; placebos: n = 30) were entered into the final analyses. Recruitment, retention, and attrition rates were 34.2%, 95%, and 5%, respectively. Retention rates in the verum and control groups were 96.7% and 93.3%, respectively (Fig. 1). Randomization, double blinding, outcome assessment, and follow-up, all proceeded without any challenges whatsoever. Reminders over the phone helped to ensure compliance.
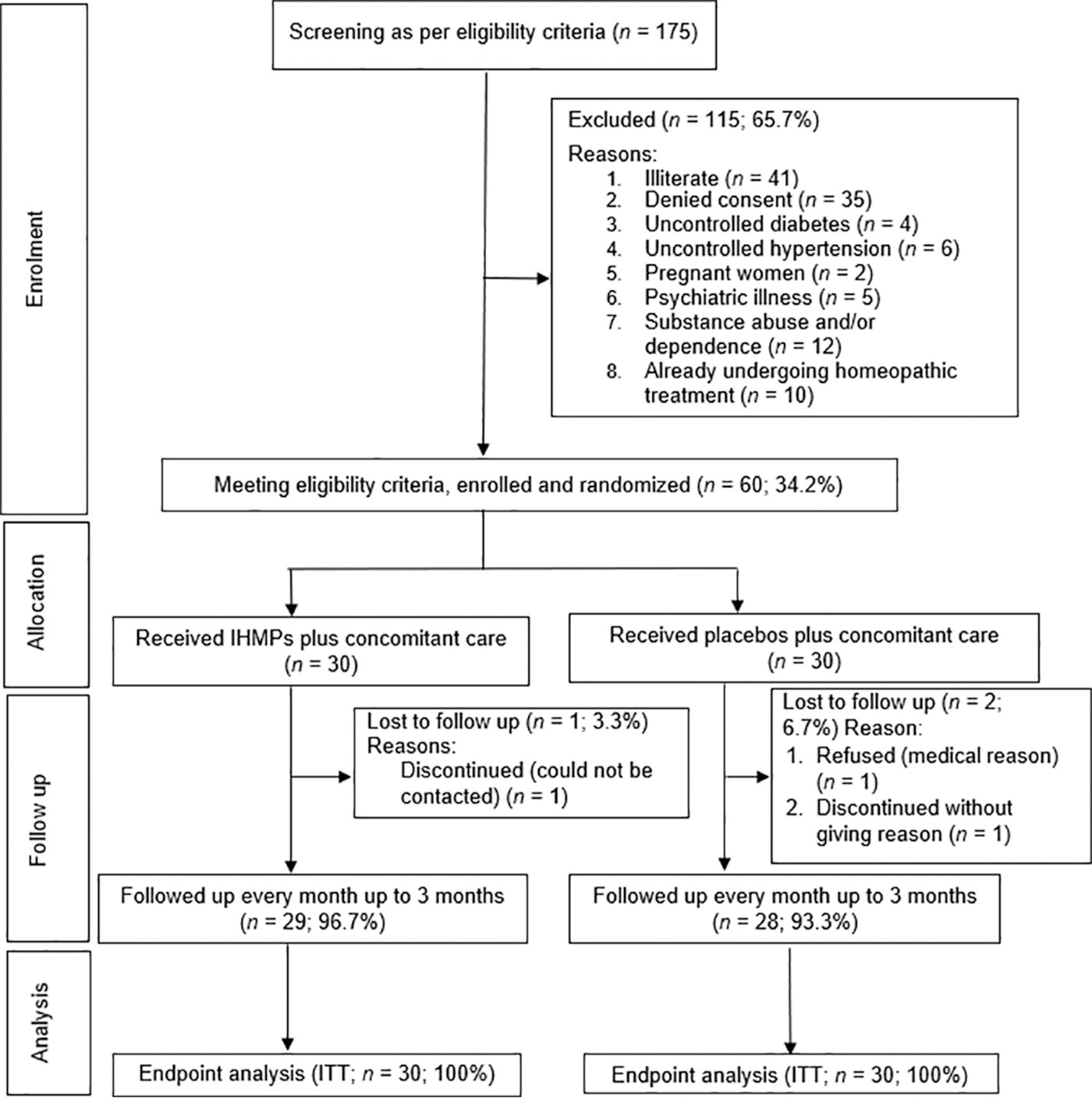
CONSORT study flow diagram.
