
Abstract
Hepatitis C virus (HCV) is a major public health problem. Soluble CD14 (sCD14) level was shown to be associated with HCV infection. In this study, we aimed to investigate the relationship between sCD14 concentration and disease progression, as well as the response to pegylated interferon/ribavirin (peg-IFN/RBV) therapy in Egyptian patients with chronic hepatitis C (CHC). The ELISA technique was used to test 80 patients with CHC and 20 healthy control persons for serum levels of sCD14 (pretreatment and after 12 weeks of treatment). CHC patients were 65 males and 15 females. Normal healthy controls included 20 age- and sex-matched volunteers. The mean age of the CHC patients was 39.94 years, while that of the controls was 39.2 years The serum sCD14 level was significantly higher in chronic HCV-infected patients (3.6±0.18 μg/mL) compared to healthy control subjects (3.1±0.18 μg/mL). The serum sCD14 level was significantly directly correlated with the hepatic fibrosis score (r=0.24, P=0.03), histological activity index (r=0.26, P=0.02), and serum aminotransferases [r=0.28, P=0.005 for alanine aminotransferase (ALT) and r=0.30, P=0.003 for aspartate aminotransferase (AST)]. The pretreatment sCD14 level was not significantly correlated to the treatment response, but it increased after 12 weeks of peg-IFN/RBV therapy and values were significantly higher in nonresponders (P=0.02). The pretreatment sCD14 level cannot predict the treatment response in chronic HCV patients receiving peg-IFN/RBV therapy. However, the serum sCD14 level after 12 weeks of treatment can serve as a negative predictor of treatment response.
Introduction
E
CD14, a protein encoded by the CD14 gene, is a component of the innate immune system. CD14 exists in 2 forms, 1 anchored to the membrane by a glycosyl-phosphatidylinositol tail (mCD14) and the other is a soluble form [soluble CD14 (sCD14)] (Simmons and others 1989). Hepatocytes and Kupffer cells express the membrane-associated form of the endotoxin receptor CD14 (mCD14) at low levels in comparison to peripheral blood monocytes (Schwabe and others 2006). Also, sinusoidal endothelial cells and activated hepatic stellate cells, the main fibrogenic cell type in the injured liver, also express membrane CD14 (mCD14) (Askar and others 2009). mCD14 acts as a coreceptor (along with the Toll-like receptor 4 and myeloid differentiation-2 for the detection of bacterial lipopolysaccharide (LPS) (Tapping and Tobias 2007). Although LPS is considered its main ligand, CD14 also recognizes other pathogen-associated molecular patterns (Ranoa and others 2013). Furthermore, it also localizes with the Toll-like receptor, the double-stranded RNA receptor, in intracellular compartments enhancing dsRNA sensing and Toll-like receptor 3 signaling (Vercammen and others 2008).
sCD14 is constitutively present in the circulation and is apparently derived from secretion of CD14 and from enzymatically cleaved mCD14 (Meiler and others 2005). sCD14 inhibits production of a T helper 1-like cytokine, interferon (INF) gamma, and T helper 2-like cytokine, interleukin 4. Importantly, sCD14 induces progressive accumulation of the inhibitory protein Ikappa B-alpha. So, sCD14 has a negative regulatory effect on T-lymphocyte activation and function by interacting directly with activated T cells (Rey Nores and others 1999).
In patients with chronic hepatitis C (CHC), elevated serum levels of sCD14 have been reported (Meiler and others 2005). IFN-α directly, or indirectly, contributes to monocyte activation and sCD14 release. Whether immune activation attributable to HCV infection plays a role in determining or predicting outcome of HCV therapy is not known (Sandler and others 2011).
First- and second-generation protease and polymerase inhibitors (telaprevir, boceprevir, sofosbuvir, simeprevir) are used for treatment of HCV in Western Europe and the United States. In developing countries, pegylated interferon (peg-IFN) combined with daily oral ribavirin is used.
