
Abstract
Our primary objective in this study was to determine the differences in inflammatory profile between patients with high risk for obstructive sleep apnea (OSA) versus low risk in a patient population undergoing cardiac rehabilitation and to evaluate the effect of 4 weeks of rehabilitation on cytokine levels in the 2 groups. A total of 20 consecutive patients were screened using the Berlin questionnaire to determine high and low risk of OSA. Of the 20 total consecutive patients, 3 patients did not consent to participate and 1 did not get cytokine analysis. Of the remaining 16 patients (8 men and 8 women), 8 (50%) patients were found to have high risk for OSA as predicted by the Berlin questionnaire. Men predominated the high-risk group (75%). There was a trend of increased cytokine load in the high-risk group; however, it did not reach statistical significance except for monocyte chemoattractant protein-1 (P value=0.02). A significant reduction was noted in cytokine levels after 4 weeks of rehabilitation in the group with OSA, which was statistically significant (P value<0.5). The high-risk group patients had elevated cytokine levels, especially monocyte chemoattractant protein-1. Further, a significant reduction in cytokine levels was noted in the high-risk group after 4 weeks of rehabilitation.
Introduction
P
Mooe and others found in a prospective cohort study that patients with an AHI of ≥10 had a 62% relative increase and a 10.1% absolute increase in the composite endpoint defined as death, cardiovascular accidents, and myocardial infarction (Mooe and others 2001). Treatment of OSA with continuous positive airway pressure (CPAP) over a 5-year period in patients with known CAD resulted in significant decrease in occurrences of new cardiovascular events—24% in treated versus 58% in nontreated patients (Milleron and others 2004). Similarly, many other cardiovascular diseases such as hypertension, congestive heart failure, and atrial fibrillation have a high incidence of sleep-disordered breathing (Pepperell and others 2002; Gami AS and others 2004; Javaheri 2006), and many patients with debilitating heart diseases or postcardiac bypass surgery undergo cardiac rehabilitation. We have previously reported a high prevalence (40%) of undetected OSA as measured using the Berlin questionnaire in a population undergoing cardiac rehabilitation (Sharma and Parker 2010).
Inflammatory markers including cytokines have been found to be elevated in patients with atherosclerosis and shown to be markers of cardiovascular complications (Teramoto and others 2003).
Clinical data also strongly suggest that cytokines and inflammatory markers are significantly raised in patients with OSA and obesity (Yokoe and others 2003). However, some markers such as interleukin-6 (IL-6) (Shamsuzzaman and others 2002) have been shown to be elevated more in patients with OSA than in obese subjects (Vgontzas and others 2002; Ohga E and others 2003), suggesting that OSA may be an independent risk factor for increased inflammation.
Further, it has been shown that treatment with positive airway pressure significantly decreases the levels of IL-6 (Yokoe and others 2003). IL-6 and TNF-a are associated with levels of high-sensitivity C-reactive protein (hs-CRP), which in turn is a robust marker of cardiovascular complications (Yokoe and others 2003). Data on cytokines support the notion that these inflammatory markers and cytokines accelerate the progression of atherosclerosis. Conceivably, the inflammation caused by OSA, as mentioned earlier, may further add fuel to the fire. It is not clear whether rehabilitation can reduce the cytokines generated by OSA.
Cardiac rehabilitation provides a great opportunity to further study this phenomenon as patients have advanced heart diseases and high incidence of OSA (Sharma and Parker 2010). Patients undergoing cardiac rehabilitation, having suffered a major cardiovascular event, may also be a more motivated population. Hence, we believe that acceptance and compliance in this high-risk population would be better, thereby positively impacting the natural history of the disease. In this study, we look at those cytokines that are elevated in patients with high risk of OSA compared with low risk in patients undergoing cardiac rehabilitation. Further, we look at the impact of 4 weeks of cardiac rehabilitation on inflammatory markers in these 2 groups.