Outcomes
PostCOVID-19 symptoms checklist score: After 3 months of intervention, the mean difference in postCOVID-19 symptoms checklist score between groups favored IHMPs against placebos; mean difference: −4.2, 95% CI −4.9 to −3.4, with large effect size (Cohen’s d: 2.854) (Table 3).
MYMOP-2 profile score: After 3 months of intervention, the mean differences in MYMOP-2 profile score between groups favored IHMPs against placebos; mean difference: −2.2, 95% CI −2.8 to −1.7, with a large effect size (Cohen’s d: 2.082). Similarly, all components of MYMOP-2, i.e., symptom 1, symptom 2, difficulty in activity, and feeling of well-being also demonstrated similar group differences favoring IHMPs over placebos after 3 months of intervention (Table 4).
Medicines used
Twenty-five different medicines were indicated at baseline in the two groups. Natrum muriaticum (n = 7, 11.7%), Pulsatilla nigricans (n = 6, 10%), Rhus toxicodendron (n = 5, 8.3%), Calcarea carbonica (n = 5, 8.3%), and Thuja occidentalis (n = 4, 6.7%) were the most frequently prescribed medicines (Table 5); majority of the potencies prescribed at baseline were 200cH (78.3%), followed by 30cH (15%) and 1000cH (6.7%). The indications of the most frequently prescribed remedies have been appended (Supplementary Appendix SA4). Change in medicines was required in 26.7% and 50% of cases in the verum and control groups, respectively.
Prescribed Medicines in the Two Groups at Baseline (n = 60)
IHMPs, individualized homeopathic medicinal products.
Adverse events
No serious adverse event was reported throughout the study. Four minor adverse events occurred in each verum and placebo group; however, all those seemed to be independent events rather than attributable to the interventions. In the verum group, four adverse events occurred—one event of injury from falling, one event of stoppage of nose, one event of bleeding per rectum, and another event of dry cough. All were treated successfully with homeopathic medicines—Arnica montana 200cH/4 doses, Rhus toxicodendron 30cH/6 doses, Nitricum acidum 30cH/1 dose, and Conium maculatum 30cH/4 doses, respectively. In the placebo group, four adverse events were recorded. One case of injury from falling was treated with Arnica montana 200cH/4 doses; one case of heavy menstrual bleeding was treated with Nux vomica 200cH/3 doses; one case of indigestion was treated with Lycopodium clavatum 200cH/2 doses; and one case of loose stool was treated with Aloe socotrina 30cH/6 doses. Once they recovered, they were returned to the previously allocated groups.
Discussion
This 3-month, double-blind, placebo-controlled, feasibility RCT on 60 participants with postCOVID-19 conditions demonstrated promising treatment effects of IHMPs against placebos in both the primary and secondary outcomes with large effect sizes after 3 months of intervention. Feasibility issues were examined and turned out to be promising. Natrum muriaticum and Pulsatilla nigricans were the most frequently prescribed medicines. Definitive trials are warranted to confirm the findings.
The obvious limitations include a feasibility design and the short duration of the trial. However, being an RCT, the methodological strengths of the study were built into its design—minimized selection bias, balancing of the two groups concerning the confounders, and formation of the basis of inferential statistical tests by ensuring comparability between groups at baseline. The advantages of blinding include minimized performance bias, ascertainment bias, and detection bias. Randomization was successful as was evident by the similar distribution of the confounder variables between groups. The treatment was in adherence to the state-of-the-art practices of classical homeopathy, based on individualization and totality of symptoms. Both the recruitment and retention rates of 34.2% and 95% were promising. The prescribed medicines in the trial reconfirmed those reported in the homeopathic literature. Several (unblinded) rescue remedies were used to treat acute (unrelated) situations. It appeared possible that this additional homeopathic treatment confounded the actions of the trial-specific medications. However, since they were “short-acting” medications chosen based on the “acute totality” of the situations, they performed on a different (superficial) level and were not expected to influence the way trial-specific medications acted. 27–28 The patients underwent re-evaluation by the treating physicians following the end of the acute phases. The doctors either administered new medications maintaining the assigned codes based on the patient’s symptomatology and as determined to be appropriate for the case or condition or they repeated the same trial medication of the same code. Higher instances of remedy changes were noticed in the IHMPs group than in the placebo. Remedy changes depend on multiple factors: perceived less pronounced effect of the medicines in the placebo group, no changes felt by the patient or a status quo after administering one medicine, new symptoms continue to appear, exhaustion of remedy action, disease or medicinal aggravation, and so on.
