
Abstract
Background:
Long COVID is a serious, complex condition that has affected the lives of millions of people globally. Complementary and integrative health (CIH) approaches offer a wide range of potential therapies for the management of long COVID symptoms. However, there is limited information available about the utilization of CIH among long COVID patients.
Methods:
Nationally representative cross-sectional data from the United States 2022 National Health Interview Survey (NHIS, response rate 47.7%, n = 27,651) were used to investigate prevalence and predictors of CIH use in the past 12 months among individuals who experienced long COVID. The 12-month prevalence of CIH use was descriptively analyzed for those with long COVID versus those without using chi-squared tests or unpaired t-tests. Independent predictors of CIH use among individuals with long COVID were analyzed using a stepwise multiple logistic regression analysis.
Results:
A weighted total of 17,610,801 US adults (19.7%) who had a confirmed case of coronavirus disease 2019 (COVID-19) developed long COVID symptoms. A slightly greater proportion of individuals with long COVID (44.4%) than those without (40.9%) used CIH approaches in the past 12 months. The most used approaches were meditation, yoga, and massage therapy. CIH use by those with long COVID was significantly associated with younger age, female sex, higher education level, having health insurance coverage, higher household income level, receiving three or more COVID-19 vaccination doses, ever having asthma, and ever having an anxiety or depression diagnosis.
Conclusions:
Long COVID represents a major challenge for patients, health care providers, health care systems, economies, and global public health. CIH approaches may play an important role in symptom management for some patients, and additional research is needed to identify which modalities are most effective. Patients and health care providers may benefit from better information about the available options for treatment.
Introduction
Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), was declared a public health emergency of international concern by the World Health Organization (WHO) on January 30, 2020, and was characterized as a pandemic on March 11, 2020. 1 As of March 3, 2024, over 770 million confirmed cases of COVID-19 and over 7 million deaths worldwide had been reported to the WHO. 2 However, a vast number of cases and deaths have likely gone unreported. 3 –5 Survivors of COVID-19 are at risk for a variety of sequelae, a condition formally known as post COVID-19 condition, but commonly referred to as long COVID. 6 Long COVID is defined as the continuation of symptoms or the development of new symptoms 3 months after a SARS-CoV-2 infection, with symptoms lasting for at least 2 months that cannot be explained by an alternative diagnosis. 6 Studies indicate that at least 10% of individuals infected with SARS-CoV-2 will develop long COVID, 7 –10 and estimates of the prevalence of long COVID among adults in the United States (US) range from 6% to 18%. 11 –15 Potential risk factors for long COVID include acute COVID-19 severity, 16,17 age, 7,13,16,17 female sex, 7,8,17,18 race/ethnicity, 8,16,18 socioeconomic deprivation, 18 and a wide range of comorbidities. 16 –18
Long COVID can impact multiple major organ systems and more than 200 different symptoms have been identified. 7,8,18 Commonly reported symptoms include, but are not limited to, fatigue, difficulty breathing or shortness of breath, and cognitive dysfunction. 16,19,20 The cognitive impairments associated with long COVID can be debilitating, and deficits have been measured at the same magnitude as alcohol intoxication at the United States or United Kingdom legal driving limits or equivalent to 10 years of cognitive aging. 8,21 Long COVID patients also report high levels of functional impairment, mainly driven by fatigue levels, worse than in patients who had a stroke and comparable to patients with Parkinson’s disease. 22 As many as 50% of long COVID sufferers meet the criteria for myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). 8 A significant proportion of individuals with long COVID are unable to return to work, and long COVID presents a substantial burden to health care systems and economies. 8,23,24
The best way to prevent long COVID is to protect against SARS-CoV-2 infection through measures including COVID-19 vaccination, improving ventilation of indoor spaces, avoiding close contact with individuals with confirmed or suspected COVID-19 illness, and seeking early treatment for COVID-19 if eligible. 25 There is currently not a single, specific treatment for long COVID, and it is recommended that individuals experiencing long COVID should work with their health care provider(s) to develop a personal care plan. 25 Rehabilitation is a critical element of long COVID management, but it does not always lead to complete recovery. 26 In addition to traditional medical management, complementary and integrative health (CIH) approaches offer a wide range of potential therapies for the management of long COVID symptoms. Studies suggest that a variety of complementary therapies (e.g., transcutaneous auricular vagus nerve stimulation, meditation, dietary supplements, olfactory training, aromatherapy, etc.) might benefit patients with long COVID. 27 –30 Utilization of CIH approaches might also be an option for treating modifiable risk factors for certain comorbidities (e.g., cardiovascular disease 31 ) that increase the risk of developing long COVID.
