
Abstract
Macrophage migration inhibitory factor (MIF) plays a pivotal role in pregnancy-related proinflammatory processes, such as placentation and labor. Differential MIF concentrations have been correlated with pathological events during pregnancy, such as recurrent miscarriages and severe pre-eclampsia (PE). The aim of this study was to prospectively investigate whether maternal MIF serum levels are already altered in early pregnancy before PE onset. Women (n=2,821) before 20 weeks of gestational age were recruited for a prospective study on early markers of PE. Forty-eight consecutive pregnancies that developed PE and 79 normotensive pregnancies that delivered at term were chosen. Maternal MIF serum levels were assessed by ELISA. We found significantly lower MIF serum levels in women who developed PE (4,967±3,119 pg/mL) compared to controls (7,640±5,519 pg/mL) (mean±standard deviation, P<0.001). Our findings indicate that low maternal MIF serum levels in early pregnancy may contribute to abnormal placental development.
Introduction
P
The macrophage migration inhibitory factor (MIF) is a key regulator of inflammatory and immune responses (Bernhagen and others 1993; Calandra and Roger 2003). MIF is an important counter-regulator of glucocorticoid action that reverses glucocorticoid-induced immunosuppression and, in particular, glucocorticoid-induced proinflammatory cytokine inhibition (Calandra and others 1995). For its intrinsic inflammatory properties, MIF is highly involved in the pathogenesis of numerous acute and chronic inflammatory diseases in both mice and humans (Grieb and others 2010).
MIF is present in human serum at concentrations ranging from 2,000 to 6,000 pg/mL (Calandra and others 1994, 2000) and from 5,000 to 15,000 pg/mL in pregnancy (Ietta and others 2002; Hristoskova and others 2006). Although the major source of human plasma MIF is unclear, MIF is expressed by several cell types, including endothelial cells (Simons and others 2011), macrophages, T and B lymphocytes (Calandra and others 1994; Bacher and others 1996; Wymann and others 1999), the pituitary gland (Bernhagen and others 1993), the liver (Bacher and others 1997), adipocytes (Hirokawa and others 1997), pancreatic islet β cells (Waeber and others 1997), ovarian follicular cells (Wada and others 1997), and the adrenal glands (Bacher and others 1997).
In the past decade, many reports showed that MIF is detectable also in different tissues and fluids during pregnancy, including placenta (Arcuri and others 1999), extra-embryonic membranes, fetal and maternal blood, and amniotic fluid. Importantly, MIF plays a pivotal role in the proinflammatory processes of pregnancy, such as placenta establishment and labor (Ietta and others 2002; Cardaropoli and others 2012).
Increased or decreased MIF concentrations have been correlated with pathological events during pregnancy. Yamada and others (2003) showed decreased MIF plasma levels during early gestation in women with recurrent miscarriages. More recently, we found that maternal serum MIF is significantly higher in patients affected by severe PE, a clinical condition known to be associated with reduced uteroplacental perfusion and placental hypoxia (Todros and others 2005).
In the present study, we investigated whether MIF serum levels are already altered in early pregnancy before PE onset.
Materials and Methods
Subjects and data collection
The study subjects were selected from a prospective study supported by the Italian Ministry of Health (No. RFPS-2007-4-638281). The main aim was to prospectively investigate early markers of pregnancy-related disorders in pregnant women having their routine blood tests at the Laboratory of O.I.R.M.—Sant'Anna Hospital (Turin, Italy) before 20 weeks of gestation. From October 2008 to August 2010, 2,821 women with singleton pregnancies were recruited and interviewed. At recruitment, blood samples were collected and the following data were recorded: maternal age, gestational age, pre-pregnancy body mass index (kg/m2), parity, smoking habits during pregnancy, and risk factors for PE (cardiovascular diseases, diabetes, autoimmune diseases, nephropathies, recurrent miscarriage, previous pregnancy with PE). Follow-up data were collected from patient's medical record or by postnatal interview 1 month after delivery: gestational age at delivery and at PE onset, gestational weight gain at delivery, blood pressure, urinary protein levels, complications occurred during pregnancy, and fetal outcome data.
