
Abstract
Treatment of hepatitis C virus (HCV) in end-stage renal disease (ESRD) patients is an important issue before kidney transplantation (KT). The aim of the study is to assess the efficacy and tolerability of HCV treatment with pegylated interferon (PEG IFN)-α 2b in children with ESRD. The study included 17 children, aged 3–18 years with ESRD on hemodialysis (HD), with chronic HCV. They received 40 μg/m2 of PEG IFN-α 2b once-weekly subcutaneous injections for 48 weeks. Early virological response (EVR) was achieved in 76.5%. At week 24, 8 patients had negative HCV RNA. Six patients received KT during therapy. Treatment was discontinued in 2 patients: one for anemia and another for retinopathy. Two patients completed 48 weeks of therapy and both achieved end-of-treatment response and sustained virological response (SVR). Constitutional symptoms were the most frequently reported side effects. Neutropenia occurred in 10 patients (58.8%), drop in hemoglobin in 10, and thrombocytopenia in 9. HCV-infected children with ESRD on HD have high EVR (76.5%) on IFN monotherapy. SVR could not be assessed due to the high dropout rate related mainly to early transplantation. Constitutional symptoms and hematological side effects were the most frequently reported side effects.
Introduction
H
It is recommended to treat HCV before performing kidney transplantation (KT) (Roth and others 2011) as HCV can flare with the use of immunosuppression (Ingsathit and others 2013), and treatment with interferon (IFN) after KT can trigger acute graft rejection (Kim and others 2011). HCV clearance before KT reduces the risk of posttransplantation complications as hematologic malignancies (Zignego and others 2012), infections (López-Medrano and others 2011), glomerular disease (Meyers and others 2003), and HCV-related new-onset diabetes can affect graft function (Tang and others 2011).
Information on the antiviral treatment of chronic HCV in patients on long-term dialysis is extremely limited (Fabrizi and others 2014). The main therapeutic option for these patients is pegylated IFN (PEG IFN) with sustained virological response (SVR) ranging between 30% and 40% and a withdrawal rate ranging from 17% to 30% (Marinaki and others 2015). There are controversies about using ribavirin (RBV) in patients with ESRD to avoid hemolytic anemia, which can be exacerbated in the presence of kidney dysfunction. Because RBV is filtered through the kidneys, its clearance is impaired in ESRD patients, and it is not removed through dialysis (Liu and others 2013). The new protease inhibitors may be the future for HCV-infected HD patients, although data are still lacking (Marinaki and others 2015).
There is significant paucity of data regarding the efficacy and tolerability of IFN therapy in pediatric patients infected with HCV with ESRD on HD. The aim of our study was to assess the safety and efficacy of treatment with PEG IFN-α 2b monotherapy in children and adolescents with ESRD on regular HD.
Materials and Methods
This is a prospective study that was carried out at the Pediatric Hepatology Unit, Cairo University Pediatric Hospital (Cairo, Egypt). The study included 17 pediatric patients of both sexes who are known to have chronic renal failure with ESRD and chronically infected with HCV. All patients were undergoing regular HD in Pediatric Nephrology Unit and were scheduled for KT. Patients were enrolled in the study after a written informed consent was signed by their parents/guardians. The study protocol was approved by the institutional review board and ethics committee.
Preenrollment investigations included the following: complete blood count (on CELL-Dyn 3700), liver function tests [total and direct serum bilirubin; alanine aminotransferase: ALT; aspartate aminotransferase: AST; alkaline phosphatase: AP; gamma glutamyl transpeptidase: GGT; serum albumin and prothrombin time: PT; (Hitachi 911*; Roche GmbH, Mannheim, Germany)], HCV antibody testing (using third-generation enzyme-linked immunosorbent assay), HCV-RNA testing [using quantitative real-time polymerase chain reaction; PCR; Applied Biosystems 7500 Real time PCR System using kits supplied by Qiagen GmbH; (Hoffmann-La Roche AG) Max-Volmer-Strabe 4-40724-Hilden-Germany], hepatitis B surface antigen (HBsAg), serum creatinine, random blood glucose, serum ferritin, antinuclear antibody (ANA), thyroid-stimulating hormone (TSH), and ophthalmological assessment.