Based on data from the 2022 National Health Interview Survey (NHIS), it has been estimated that approximately 40% of US adults use CIH approaches. 32 However, there is limited information available about the utilization of CIH approaches among long COVID patients. It has been reported that by 2029, the global complementary health industry is expected to quadruple in value, driven in part by rising demand for long COVID therapies. 33
Therefore, the primary aims of this study were to (i) estimate the prevalence of CIH approach utilization and (ii) analyze predictors of CIH approach utilization among US adults with long COVID in 2022.
Methods
Nationally representative cross-sectional data were obtained from the 2022 NHIS. The NHIS is a household interview survey conducted in-person and by telephone among the civilian noninstitutionalized population residing within the 50 states, and the District of Columbia. The response rate was 47.7% (n = 27,651) for adults (aged 18 years and over).
Outcome measures
The primary outcome measures were whether individuals ever had long COVID, and the use of CIH approaches in the past 12 months. Long COVID was assessed by the NHIS using the question “Did you have any symptoms lasting three months or longer that you did not have prior to having coronavirus or COVID-19?” Long COVID was only assessed for respondents who had ever had a symptomatic COVID-19 case confirmed by either their health care provider or by test. Therefore, there were missing data for many respondents (Table 1). Only respondents who answered “yes” or “no” to the survey question were included in this analysis (i.e., those who refused to respond, responded “don’t know,” or who did not a have a symptomatic COVID-19 case confirmed by health care provider or test [i.e., coded as missing] were excluded; n = 18,705).
Survey Response Options for the Question Assessing Long COVID in the 2022 NHIS
CIH use was defined as either seeing a chiropractor, practitioner of acupuncture, practitioner of massage, a naturopath, art therapist, and/or music therapist in the past 12 months; and/or having used mind–body approaches (mantra meditation, mindfulness meditation, spiritual meditation, guided imagery, progressive relaxation, and/or yoga) in the past 12 months.
Independent variables
Age, sex, race/ethnicity, and socioeconomic deprivation have been identified as risk factors for long COVID. 11,18 Additionally, a wide range of comorbidities have also been identified as potential risk factors for long COVID, including, but not limited to, asthma, hypertension, obesity, depression, and anxiety. 18,34,35 Meanwhile, age, sex, education level, geographic region, and household income level have commonly been reported as significant predictors of CIH use among various populations in the United States, including among older adults, 36 and among individuals with asthma, 37 hypertension, 31 stroke, 38 a history of colorectal cancer, 39 and multiple chronic conditions. 40 Therefore, self-reported data on sociodemographic characteristics including age, sex, race/ethnicity, region, education level, health insurance coverage status, and income level were included in the analysis, along with body mass index (BMI) category, asthma, cardiovascular disease, high cholesterol, prediabetes, type 2 diabetes, chronic obstructive pulmonary disease (COPD), cancer, chronic fatigue syndrome, anxiety, and depression were included in the analysis. Cardiovascular disease was defined as ever diagnosed with hypertension, stroke, myocardial infarction (i.e., heart attack), or coronary heart disease.
Statistical analysis
The overall prevalence of long COVID among individuals with a confirmed case of COVID-19 was calculated, and characteristics were compared between those with long COVID versus those without using chi-squared tests or unpaired t-tests, as appropriate (alpha level = 0.05). The 12-month prevalence of CIH use was calculated separately for individuals with long COVID and without long COVID. Additionally, the 12-month prevalence of consultations with a chiropractor, practitioner of acupuncture, massage therapist, and naturopath, and the use of each mind–body approach was calculated. Estimates were calculated using weights to account for complex survey design. The weighted estimates are representative for the noninstitutionalized civilian population of the United States rather than reflecting raw survey numbers.