The hypothesis of this study was that inflammatory markers are more elevated in patients with CAD and OSA when compared with patients with CAD without OSA in those undergoing cardiac rehabilitation. As previous studies in patients with CAD have shown reduction of proinflammatory cytokines with exercise, we also investigated whether this holds true for patients with high risk of OSA in absence of continuous positive pressure (CPAP) therapy.
Study Design
Patients initiating cardiac rehabilitation at an academic hospital were asked to participate in this study. Inclusion criteria for the study consisted of patients initiating a cardiac rehabilitation program. We anticipated that subjects involved in this study would not carry any additional risk because of the study protocol. Exclusion criteria included patients actively receiving CPAP treatment for the treatment of OSA or actively undergoing cardiac rehabilitation (patients who had already started rehabilitation sessions). Blood samples were taken in the morning of the first day of rehabilitation session and again after 4 weeks of cardiac rehabilitation. No major risks were anticipated except those from blood draw (ie, pain, bleeding, thrombophlebitis).
The study protocol was approved by the Palmetto Richland Hospital Institutional Review Board. The patients were referred mostly by cardiologists, and indication for referral to cardiac rehabilitation in our patient population included postcoronary artery bypass graft, postmyocardial infarction, and angina.
Twenty consecutive series of patients initiating cardiac rehabilitation from June 2007 to September 2007 were consented by the principal investigator and study coordinator(s) and assessed for risk of OSA using the Berlin questionnaire. A total of 18 patients were found to meet the criteria, of which 3 patients refused to participate in the study. One patient did not follow up for repeat cytokine analysis. The final number of patients analyzed was 16.
The Berlin questionnaire is a simple, 1-page questionnaire designed as a prediction tool for OSA. The Berlin questionnaire consists of 3 categories of questions. Category 1 deals with the presence and intensity of snoring. Category 2 gauges the degree of daytime sleepiness, whereas category 3 determines presence of hypertension or BMI over 30 kg/m2. Category 1 tries to determine the intensity of snoring by grading it between slightly louder than breathing to very loud, which can be heard in the next room. It further grades snoring on the basis of frequency (ie, never to every day), and whether the snoring bothers other people (yes/no) and has anyone noticed the patient quitting breathing and how often. Category 2 has 4 set of questions: (1) how often does the patient feel tired after waking up, (2) how often the patient feels tired during the day, (3) has the patient fallen asleep behind the wheels, and (4) if yes, how often. Categories 1 and 2 are considered positive if 2 or more questions are answered as yes and frequency is more than 3–4 times a week. Category 3 is considered positive if the patient has hypertension and/or BMI of 30 kg/m2. The patient is determined to be at high risk if 2 or more categories score positive.
The Berlin questionnaire has a positive predictive value of 85% and a negative predictive value of 94% for severe OSA (Mooe and others 2001). That is, the Berlin questionnaire is 85% accurate in assessing the risk of patients with OSA and 94% accurate in assessing the presence of OSA in patients who have severe OSA (Netzer and others 1999).
The patients were divided into 2 groups as high risk and low risk for OSA. Both groups underwent cytokine profiling by 27 human Plex cytokine analysis systems before entering rehabilitation. After 4 weeks of cardiac rehabilitation, both groups underwent repeat cytokine profiling. Differences in both groups before and after cardiac rehabilitation were investigated. Inclusion criteria involved that all patients are starting cardiac rehabilitation and willing to participate by signing an informed consent.
Data analysis
As part of the protocol, physicians of the patients with a positive Berlin questionnaire were notified of these findings. As a result of clinical determination by their primary physician, 15 patients underwent an overnight polysomnography to determine the presence of OSA. Thirteen of these patients were found to have OSA (86%).
It was expected that 8 (40%) will be OSA subjects, based on previous data. The power to detect a difference between OSA subjects and the others will depend on the actual difference between the 2 groups' cytokine levels and on the common standard deviation for each cytokine being tested. The effect size (which is the difference between the means divided by the standard deviation) detected with the indicated sample sizes is 1.35; testing was at the 0.05 level and power of 0.80.