All patients were subjected to full history taking and meticulous clinical examination. Patients included in the study had to fulfill the following criteria: age from 3 to 18 years, total leukocytic count (TLC) >3000/mm3, absolute neutrophilic count (ANC) ≥1500/mm3, hemoglobin level >7 g/dL, platelet count ≥75,000/mm3, serum albumin >3.5 g/dL, PT ≤3 s above the upper limit of normal, normal TSH, ANA <1/40, and negative HBsAg.
Patients were excluded if they had any of the following: body mass index ≥95th percentile (that was calculated using dry body weight, which was measured immediately following the HD session), uncontrolled diabetes, decompensated cardiac disease, significant neurological condition requiring medications, psychiatric disorders, evidence of retinopathy, autoimmune disease, steroid or immunosuppressive therapy, substance abuse, previous IFN therapy within one year, decompensated liver disease (liver cell failure), or any associated cause of liver disease other than HCV.
As clearance of IFN-α 2b is about twice as low in dialysis patients as in nonuremic patients and leads to exaggeration of its side effects (Rostaing and others 1998), we reduced PEG IFN-α 2b dose in our study group from the usual dose of 60 to 40 μg/m2, given as subcutaneous injections once weekly. Low dose of PEG IFN for patients with ESRD was recommended by previous studies, which included adult patients on HD (Fabrizi and others 2008; Wang and others 2014; Marinaki and others 2015).
Efficacy assessment
HCV RNA testing was determined before starting treatment and was repeated after 12 weeks of therapy to assess early virological response (EVR). For patients who had negative or decrease in HCV RNV >2 log, treatment was continued for another 12 weeks; otherwise treatment was discontinued. For patients who completed 24 weeks of therapy, HCV RNA testing was repeated and treatment was continued for another 6 months for those with negative HCV RNA. After 48 weeks of treatment, HCV RNA testing was performed to assess end-of-treatment response (ETR). Patients who had negative HCV RNA at the end of treatment repeated HCV RNA testing at week 72 to assess SVR, which was considered the endpoint of the study.
Safety assessment
To detect potential side effects of IFN therapy, specific investigations (complete blood count, liver functions) and questionnaire directed to the patients were performed at specific intervals (at week 0, 1, 2, 4, and monthly thereafter till end of treatment). Dry weight and height were assessed every 3 months with recalculation of IFN dose accordingly. TSH and fundus examination were done at week 0, 12, 24, and 48.
Patients were questioned in a structured way about the commonly observed and expected side effects of IFN, including fever, chills, fatigue, musculoskeletal pain, headache, nausea, vomiting, anorexia, dyspepsia, itching, skin rash, cough, shortening of breath, hair loss, injection site reaction, decreased concentration, insomnia, and depression.
IFN dose was reduced to 20 μg/m2 if TLC dropped to <1500/mm3, ANC <750/mm3, and platelets <70,000/mm3. Treatment was permanently discontinued if TLC dropped below 1000/mm3, ANC <500/mm3, platelets <50,000/mm3, and hemoglobin <7 g/dL, which was not corrected with maximum increase in erythropoietin dose.
Statistical methods
Data were collected and tabulated. Statistical Package for Social Science (SPSS) program version 17.0 was used for data analysis. Mean and standard deviation (SD) or median and interquartile range (IQR) were estimates of quantitative data, including age and laboratory results; while frequency and percentage were estimates of qualitative data such as sex and treatment side effects. Comparison between basic laboratory results before and after treatment was done. Differences were tested by Student's paired and unpaired t-test, Mann–Whitney U test, or Wilcoxon test for quantitative data. A two-sided P value <0.05 was considered statistically significant.
Results
The study included 17 patients; 9 of them were males (52.9%). Their mean age at the time of enrollment in the study was 11.2 ± 3.9 years (range: 4–18 years). All patients were known to have ESRD, were performing regular HD thrice per week, and were being prepared to perform KT. HCV was discovered during regular screening in the HD unit. All patients were treatment naive, ie, did not receive any treatment for HCV before.
Results of laboratory tests before starting treatment are shown in Table 1. Liver biopsy was not performed in any of the patients to avoid risk of bleeding that may be caused by platelet uremic dysfunction.
ALT, alanine aminotransferase; ANC, absolute neutrophilic count; AP, alkaline phosphatase; AST, aspartate aminotransferase; GGT, gamma glutamyl transpeptidase; HCV, hepatitis C virus; IQR, interquartile range; PT, prothrombin time; SD, standard deviation; TLC, total leukocytic count.