For this study, 2 subsets of pregnancies (matched for maternal age and gestational age at recruitment) were chosen: the first 48 consecutive pregnancies that afterward developed PE (PE group) and 79 normotensive pregnancies randomly selected among those who delivered at term (controls).
The study was approved by our hospital ethics committee, and written informed consent was obtained from each woman.
Definitions
PE was diagnosed when hypertension (systolic blood pressure ≥140 mmHg or diastolic blood pressure ≥90 mmHg) and proteinuria (≥300 mg/24 h) appeared after 20 weeks of gestational age in previously normotensive women, according to the American College of Obstetricians and Gynecologists criteria (2002). PE was considered severe when one or more of the following criteria were present: systolic pressure ≥160 mmHg or diastolic pressure ≥110 mmHg on 2 occasions at least 6 h apart or significant proteinuria (≥3+on urine dipstick or>5 g in a 24-h urine), oliguria of less than 500 mL in 24 h, cerebral or visual disturbances, pulmonary edema or cyanosis, epigastric or right upper-quadrant pain, impaired liver function, and thrombocytopenia (2002). Patients with PE were further classified as either having early-onset (<34 weeks) or late-onset (≥34 weeks) disease according to the gestational age at which PE was diagnosed.
The hemolysis-elevated liver enzymes-low platelets (HELLP) syndrome was defined by the following criteria: hemolysis (characteristic peripheral blood smear and serum lactate dehydrogenase ≥600 U/L), elevated liver enzymes (serum aspartate aminotransferase ≥70 U/L), and low platelet count (<100,000/μL) (Audibert and others 1996).
Small-for-gestational age (SGA) babies were characterized by birth weight below the 10th centile according to Italian birth weight references (Bertino and others 2010).
Controls were healthy women with a normotensive pregnancy who delivered at term (≥37 weeks) a normal fetus.
Gestational age was calculated from the first day of the last menstrual period and confirmed by ultrasonographic examination before 20 weeks of gestation.
Samples
Maternal venous blood samples (5 mL) were collected into Vacutainer tubes (Becton Dickinson, Plymouth, United Kingdom) without anticoagulant. Serum was separated by centrifugation immediately after clotting and stored at −20°C until assayed.
MIF assay
MIF concentration was assayed in serum samples, collected before 20 weeks of gestation, of 48 pregnancies who developed PE (PE group) and 79 controls by a colorimetric sandwich ELISA as reported by Ietta and others (2002). Briefly, 100 μL/well of anti-human MIF monoclonal antibody (2.0 μg/mL) (R&D Systems, Abingdon, United Kingdom) was used for coating and 100 μL/well of biotinylated goat anti-human MIF polyclonal antibody (200 ng/mL) (R&D Systems) for detection. MIF concentration was calculated by extrapolation from a standard curve (range 25–2,000 pg/mL) using bacterially expressed recombinant human MIF (R&D Systems). The samples and the standards were appropriately diluted in Tris-buffered saline–BSA [20 mM Tris–HCl, 150 mM NaCl (pH 7.3), 0.1% (w/v) BSA, 0.05% (v/v) Tween 20] and assayed in duplicate. The sensitivity limit of the assay is 18 pg/mL. Intra- and interassay coefficients of variation are 3.86%±0.95% and 9.14%±0.47%, respectively. Each MIF assay was run including a standard curve and a combination of cases and controls. The operator was blinded to case–control status. “Single measure” and “average measures” intraclass correlation coefficients, calculated by a “two-way random model with measures of absolute agreement,” were both excellent (0.924 and 0.961, respectively).
Statistical analysis
All data analyses were performed using SPSS version 18.0 (SPSS, Inc., Chicago, IL). Continuous variables were reported as means and standard deviation. Means between the 2 groups were analysed by Student's t-test, preceded by evaluation of variance homogeneity with Levene's test. Means among the 3 groups were compared using one-way analysis of variance. Tamhane post hoc tests, chosen to account for unequal variances, were calculated to identify significant differences between the dependent variables at α<0.05. Categorical variables were presented as frequencies (percentages), and the comparison between different groups was done with chi-square test (χ 2) by means of a 2×2 contingency table; Fisher's exact test was used for small sample sizes.