Given the importance of early predictive parameters of therapeutic efficacy, to limit the frequent side effects of drug exposure in patients unlikely to benefit from treatment, we sought to investigate whether measures of serum levels of sCD14 before the initiation of anti-HCV treatment correlate with response to HCV therapy in HCV-infected patients. Moreover, we aimed to investigate the relationship between sCD14 serum concentration and disease progression in Egyptian patients suffering from CHC.
Patients and Methods
Eighty randomly selected, treatment-naive, Egyptian patients with CHC genotype 4, who were candidates for IFN-based therapy, participated in the study. In addition, 20 healthy subjects were included as volunteers. Informed consent was obtained from each patient according to the 1975 Helsinki Declaration, and the study was approved by the Cairo University Ethics Committee.
Serum samples from all patients and controls were tested for HCV antibodies and HCV RNA by polymerase chain reaction (PCR). Other laboratory tests included complete blood count, fasting blood glucose, aspartate aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase, serum creatinine, and serum albumin.
All healthy controls were negative for HCV antibodies and HCV RNA.
All HCV patients were subjected to quantitative PCR assay for HCV before starting treatment as well as 4, 12, and 24 weeks after beginning treatment. Patients who completed the treatment course (48 weeks) were tested again by PCR 6 months after the end of treatment to detect sustained virological response (SVR). SVR is defined as undetectable HCV RNA in the serum 24 weeks after the cessation of therapy.
HCV RNA was extracted from a 200 μL serum sample using the Ana-gen RNA extraction kit (Qiagene) according to the manufacturer's instructions. cDNA was prepared by reverse-transcription PCR using M-MLV reverse transcriptase (Fermentas). The amplified cDNA was further subjected to 2 rounds of PCR amplifications using a highly conserved primer sequence, upstream primer 5′-GCAGAAAGCGTCTAGCCATGGCGT and downstream primer 5′-CTCGCAAGCACCCTATCAGGCAGT. The conditions for the first round of PCR were as follows: an initial denaturation step at 95°C for 2 min followed by 30 cycles of 45 s at 94°C, 45 s at 54°C, and 1 min at 72°C. PCR cycling conditions for the second round are as for the first round of amplification except for an annealing temperature of 54°C. All PCR products (first and second rounds) were analyzed on a 1.8% agarose gel prepared in 0.5% TBE buffer, stained with ethidium bromide, and visualized by ultraviolet.
Liver biopsy as a routine measure before starting treatment was done to all patients using a Medax 16G×200-mm single-step biopsy needle. Percutaneous liver biopsies were fixed in 10% neutral formalin, processed, then embedded in paraffin, and cut at 5 μm thickness. Histological sections were stained with hematoxylin and eosin stains. Liver sections were evaluated by a single pathologist who was blinded to the patients' clinical and laboratory data.
The degree of inflammatory reaction and the stage of fibrosis were evaluated according to the Metavir scoring system (Bedossa and others 1996).
Before treatment and 12 weeks after treatment, sCD14 was measured in serum samples using the ELISA kit supplied by R&D systems, Inc. catalogue number DC140. This assay employs the quantitative sandwich enzyme immunoassay technique. A monoclonal antibody specific for sCD14 has been precoated onto a microplate. Standards and samples are pipetted into the wells and any sCD14 present is bound by the immobilized antibody. After washing away any unbound substances, an enzyme-linked polyclonal antibody specific for sCD14 is added to the wells. Following a wash to remove any unbound antibody-enzyme reagent, a substrate solution is added to the wells and color develops in proportion to the amount of sCD14 bound in the initial step. The color development is stopped and the intensity of the color is measured.
All patients received a course of pegylated interferon α2b (1.5 μg/kg/week) plus ribavirin (RBV) (1,000–1,200 mg/day) therapy.
Results
CHC patients were 65 males and 15 females. Normal healthy controls included 20 age- and sex-matched volunteers. The mean age of the CHC patients was 39.9 years, while that of the controls was 39.2 years.
Comparing the laboratory data of the chronic HCV patients and healthy controls showed that the transaminase levels were significantly higher in the chronic HCV patients, while the WBC count was significantly lower (Table 1).
Median (IQR) Mann–Whitney U test.
ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; GGT, gamma glutamyl transferase; HCV, hepatitis C virus; IQR, interquartile range; PC, prothrombin concentration; sCD14, soluble CD14; WBC, white blood cells.
Serum sCD14 levels were significantly higher in chronic HCV patients (3.6±0.18 μg/mL) than in the control group (3.1±0.18 μg/mL) (P=0.000) (Table 1 and Fig. 1).

Box plot illustration showing soluble CD14 (sCD14) levels in groups 1 and 2.
It was found that the pretreatment serum sCD14 level was significantly directly correlated with the hepatic fibrosis score and histological activity index (HAI) (Table 2).
HAI, histological activity index.
After receiving a course of peg-IFN-α2b (1.5 μg/kg/week) plus ribavirin (1,000–1,200 mg/day) therapy, patients were classified according to their virological response into responders: 35 patients (43.8%) who achieved SVR and nonresponders: 45 patients (56.3%).
Among the responders group, 20 patients (57.1%) showed rapid virological response defined as undetectable HCV RNA by PCR after 4 weeks of treatment, 12 patients (34%) showed early virological response defined as detectable HCV RNA at week 4 but undetectable at week 12, and 3 patients (8.5%) showed delayed virological response defined as undetectable HCV RNA at week 24 and more than 2 log drop but detectable HCV RNA at week 12. Those patients received a full course of peg-INF/RBV therapy (48 weeks).
While among the nonresponders group, 37 patients (82.2%) were nonresponders defined as failure to clear HCV RNA from serum after 24 weeks of therapy and 8 patients (14.8%) were relapsers defined as the reappearance of HCV RNA in serum after therapy is discontinued.
Demographic features of responders and nonresponders are presented in Table 3.
There was no statistically significant difference in all baseline laboratory and histopathological parameters among the responders group versus the nonresponders group except for the pretreatment hemoglobin level and the pretreatment total white blood cell count, which were significantly higher in the nonresponders group (P=0.01). The pretreatment viral load was higher in the nonresponders group (median=312,662 IU/L and interquartile range (IQR) 88,357–1,306,810 IU/L) compared to the responders group (median=213,000 IU/L and IQR 28,900–842,900 IU/L) with no significant difference (P=0.206) (Table 4).
Median (range) Mann–Whitney U test.
PC, prothrombin concentration; sCD14, soluble CD14.
The pretreatment sCD14 level was higher in the responders (3.6±0.2 μg/mL) than in the nonresponders (3.6±0.2 μg/mL), but with no statistical significance.
After 12 weeks of therapy, the serum sCD14 level was significantly higher in the nonresponders (5.9±1.8 μg/mL) than in the responders (5.1±1.2 μg/mL). Also, the change (rise) in the sCD14 level from the pretreatment level to the level after 12 weeks of peg-INF/RBV therapy was significantly higher in nonresponders (median=1.5 μg/mL and IQR 1–4.2 μg/mL) compared to responders (median=1.1 μg/mL and IQR 0.7–1.7 μg/mL; P value=0.03) (Table 5, Fig. 2).