Independent predictors of CIH approach used in the past 12 months among individuals with long COVID were analyzed using a stepwise multiple logistic regression analysis. Only those predictors associated with CIH use in univariate analysis at a p-value of ≤0.10 were considered. Furthermore, to address expected moderate multicollinearity, a correlation threshold of r = 0.6 was used to adjust the independent variables used in the multiple logistic regression analysis. Due to a high correlation between the anxiety and depression variables (r = 0.644), the two variables were recoded into a single “anxiety or depression diagnosis” variable. Adjusted odds ratios, confidence intervals, and p-values were calculated using relative weights (alpha level = 0.05). The Hosmer–Lemeshow test was used to assess model goodness-of-fit. Based on the format of the NHIS questions, those who refused to respond, responded “don’t know,” or didn’t answer all of the relevant survey questions used for this study were excluded from the multiple logistic regression analysis (n = 90). Analyses were conducted in SAS Studio.
Results
A weighted total of 17,610,801 US adults (19.7%) who had a confirmed case of COVID-19 ever developed long COVID symptoms. Adults who experienced long COVID differed from individuals without long COVID on certain sociodemographic characteristics, including age, sex, race/ethnicity, family income level, COVID-19 vaccination doses, COVID-19 symptom severity, and selected comorbidities (Table 2). Specifically, long COVID was associated with slightly higher age, female sex, Hispanic ethnicity, lower household income level, fewer COVID-19 vaccination doses, severe COVID-19 symptoms, obesity, and with each comorbidity assessed.
Comparison of Characteristics of Adults with and without Long COVID following a Confirmed Case of COVID-19 a
p-values are derived from unpaired t-tests and chi-square tests, as appropriate, using relative weights; statistically significant p-values are shown in bold.
Weighted frequencies or means are reported and are representative of the civilian, noninstitutionalized population of the United States.
More adults without long COVID (weighted n = 29,403,908; 40.9%) used CIH approaches in the past 12 months than adults with long COVID (weighted n = 7,814,005; 44.4%). However, a greater proportion of individuals with long COVID than those without used each of the CIH approaches assessed, except for yoga (Fig. 1). The most frequently used CIH approaches for individuals with long COVID were meditation (22.3%) and yoga (17.2%), followed by massage therapy (15.4%), chiropractic care (13.8%), and guided imagery or progressive relaxation (10.2%).
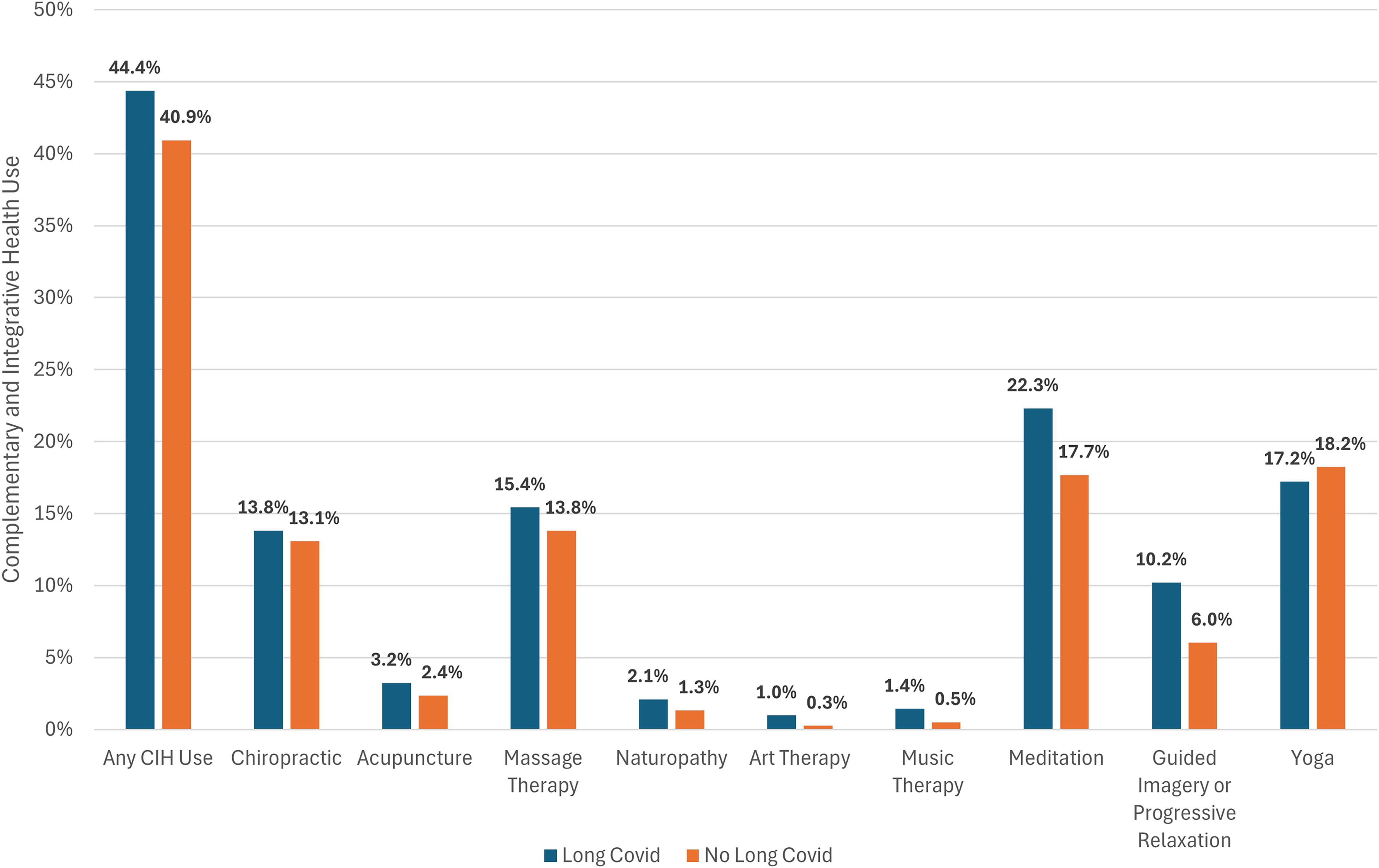
Twelve-month prevalence of CIH use among adults with and without long COVID. Weighted frequencies were used.
In both univariate analysis (Table 3) and multivariate logistic regression analysis (Table 4), CIH use in adults who experienced long COVID was significantly associated with younger age, female sex, higher education level, having health insurance coverage, higher household income level, receiving three or more COVID-19 vaccination doses, ever having asthma, and ever having an anxiety or depressive disorder diagnosis. By contrast, individuals with long COVID who had ever been diagnosed with a cardiovascular disease, high cholesterol, and type 2 diabetes