Spearman's rank correlation was utilized to assess the correlation between MIF concentrations and gestational age at recruitment.
All tests were two-tailed, and the results were considered significant for a P value less than 0.05.
Results
The main characteristics of study population are summarized in Table 1.
P<0.050 versus PE group.
P<0.001.
BMI, body mass index; HELLP, hemolysis-elevated liver enzymes-low platelets; MIF, macrophage migration inhibitory factor; NS, non significant; PE, pre-eclampsia; SD, standard deviation; SGA, small for gestational age.
Gestational age at recruitment ranged between 5 and 18 weeks. The correlation analysis showed no correlation between maternal serum MIF concentration and gestational age in both cases (women who subsequently developed PE) (Spearman's rho=−0.04; P>0.05) and controls (Spearman's rho=−0.03; P>0.05). Therefore, MIF levels were not affected by gestational age at recruitment.
Maternal MIF serum concentration, measured before 20 weeks of gestation, was significantly lower in women who subsequently developed PE compared to controls (4,967±3,119 pg/mL versus 7,640±5,519 pg/mL, respectively) (P<0.001) (Table 1).
Eighteen patients developed early-onset PE and presented significantly lower MIF serum levels (3,983±1,620 pg/mL) compared to controls (P<0.001). Maternal MIF concentration decrease in late-onset PE (5,557±3,642 pg/mL) was not significant (Fig. 1). There were no significant differences when we compared MIF levels in severe versus mild PE as well as in PE-SGA compared to PE without SGA fetuses or in PE complicated by HELLP syndrome relative to PE without HELLP (data not shown).

Maternal macrophage migration inhibitory factor (MIF) serum concentration (pg/mL) in controls, early-onset, and late-onset PE groups.
Discussion
In the present study, decreased maternal MIF serum levels during early gestation showed a significant association with future PE development.
We previously reported that maternal MIF serum levels are higher in patients affected by PE, particularly when the syndrome is associated with fetal growth restriction or when delivery occurs before 34 weeks (Todros and others 2005; Cardaropoli and others 2012).
By an in vitro study on the first-trimester human placenta, we also demonstrated that placental MIF secretion is upregulated by low oxygen tension (Ietta and others 2007). Since severe PE is associated with placental hypoxia and reduced uteroplacental perfusion, we hypothesized that MIF is involved in the early stages of physiopathological placental development.
In stark contrast with the previously observed MIF increase during third trimester of PE pregnancies (Todros and others 2005; Cardaropoli and others 2012), the present findings still support the central role played by MIF in the PE syndrome.
MIF is detectable in plasma and serum of normal subjects at steady levels ranging from 2,000 to 6,000 pg/mL, depending on the assay used (Calandra and others 2000; Aloisi and others 2005). This unique feature makes MIF easy to be monitored to detect its alterations. In this context, reports showed that maternal serum MIF concentration does not change throughout physiological pregnancy. In contrast, higher MIF serum levels were detected in pregnant relative to nonpregnant healthy women (Mizue and others 2000; Ietta and others 2002; Yamada and others 2003) (Fig. 2, dark line).