A t-test was used to assess for cytokine differences. As this is a pilot study, the initial testing was considered as exploratory in the sense of seeking to find those markers that are differentially expressed between OSA and non-OSA patients.
Results
A total of 20 consecutive patients were invited to the study. Three patients refused to participate and 1 patient did not get cytokine analysis and was not included in the final analysis. Of the remaining 16 patients, the baseline characteristics of low- and high-risk OSA are shown in Table 1. The patients with high risk for OSA tended to be younger (mean age: 65) compared with the low-risk group (mean age: 78). The high-risk group also had higher percentage of males (75%). The following cytokines were detected in sufficient levels for further analysis: IL-2, IL-4, IL-8, interferon gamma (IFN-g), IL-13, and monocyte chemoattractant protein-1 (MCP-1).
OSA, obstructive sleep apnea.
There was a trend toward increased cytokine load in the group with OSA; however, it did not reach statistical significance except for MCP-1 (P value=0.02) (Fig. 1a, b).
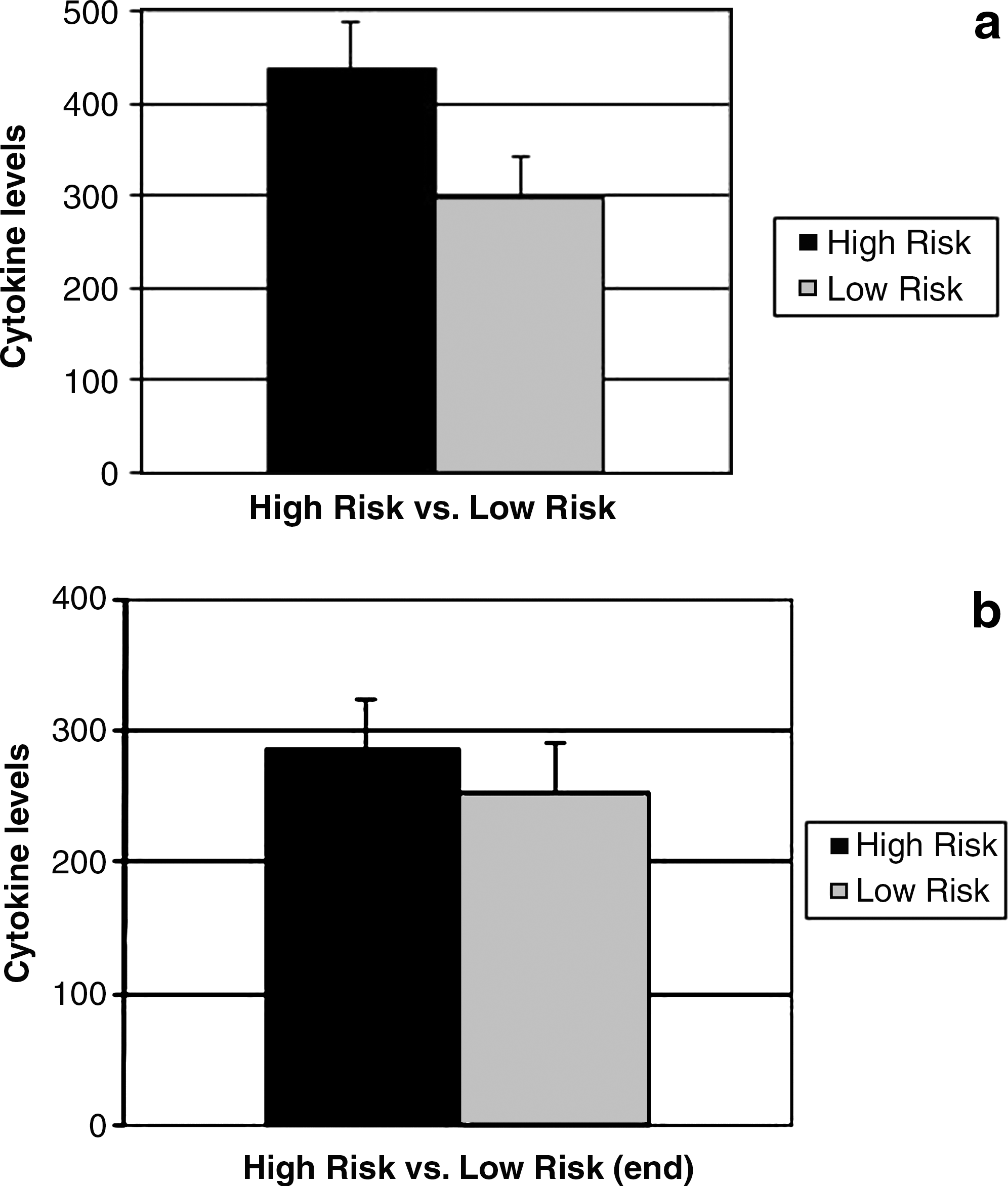
A significant reduction was noted in cytokine levels after 4 weeks of rehabilitation in the group with OSA, which was statistically significant (P value<0.05) (Table 2).