were significantly less likely to utilize CIH approaches. Although not significantly associated with CIH use among individuals with long COVID in univariate analysis, race/ethnicity and BMI category were both significant predictors of CIH use in the multivariate logistic regression analysis. Specifically, non-White individuals were significantly more likely to use CIH approaches than individuals identifying as White, and individuals who were underweight, overweight, or obese were significantly less likely to use CIH approaches than individuals of normal weight. The Hosmer–Lemeshow goodness-of-fit test statistic was not significant (χ 2 = 4.791, df = 8, p = 0.780), suggesting adequate model fit.
Comparison of Characteristics of Adults with Long COVID Using or Not Using CIH Approaches a
p-values are derived from unpaired t-tests and chi-square tests, as appropriate, using relative weights; statistically significant p-values are shown in bold.
Weighted frequencies or means are reported and are representative of the civilian, noninstitutionalized population of the United States.
Individual Predictors of CIH Approach Use in Adults with Long COVID
p-values derived from logistic regression analysis using relative weights.
Discussion
The estimated prevalence of long COVID among the total US adult population based on the 2022 NHIS was 6.9%, as previously reported by Adjaye-Gbewonyo et al. 12 However, this is likely an underestimate because it doesn’t account for individuals who experienced long COVID but never had the precipitating COVID-19 infection confirmed by a health care provider or test. The estimated prevalence of long COVID among US adults who ever had COVID-19 based on the 2022 NHIS was 19.7%. The prevalence estimates derived from the 2022 NHIS were in line with estimates derived from the 2022 Behavioral Risk Factor Surveillance Survey (BRFSS), 14 but were substantially lower than estimates from the National Center for Health Statistics’ experimental, online Household Pulse Survey. Specifically, it was estimated that, as of December 2022, 14.4% of US adults had ever experienced long COVID, whereas 28.1% of adults who had ever had COVID-19 experienced long COVID. 15
CIH approaches were used by 44.4% of noninstitutionalized, civilian US adults who ever experienced long COVID. This was slightly higher than the estimated prevalence of CIH use by US adults who had not experienced long COVID (40.9%) but lower than the estimated prevalence of CIH use globally among patients with COVID-19 during the height of the pandemic (0.65, 95% confidence interval = 0.48–0.81). 41
The most frequently used CIH approaches for individuals with long COVID were meditation (22.3%), yoga (17.2%), massage therapy (15.4%), chiropractic care (13.8%), and guided imagery or progressive relaxation (10.2%). However, while the NHIS data indicate which CIH approaches individuals used, they don’t specify whether individuals were specifically using the approaches to manage long COVID symptoms. In addition, it is possible that the use of certain provider-based therapies, such as massage therapy or chiropractic care, may have decreased in the aftermath of the pandemic. Some individuals may have chosen to continue to isolate or maintain social distancing practices during the study period, which could have resulted in decreased use of CIH approaches that require in-person interaction.