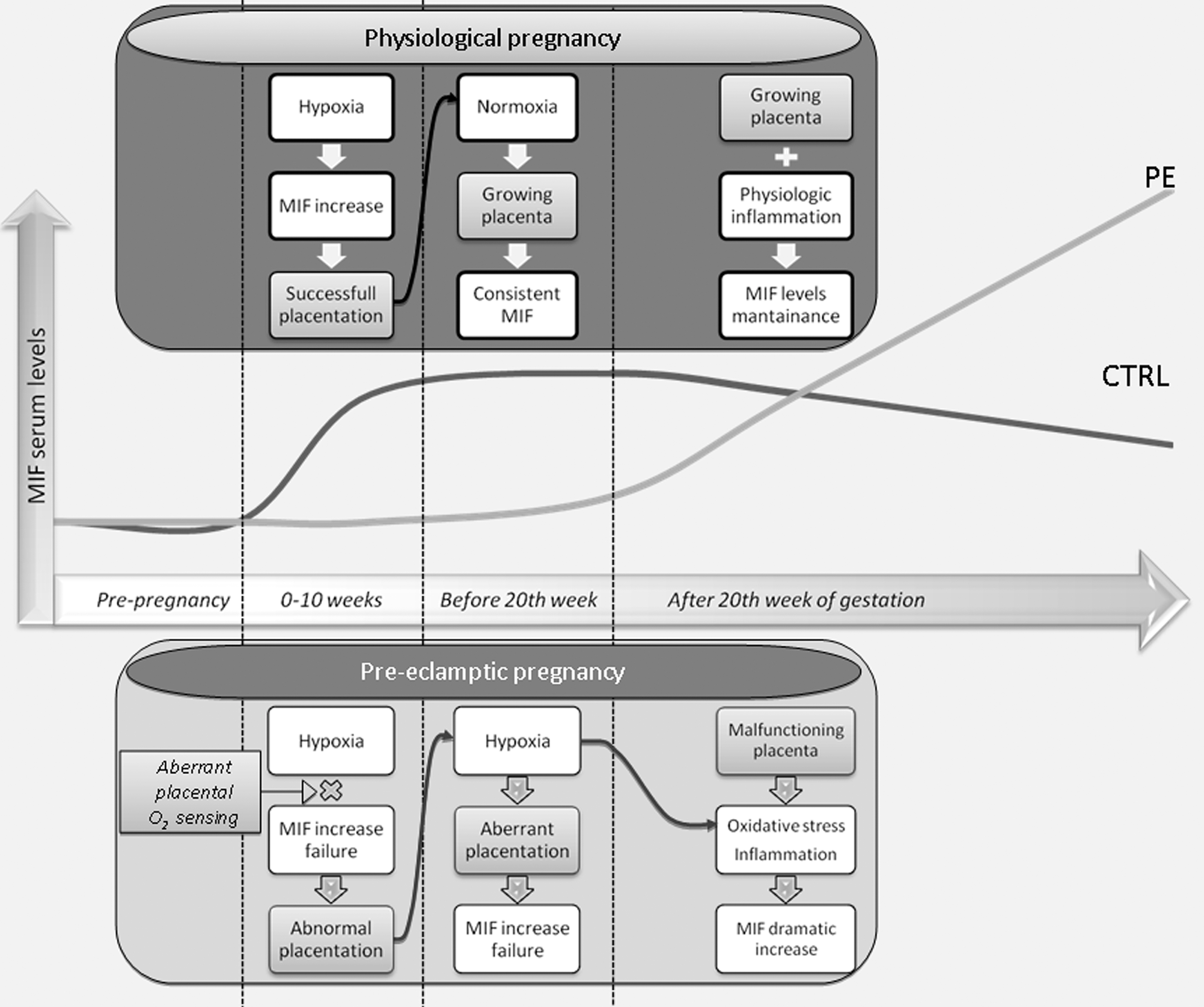
Hypothetical correlation between maternal MIF serum levels and placental development during physiological/pre-eclamptic pregnancy.
MIF increase or decrease was associated with human pregnancy complications, including miscarriage, preterm labor, and PE (Yamada and others 2003; Todros and others 2005; Pearce and others 2008, 2010). More specifically, Yamada and colleagues (2003) showed that decreased MIF maternal serum levels during early gestation were associated with recurrent miscarriages, whereas higher MIF maternal serum levels during early and mid-gestation were linked to spontaneous preterm delivery (Yamada and others 2003; Pearce and others 2008, 2010).