IL, interleukin.
The results also suggest overactivation of proinflammatory TH1 cytokines with increased TH1/TH2 ratio in the patients with high risk for OSA (Table 3).
Discussion
As far as we know, this is the first pilot study that looks at the impact of rehabilitation on cytokines in the patients with or without high risk of OSA undergoing cardiac rehabilitation.
Our study finds increased levels of cytokines in the OSA group, with MCP-1 levels significantly higher (P=0.02) and other cytokines showing trends toward higher level.
The cytokines detected were mostly proinflammatory, revealing an increase in TH1/TH2 ratio.
We also found significant reduction in the cytokine levels (P<0.05) after 4 weeks of cardiac rehabilitation. Cytokine levels after 4 weeks of cardiac rehabilitation were higher in the high-risk OSA group, although they did not reach statistical significance.
We found detectable and elevated levels of IL-2, IL-4, IL-6, IL-8, IL-13, IFN-g, and MCP-1.
Inflammation is an important factor in the pathogenesis of atherosclerosis. OSA has been shown to increase the levels of inflammatory markers. Treatment of OSA has been shown to result in lowering of the levels of cytokines.
Our study found elevated cytokine levels during the beginning of rehabilitation in both high-risk OSA and non-OSA groups, although there was a trend of higher cytokine load in the OSA group. Both groups demonstrated a reduction in inflammatory load after 4 weeks of rehabilitation. This is consistent with a prior study that has revealed that exercise in CAD patients is an effective way of inducing reduction in proinflammatory markers (Goldhammer and others 2005). A similar trend was seen in our study in both groups; however, the OSA group continued to show a higher inflammatory load than the non-OSA group, although statistical significance was not reached. We postulate that the higher inflammatory load in the OSA group may be due to unresolved OSA.
Growing evidence suggests that regular exercise induces an anti-inflammatory state (Petersen and Pedersen 2005), but the mechanism is poorly understood. It has been postulated that the anti-inflammatory effects of exercise may be due to cytokine modulation and possibly compensatory enhancement of anti-inflammatory mechanism, including shifting of the balance to TH2-derived cytokines (Kadoglou and others 2007). It has also been shown that IL release by adipose tissue due to sympathetic stimulation is attenuated by physical activity and may contribute to the anti-inflammatory effects (Freemantle and others 1997; Mohamed-Ali and others 2000).
As BMI may have an effect on cytokine levels, we limited the study to 4 weeks.
It is interesting to note that MCP-1 was significantly elevated in the high-risk group undergoing cardiac rehabilitation.
MCP-1 appears to be responsible for the direct migration of monocytes into the intima at sites of atherosclerotic lesion (Boring and others 1998; Gu and others 1998).
MCP-1 has been implicated as a key player in the development of intimal hyperplasia after angioplasty as well as in vasculogenesis and thrombosis (Charo and Taubman 2004).