Although few studies have assessed the use of meditation for the management of long COVID, meditation appears to be a promising nonpharmacological approach for the treatment of certain long COVID symptoms. A recent review study reported that long COVID patients might be able to achieve improvements in symptoms and underlying pathology through meditation. 42 Additionally, the results of a randomized controlled trial indicated that a 4-week neuromeditation program reduced cognitive impairment, fatigue, muscle and joint pain, mental health symptoms, and improved sleep quality in long COVID patients. 43
Similarly, other mind–body therapies (e.g., yoga, tai chi, qigong, etc.) could potentially help to manage certain long COVID symptoms, including cognitive impairment, mental health symptoms, fatigue, shortness of breath, and sleep disturbances. 44 –46 In particular, deep breathing exercises, such as pranayama [yogic breathing techniques] completed as part of a yoga practice, may help to reduce or eliminate dyspnea and improve mental health symptoms associated with long COVID. 44,45,47,48 Yoga has already been incorporated into rehabilitation programs for adults with long COVID. 49 However, yoga was the only CIH approach that had lower utilization among individuals with long COVID (17.2%) than those without (18.2%) in this study. This may be because yoga, unlike the other approaches assessed, includes a physical activity component, which might be a limitation of use for some individuals given that long COVID can cause pain and fatigue. However, there is evidence that yoga can help to manage both pain and fatigue in patients with CFS, 50 as well as in other patient populations. 51 –55 Therefore, the accessibility of appropriate yoga practices for individuals with long COVID should be explored further in future research.
With regard to manual therapies, a systematic review reported that massage therapy has provided benefits to patients experiencing symptoms similar to those for long COVID. 56 Therefore, targeted massage therapy might support the management of certain symptoms, including muscular and joint pain, fatigue, respiratory, mental health, and gastrointestinal symptoms in long COVID patients. 56 However, there remains a lack of direct clinical evidence for the application of massage therapy for the treatment of long COVID. It is possible that long COVID patients may seek chiropractic care for the alleviation of joint and muscle pain, but studies assessing the use of chiropractic care in relation to long COVID were not identified. It is also possible that NHIS participants who reported the use of CIH approaches were seeking care for complaints unrelated to long COVID.
A recent article by Bilc and Holger 57 also examined the use of CIH approaches among US adults with long COVID using data from the 2022 NHIS. This study shares some similarities to the one conducted by Bilc and Holger, but an important distinction is that different sets of independent variables were used in the multivariate logistic regression models developed by each study. For example, this study incorporated a wide range of comorbidities that have been identified as potential risk factors for long COVID, while Bilc and Holger (2024) only included general health status. Additionally, Bilc and Holger developed separate models for each CIH modality and any CIH use, while this study focused solely on any CIH use. Taken together, these studies provide valuable insights into CIH use among US adults with long COVID.
This study indicated that use of CIH approaches in the past 12 months among individuals who experienced long COVID was significantly associated with younger age, female sex, higher education level, having health insurance coverage, and higher household income level, consistent with earlier reports on the characteristics of US adults who use CIH approaches. 58 –60
CIH approach use was also significantly associated with receiving three or more COVID-19 vaccination doses. Varied associations between CIH use and vaccination behavior have previously been reported. It has been suggested that complementary medicine lends support to the antivaccination movement because some providers have a negative attitude toward vaccination. 61 –63 However, findings from the 2002 NHIS showed that US adults who used CIH approaches had significantly higher vaccination coverage levels than non-CIH users for influenza and pneumococcal vaccines. 64 More recently, findings from the 2017 NHIS indicated that overall CIH users were as likely as nonusers to have received an influenza vaccination in the past 12 months, although individuals who consulted with naturopaths, homeopaths, and chiropractors were less likely to have received an influenza vaccination. 65 Future research should examine the relationship between COVID-19 vaccination coverage and the use of different CIH therapies among long COVID survivors to elucidate potential associations.