Regarding efficacy of treatment (Fig. 1): at week 8, 1 patient succumbed because of complication of her original renal condition. At week 12, 13 patients (76.5%) achieved early EVR and 3 were nonresponders. Out of the 13 responders, 1 patient dropped out, a second discontinued treatment because of severe anemia, a third died with anemic heart failure, and a fourth was transplanted. The remaining 9 patients were HCV RNA negative at week 24, except one. Five out of the remaining 8 received a KT after 24 weeks of therapy. Treatment was discontinued for 1 patient who developed bilateral retinopathy. Only 2 patients completed 48 weeks of therapy. Both patients achieved ETR and SVR after which 1 was transplanted.

Response of HCV-infected patients with ESRD on chronic HD (n = 17) to IFN monotherapy. ESRD, end-stage renal disease; HCV, hepatitis C virus; HD, hemodialysis; IFN, interferon.
Six patients (35.3%) were transplanted before completing the full course of treatment due to either technical difficulties in maintaining the arteriovenous shunt or uncertainty of donor availability after completion of treatment course. HCV RNA was tested in those patients after KT within a period ranging between 6 and 18 months; 2 relapsed and 4 patients were negative for HCV RNA.
Regarding safety of treatment: side effects were statistically analyzed till the 28th week of therapy due to the small number of patients continuing treatment thereafter. Most of the side effects were constitutional manifestations in the form of fever, the most frequently reported side effect, being present in 82.4% of the patients followed by anorexia (76.5%), musculoskeletal pain (75%), and fatigue (64.7%). Fever had the highest rate of frequency during the first week of treatment and showed another peak at week 8 and musculoskeletal symptoms had the highest frequency during the latest week of therapy (Fig. 2). While frequency of anorexia declined till end of treatment, vomiting had its highest peak at week 16 (Fig. 3).
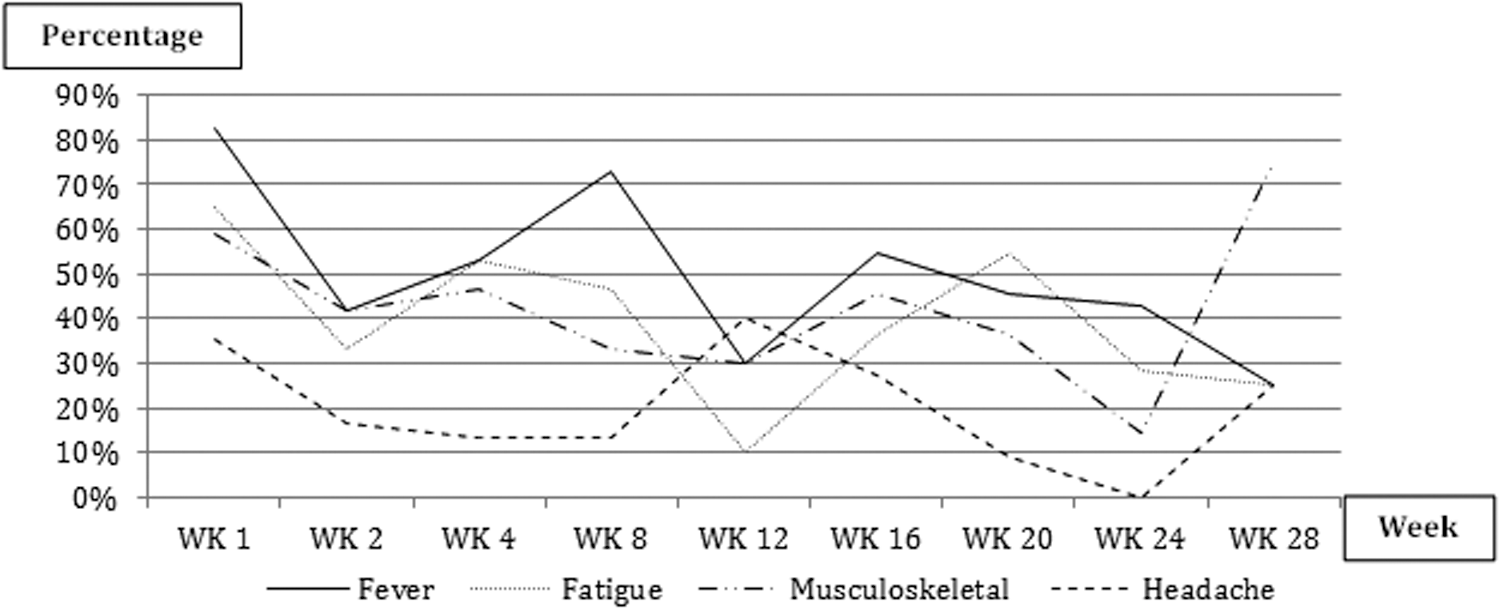
Trend of constitutional symptoms through the 28 weeks of therapy.