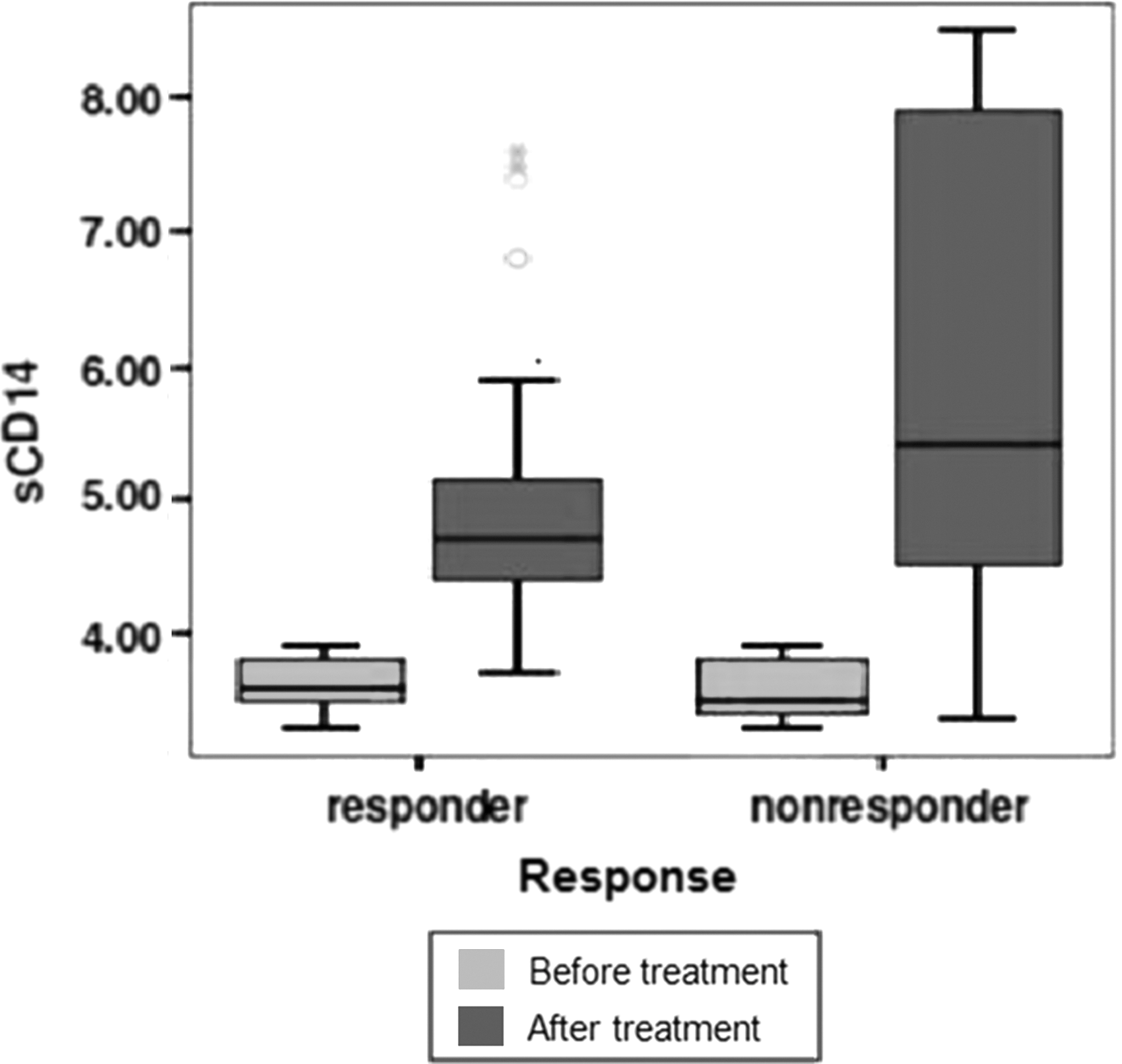
sCD14 levels in responders and nonresponders.
The pretreatment sCD14 level was significantly directly correlated with the pretreatment transaminases (ALT and AST). No significant correlation was found between the pretreatment sCD14 level and the pretreatment viral load. After 12 weeks of treatment, the serum sCD14 level and the sCD14 level change during treatment were significantly directly correlated with the viral load. However, no significant correlation was found between the sCD14 level after 12 weeks of treatment and the sCD14 level change during treatment with any of ALT or AST serum levels (Table 6).
HC, hepatitis C.
Discussion
The outcome of HCV infection is usually related to the interaction between the virus and the host immune response (Heydtmann and others 2001; Esmat and others 2012). In the current study, it was found that the serum sCD14 level was significantly higher in patients with CHC (3.6±0.18 μg/mL) compared to healthy controls (3.14±0.18 μg/mL). This can be explained by the fact that in patients with CHC, elevated serum levels of endotoxins (lipopolysaccharides) had been reported due to impaired phagocytic functions and reduced T-cell-mediated antibacterial activity (Jirillo and others 2002). Furthermore, one cannot exclude the passage of LPS from the gut flora to the blood stream, owing to altered intestinal permeability (Meiler and others 2005). LPS activation of myeloid cells and hepatocytes causes the shedding and secretion of sCD14 (Hiki and others 1998; Paik and others 2013). Moreover, CD14 is expressed on mature monocytes and macrophages, such as Kupffer cells (Schwabe and others 2006), and sCD14 is released from monocytes upon activation (Hiki and others 1998). Our results matched with the results of Sandler and others (2011) who found that sCD14 levels were increased in subjects with either HBV or HCV infection.