The use of CIH approaches in the past 12 months among individuals who experienced long COVID was also significantly associated with ever having asthma, and ever having an anxiety or depressive disorder diagnosis. Previous studies have reported relatively high prevalence of CIH use among adults with asthma (e.g., 20–40%), 37,66 anxiety (e.g., 28–57%), 67,68 and depression (e.g., 20–54%). 67,68 It is perhaps not surprising that asthma was an important comorbidity in this study. Retrospective cohort studies have indicated that individuals with asthma are at an increased risk of developing long COVID. 69,70 Furthermore, it may be difficult to distinguish long COVID from asthma due to overlapping symptoms (e.g., dyspnea). 71 Similarly, a prospective cohort study reported that having a prior diagnosis of anxiety or depression may increase the risk of developing long COVID, 72 and anxiety and depression may develop after infection with SARS-CoV-2, possibly due to distressing long COVID symptoms. 73 –75 Overall, the evidence points to complex relationships between long COVID and these comorbidities, and concerns about these conditions alongside long COVID may drive individuals to seek CIH care.
Individuals with long COVID who had ever been diagnosed with cardiovascular disease, high cholesterol, and type 2 diabetes were significantly less likely to utilize CIH approaches. A possible reason for lower utilization of CIH approaches among individuals with cardiovascular disease or type 2 diabetes is that these individuals may suffer from physical dysfunction related to these diseases and their sequelae that complicates their access to various CIH therapies. Unfortunately, the NHIS does not collect information on the specific reasons that individuals do or do not use CIH approaches. Furthermore, due to the use of cross-sectional data in this study, it is not known whether individuals experienced long COVID and comorbidities concurrently or sequentially.
Another major limitation of this study is that only a small selection of CIH approaches were included in the NHIS (e.g., Ayurveda, Chinese herbal medicine, and other approaches were not included). Additionally, the NHIS relies on self-reported data and, therefore, these study results are subject to potential recall bias. Additionally, the NHIS only captures data for the noninstitutionalized, civilian US population, excluding individuals in hospitals, nursing homes, long-term rehabilitation, or prison facilities. Active-duty Armed Forces personnel were also not captured in the NHIS data. These populations, some of them quite vulnerable, merit further study to assess the prevalence of long COVID and to consider therapy options and availability.
Overall, this research indicates the widespread use of CIH approaches among individuals who experienced long COVID. However, additional information is needed to understand whether individuals are specifically using CIH approaches to address long COVID symptoms, and if so, which symptoms individuals are seeking to address through different CIH modalities. To that end, it would be useful to directly survey the population who have experienced long COVID to obtain more detailed information about their CIH use. Clarifying these health-seeking behaviors among long COVID sufferers may help to indicate where there is high or unmet need for long COVID rehabilitation and recovery. Long COVID interventions will likely benefit from multidisciplinary approaches to address the numerous symptoms associated with the condition.
Conclusion
It was estimated that 44% of US adults who had experienced long COVID used CIH approaches in the past 12 months. The most frequently used CIH approaches were meditation, yoga, and massage therapy. Utilization was more common among adults who were younger, female, had a higher education level, had health insurance coverage, had a higher household income level, received three or more COVID-19 vaccination doses, ever had asthma, and ever had an anxiety or depressive disorder diagnosis. Long COVID represents a major challenge for patients, health care providers, health care systems, economies, and global public health. CIH approaches may play an important role in symptom management for some patients, and additional research is needed to identify which modalities are most effective. Patients and health care providers may benefit from better information about the available options for treatment.
Footnotes
Acknowledgments
The author would like to thank Drs. James Whedon and Steffany Moonaz for providing feedback on this article.
Authors’ Contributions
L.G.: Completed article drafting, study conception and design, and data collection and analysis.
Ethics Approval and Consent to Participate
NCHS Research Ethics Review Board approved NHIS data collection (Protocol #2019–09). All participants provided informed consent to participate. An additional ethical approval for performing this research was not required.
Availability of Data and Materials
Author Disclosure Statement
The author declares that there are no conflicts of interest.
Funding Information
This research received no specific funding.