Intimal hyperplasia is an important component of the atherosclerotic plaque and is thought to be critical to the development of restenosis after coronary artery angioplasty and stent placement (Ross 1995).
The response to arterial injury appears to be mediated by MCP-1 and CCR2. Antibodies to MCP-1 attenuate intimal hyperplasia in a rat model of carotid artery injury (Furukawa and others 1999). A CCR2 (functional receptor of MCP-1) blocking antibody has been shown to provide significant protection against in-stent stenosis (Horvath and others 2002). Braunwald and others looked into the role of MCP-1 in the patients with ischemic heart disease. Their study revealed that the patients with coronary heart disease and high level of MCP-1 had significantly greater risk of death or myocardial infarction over a 10-month follow-up period (de Lemos and others 2003).
IL-8, another chemokine and a neutrophilic chemoattractant, also activates monocytes and may direct their recruitment to vascular lesions (Gerszten and others 1999). It has been found in macrophage-rich atherosclerotic plaques. Animal studies have shown that mice lacking the IL-8 receptor had less accumulation of macrophages and smaller atherosclerotic lesions (Boisvert and others 1998).
T cells likewise encounter signals that cause them to elaborate inflammatory cytokines such as γ-interferon and lymphotoxin (tumor necrosis factor [TNF]-β), which in turn can stimulate macrophages as well as vascular endothelial cells (Hansson and Libby 1996).
The Th1/Th2 balance is critically skewed, one way or the other, in several diseases, such as acute and chronic infections, autoimmunity, and atopy/allergy (Fearon and Locksley 1996; Mosmann and Sad 1996; Elenkov and Chrousos 1999).
The type of immune reaction that would be triggered, that is, Th1 predominant (cell mediated) or TH2 (antibody mediated), depends on the type of cytokines involved. Certain cytokines are triggered depending on the type of insult inflicted. Many noninfectious diseases are now believed to be mediated by specialized cytokine responses. In our study, the majority of the cytokines detected and elevated in the OSA group were TH1 inducers (IL-2, IFN-g, IL-8, and MCP-1). IL-4 and IL13 are TH2 inducers; however, the levels of IL13 were higher in the low-risk group (see table 3). This suggests that OSA appears to be a predominant TH1-related disease process (proinflammatory).
It is interesting to note that IL-13, an anti-inflammatory cytokine, was higher in the non-OSA group but reduced in both groups after exercise even though it remained higher in the low-risk group. We would expect this to get elevated after exercise intervention. However, past studies showing elevation in anti-inflammatory markers were done with longer durations of exercise.
We acknowledge that this study had a small sample size. Screening for high- and low-risk patients was based on the Berlin questionnaire. The Berlin questionnaire is 85% accurate in assessing the risk of patients with OSA and 94% accurate in assessing the presence of OSA in patients who have severe OSA. The subsequent evaluation of a sample of our population with positive Berlin questionnaire who underwent overnight polysomnography revealed that 13 of 15 (86%) patients had OSA.
All of the 27 cytokines were not observed, which may be due to their levels being either too low or too high. Certain cytokines may have a circadian rhythm, which may partially explain the inability to detect some cytokines because blood samples were drawn early in the morning before start of exercise session. Baseline characteristics reveal increased cardiovascular disease in the low-risk category, but the numbers are small and differences are not significant. Even if these differences were significant it would further highlight the point that OSA is a powerful driver of inflammation despite more disease burden in the low-risk category.
In conclusion, our study suggests that the patients entering cardiac rehabilitation with high risk for OSA have a higher inflammatory burden compared with the low-risk group. Cardiac rehabilitation reduces this inflammatory burden in the patients with OSA.
Our study provides insight into the interaction of exercise, OSA, and cytokines. Larger studies to support the above findings and evaluate the effect of CPAP therapy on inflammatory burden in cardiac rehabilitation are needed.
Footnotes
Author Disclosure Statement
No competing financial interests exist.