Trend of gastrointestinal symptoms through the 28 weeks of therapy.
Neutropenia with ANC <1500/mm3 was observed in 10 patients (58.8%), only 1 had drop of ANC <750/mm3, which required IFN dose adjustment. Drop in hemoglobin level >2 g/dL occurred in 10 patients (58.8%) and necessitated increase in the dose of erythropoietin. Seven out of those patients had drop of hemoglobin level below 7 g/dL, which required blood transfusion and necessitated treatment discontinuation in 1 patient. Nine patients (52.9%) developed thrombocytopenia with platelet count ranging between 70,000 and 130,000/mm3. None of them required platelet transfusion.
One patient developed bilateral retinopathy with optic disc gliosis, which necessitated discontinuation of IFN therapy at week 24. Another patient had elevated TSH level with normal free T3 and T4. Other reported side effects are summarized in Table 2.
Results of basal laboratory tests were compared to results at 12 and 24 weeks of therapy (Table 3). There was statistically significant improvement of ALT level after 12 and 24 weeks (P = 0.001 and 0.009, respectively). There was a statistically significant drop in TLC after 12 weeks and drop in platelet count after 24 weeks of IFN treatment. Although there was a decrease in hemoglobin level, ANC, and increase in creatinine level, the differences did not reach statistical significance.
P < 0.05 is considered significant.
Discussion
HCV infection is one of the major risk factors for lower survival rate among HD patients (Zeniya 2015). Treating these patients with antiviral therapy before KT is safer and more effective than administering this treatment posttransplantation (Fabrizi and others 2006). Immunosuppressive therapy after KT may cause a more rapid and aggressive course of HCV infection (Manuel and others 2012). Administration of antiviral therapy after KT is associated with high risk of graft rejection (Rostaing and others 2012). Achieving SVR before KT should be a primary goal to reduce the likelihood of HCV-related complications in the liver and other systems (Esforzado and Campistol 2012).
Antiviral therapy based on PEG IFN plus RBV for HCV has been considered the standard of care for HCV-infected individuals on regular dialysis with encouraging results in terms of efficacy and safety (Fabrizi and others 2014). There are controversies about adding RBV for treatment of patients with ESRD. Liu and others (2015) stated that most HD patients can tolerate combination therapy with low-dose RBV with greater SVR rate than PEG IFN monotherapy. However, an earlier position statement (Dienstag and McHutchison 2006; Yee and others 2006) did not recommend RBV in dialysis patients, as the drug is not removed during conventional dialysis and its accumulation causes dose-dependent hemolytic anemia (Strader and others 2004; Heathcote and Main 2005). There is no evidence that IFN-RBV combination is superior to IFN monotherapy in those patients (Fabrizi and others 2006). IFN monotherapy was therefore recommended for the treatment of dialysis patients with chronic HCV [Asian Pacific Association for the Study of the Liver (APASL) and others 2007].
Although newer antiviral drugs have been developed for HCV treatment, data are still scanty in patients with renal failure and HD (Marinaki and others 2015); and to date, IFN and RBV are the only approved drugs for treatment of HCV in children. There is extreme lack of data regarding the effect of IFN on HCV-infected children with ESRD who are on regular HD. The aim of our work was to assess the efficacy and tolerability of IFN monotherapy in this very specific group of population.
All patients in our study were asymptomatic and HCV was discovered during routine screening in the HD unit. It is well documented that the clinical course of HCV infection in children and adolescents is usually silent, with minimal histological changes (Abdel-Hady and others 2011).
HD patients with chronic HCV usually have serum aminotransferase levels within the normal range. The diminished values of liver enzymes restrict their diagnostic significance and make them an unreliable tool for hepatitis surveillance (Marinaki and others 2015). Similarly, almost half of our patients had normal transaminase levels before starting treatment, thus regular screening of these patients for HCV is mandatory.