A significant positive correlation between the sCD14 serum level and pretreatment serum transaminases evidenced in the current study can be explained by the LPS-induced monocyte activation that is increased in HCV infection (Sandler and others 2011).
Interestingly, we found a significant positive correlation between the sCD14 serum level and the degree of hepatic fibrosis. It is well known that immune activation has been suggested to accelerate liver disease. A possible explanation of the association between the sCD14 serum level and hepatic fibrosis is that patients with HCV display a high degree of microbial translocation and elevated LPS levels that had been strongly associated with the severity of liver disease (Dolganiuc and others 2007; Sandler and others 2011). The increased LPS in the portal circulation would activate Kupffer cells to produce cytokines such as IL-6, tumor necrosis factor alpha, and the profibrotic transforming growth factor β, stimulating hepatic stellate cells to synthesize collagen, resulting in hepatic fibrosis. These effects would be enhanced in patients with higher sCD14 serum levels. In a study performed by Meiler and others (2005), they demonstrated that HCV patients with advanced liver fibrosis or cirrhosis had significantly higher sCD14 levels than patients with less advanced stages of liver fibrosis. Similarly, Sandler and others (2011) showed that compared to subjects with minimal fibrosis, subjects with severe fibrosis had higher plasma levels of sCD14 and more hepatic CD14+ cells.
In this study, SVR was achieved in 35 patients (43.8%) and this agrees with the estimated SVR in genotype 4 as addressed by various studies showing SVR rates varying between 43% and 70% (Manns and others 2001; El Makhzangy and others 2009; Omran and others 2014).
The current study showed that pretreatment sCD14 serum levels were lower in the responders than in the nonresponders with no statistical significance, but serum sCD14 levels increased significantly with treatment in both responders and nonresponders (pretreatment serum level; 3.6±0.18 vs. 5.6±1.6 μg/mL after 12 weeks; P=0.000). IFN-α is a broad immune activating cytokine that directly, or indirectly, contributes to monocyte activation and sCD14 release.
After 12 weeks of treatment, sCD14 serum levels were significantly higher in the nonresponders than in the responders (P=0.02). Also, the change (rise) in sCD14 serum level was significantly higher in nonresponders compared to responders (P=0.03). In a study done on HIV/HCV-coinfected patients, Marchetti and others (2012) demonstrated that EVR and SVR patients showed lower levels of pretreatment sCD14 compared to nonearly virological responders (Null Responders, nonresponders) and non-SVR (N-SVR) subjects. Also, Sandler and others (2011) found that high baseline sCD14 levels were associated with failure to respond to therapy for HCV, reflecting the connection between fibrosis and therapeutic failure. However, they demonstrated that levels of sCD14 did not change appreciably regardless of treatment response.
Week 12 plasma sCD14 levels were found to associate with HCV load. So, this marker of immune activation is a negative predictor of the successful virological response to peg-IFN/RBV therapy.
In conclusion, the sCD14 level was significantly higher in chronic HCV-infected patients compared to healthy control subjects. It correlated significantly with serum transaminases, hepatic fibrosis, and HAI. The pretreatment sCD14 levels were not significantly related to treatment response, however, sCD14 serum levels increased significantly during peg-IFN/RBV therapy and the sCD14 level after 12 weeks of treatment was significantly higher in nonresponders to peg-INF/RBV therapy. So, significant elevation of serum sCD14 levels after 12 weeks of peg-INF/RBV therapy can predict nonresponse to treatment.
Footnotes
Acknowledgment
All authors would like to thank Professor Hasan Hamdy, Prof. of Hepatology, Ain Shams University for discussing this research work.
Author Disclosure Statement
No competing financial interests exist.