To provide a more thorough and dependable analysis, future research should focus on replications with larger sample sizes. The effects of IHMPs in LM potencies can also be evaluated. Longer study periods may provide additional information, but it is important to examine the ethical issues surrounding placebo-controlled trials. One potential outcome measure for future research is the Symptom Burden Questionnaire, which was created by Mapi Research Trust under the project “Advancing Understanding of Long COVID: Leveraging Patient Perspectives with the Symptom Burden Questionnaire.” 29
In an earlier double-blind RCT on 200 participants with postCOVID-19 fatigue by Rathi et al., a 14-day supplementation of ImmunoSEB plus ProbioSEB CSC3 resolved postCOVID-19 fatigue and improved patients’s functional status, and quality of life. 30 Treatment efficacy was compared using the Chalder Fatigue scale (CFQ-11). In comparison, this trial had a lesser number of participants and used a double-blind design, but extended for 3 months with positive results favoring the IHMPs over placebos. In an earlier single-blind RCT on 60 participants with post-COVID-19 fatigue in adults by Saha et al, a 3-month intervention with IHMPs produced statistically significant results over placebos in both the outcome measures. 17 In comparison, this trial had the same number of participants and used a double-blind design, but for 3 months, with postCOVID-19 conditions, and with positive results favoring the IHMPs over placebos. Another double-blind RCT on 100 participants with neuropsychiatric symptoms of post-COVID syndrome by Naeini et al., a 10-day intervention of fluvoxamine 100 mg tablet or a placebo daily orally. Fluvoxamine produced statistically significant results over placebos in primary outcome measures only. 31 In comparison, this trial had a lesser number of participants and used a double-blind design but extended for 3 months, with positive results favoring the IHMPs over placebos in both primary and secondary outcome measures. Another randomized, double-blind, placebo-controlled trial on 62 participants with post-acute-COVID-19 syndrome is ongoing comparing IHMPs with placebos having Fatigue Assessment Scale and SF-36 as the primary outcome and MYMOP2 as the secondary outcome (NCT05104749). 32 In a published case series of 9 patients with postCOVID-19 sequelae, eight got relief from Bryonia alba and one from sulfur. Some other medicines such as Arsenicum album, Rhus toxicodendron, and Calcarea carbonicum were prescribed as and when necessary. 33 The sample size was too small to arrive at any meaningful conclusion.
Conclusions
Sixty participants with postCOVID-19 conditions participated in a three-month, double-blind, feasibility RCT that compared IHMPs with identical-looking placebos. Trial feasibility issues revealed some encouraging results. The effects produced on both the primary and secondary outcomes by the IHMPs were seemingly better than placebos. Overall, IHMPs may have promising benefits against placebos, but these should be supported by definitive trials.
Footnotes
Acknowledgments
The authors are grateful to Dr. Amitava Paul, MD (Hom), Deputy Superintendent of the hospital for the smooth running of the trial. The authors acknowledge the kind help received from Dr. Krishna Basu Ray, MD, for clinical examination and diagnosis of all the enrolled participants of the trial. We sincerely thank fellow postgraduate trainees, staff, pharmacists, and patients for their sincere participation in the study.
Authors’ Contributions
A.R.: Conceptualization, methodology, validation, investigation, data curation, writing—original draft, review and editing, and project administration. P.B., S.G., S.S., S.N., S.G.: Conceptualization, methodology, validation, investigation, resources, data curation, writing—review and editing, supervision, and project administration. A.R.S.: Concept, methodology, and writing—review and editing. S.K.M.: Resources, supervision, project administration, and writing—review and editing. M.K., S.S.: Conceptualization, methodology, formal analysis, writing—original draft, review and editing, visualization, supervision, and project administration.
Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. The institution played no role in the analysis of the study results or the preparation of the paper.
Supplementary Material
Supplementary Appendix SA1
Supplementary Appendix SA2
Supplementary Appendix SA3
Supplementary Appendix SA4
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.