In line with other pregnancy complications, for example, preterm labor, PE syndrome is characterized by altered maternal MIF levels, alteration detectable long before symptoms manifestation. Importantly, MIF levels in PE show variations from normal levels to decrease months prior PE onset and increase in an already diagnosed PE (Fig. 2, light line).
The origin of MIF in maternal serum is not known. Indeed, we can only speculate relying on the literature. Data obtained in normal and pathological pregnancies indicated that fetoplacental tissues, mainly trophoblast cells and amniotic membranes, are a predominant source of MIF (Hristoskova and others 2006; Cardaropoli and others 2012). In normal pregnancy, the involvement of MIF appears particularly striking at the site of implantation where it is expressed by the villous and the extra-villous trophoblast (Arcuri and others 1999). Placenta MIF mRNA and protein levels are higher at 7–10 weeks of gestation when placental oxygen tension is low, whereas it decreases at 11–12 weeks when the maternal–placental circulation is established, with higher oxygen levels (Ietta and others 2007). Therefore, the following pathway is likely to occur: the high production of MIF by the fetoplacental unit at the beginning of pregnancy contributes to high maternal serum levels and to physiological placental development. Indeed, maternal serum levels remain above those of nonpregnant women because the growing placenta and the membranes continue to be a source of this cytokine (Fig. 2, upper pattern).
We speculate that low maternal MIF serum levels at the beginning of pregnancy could cause or be the consequence of abnormal placental development typical of PE. Moreover, it could be linked to pathological alterations in fetoplacental oxygen sensing (Fig. 2, lower pattern “0–10 weeks”). Ortiz-Barahona and others (2010) showed that some polymorphic variants on MIF gene promoter lead to an impaired responsiveness to hypoxic stimuli. The variation of a single nucleotide on MIF promoter can reduce or even abolish the normal upregulation of MIF transcription directly exerted by the transcription factor, hypoxia-inducible factor (HIF), which is highly expressed during the first weeks of pregnancy (Caniggia and others 2000). In patients with these variants, the production of MIF by fetomaternal tissues might be inadequate at the beginning of pregnancy, with a consequent abnormal MIF-dependent placental proliferation and invasion. Furthermore, Rolfo and others (2010) reported the disruption of oxygen sensing in early-onset, but not late-onset, pre-eclamptic placentae. In early-onset PE placentae, they found decreased expression of molecules known to be upregulated in response to low oxygen tensions while HIF levels were increased. It is noteworthy that in our study, pregnant women who subsequently developed early-onset PE had the lowest MIF serum levels (Fig. 1).
Later in pregnancy, approximately at the time of the onset of PE symptoms, a damaged placenta releases necrotic materials that induce a systemic inflammatory response in the pregnant woman (Redman and Sargent 2005; Huppertz 2008) (Fig. 2, lower pattern “after 20 weeks”). Increased levels of a variety of proinflammatory cytokines, such as tumor necrosis factor alpha and interleukin-6, have been demonstrated in serum of women with PE (Conrad and Benyo 1997; Clark and others 1998) and in placental explants from PE pregnancies (Conrad and Benyo 1997). The higher levels of MIF in the maternal serum of PE patients are likely to be the result of a maternal inflammatory response.
Moreover, as reported for other proteins in PE patients, higher levels of MIF in the maternal serum could originate from a leak by the necrotic placental tissue or it could be the result of a feedback process in which the placenta compensates itself for MIF deficiency by late overproduction (Burger and others 2004; Zhong and others 2010).
It is possible that abnormal maternal MIF serum levels could be used as an early marker to detect subjects at risk for early-onset PE, which is often associated with increased fetal–maternal morbidity (von Dadelszen and others 2003). Our data represent a starting point for future investigations aimed to verify the effectiveness of MIF as PE biomarker on a wider population.
In conclusion, our findings provide new insights into the understanding of PE pathogenesis and suggest that low MIF levels in early pregnancy significantly contribute to PE onset.
Footnotes
Acknowledgment
This study was supported by the Italian Ministry of Health (No. RFPS-2007-4-638281).
Author Disclosure Statement
No competing financial interests exist.