IFN monotherapy of HD patients results in SVR ranging between 31% and 45% (Fabrizi and others 2005, 2008; Gordon and others 2008; Marinaki and others 2015). Ahn and others (2015) reported in their multicenter study that was performed on HCV-infected adult patients with ESRD on regular HD that, over all SVR was 65.7%. Almost half of the patients in their study received IFN monotherapy and to the other half, RBV was added. Thirty-seven percent of their patients dropped out before completion of treatment, and 46.2% showed SVR despite premature termination of treatment. Ninety percent of the 22 patients who completed the scheduled course achieved SVR.
The strength of our study is that it was a single center study that was carried out on a relatively fair number of exclusively pediatric patients with ESRD using the same type, dose, and duration of therapy. This was unlike many other studies that showed heterogeneity regarding IFN type, addition of RBV, and treatment duration (Gordon and others 2008; Wang and others 2014; Ahn and others 2015).
Some studies reported that adult patients with ESRD on chronic HD usually have high SVR rate as they usually have a lower viral load (Liao and others 2011) and increased endogenous IFN release from circulating white blood cells (Badalamenti and others 2003).
Our patients had a higher rate of EVR (76.5%) on IFN monotherapy compared to other studies that included nonuremic children who received combined therapy of IFN and RBV and had EVR ranging between 47% and 68% (Jara and others 2008; Sokal and others 2010; Wirth and others 2010; Schwarz and others 2011; El-Karaksy and others 2016). EVR appears to be a good predictor of SVR (Wang and others 2014) and HCV-infected patients with ESRD should be encouraged to continue therapy.
Because only 2 patients in this study completed the 48 weeks of therapy, we could not calculate the actual SVR or analyze the predictors of response.
Patients with chronic HCV and ESRD on dialysis are difficult to treat and show higher dropout rates during treatment (Ahn and others 2015). In other studies done on adults, the high dropout rate in patients with ESRD (ranging between 17% and 30%) was an indicator of intolerability of administered drugs as it was attributed to side effects of therapy (Russo and others 2003; Fabrizi and others 2008; Marinaki and others 2015). In our study, only 2 patients (11.8%) discontinued treatment because of IFN side effects.
In this study, constitutional manifestations were the most frequently reported adverse events of therapy that occurred in more than 75% of cases and they had low to moderate severity, as they did not affect treatment course. Meanwhile, in adult studies on patients with ESRD, hematological manifestations in the form of leukopenia and anemia followed by depression were the most frequent side effects that led to a considerable dropout rate of patients even with using a low dose of IFN (Wang and others 2014). Gordon and others (2008) reported that fatigue, weakness, and loss of appetite were the most common adverse events in their study group, which was performed on adult patients with ESRD.
Anemia is a common feature in patients with ESRD that is induced by relative erythropoietin deficiency, uremic-induced inhibitors of erythropoiesis, shortened erythrocyte survival, and disordered iron homeostasis (Babitt and Lin 2012). Although we used a 40 μg/m2 dose of PEG IFN instead of the standard dose of 60 μg/m2, hematological side effects in the form of anemia, neutropenia, and thrombocytopenia occurred in more than half of our patients. Hematological adverse events in our pediatric patients with ESRD were more commonly observed than other studies that were also performed on children, but without renal failure (Jara and others 2008; Sokal and others 2010; Wirth and others 2010; Schwarz and others 2011; El-Karaksy and others 2016). Treatment discontinuation in our study group due to hematological side effects was more frequent than reported in the aforementioned studies.
We observed a statistically significant drop in TLC after 12 weeks of therapy and statistically significant drop in platelet count after 24 weeks. Alsaran and others (2013) reported comparable results as there was a statistically significant drop in hemoglobin, TLC, as well as platelet count in their study group. Side effects of IFN therapy should be thoroughly monitored and traced through the whole duration of treatment as some complications such as musculoskeletal pain, insomnia, cough, and skin rash may have the highest peak of incidence during the later phase of therapy.
The limitation in our study is the high dropout rate. This was mainly attributed to early withdrawal for transplantation in addition to complications related to the patients' original renal condition and side effects of IFN therapy. Six of our patients were transplanted before termination of treatment course. This was due to either technical problems in the venous access needed for dialysis or uncertainty of donor availability later on, knowing the fact that in Egypt, we perform only living donor transplantation, which subsequently restricts the opportunities to find a matching donor.
In conclusion, HCV-infected children with ESRD on chronic HD achieved high EVR (76.5%) to IFN monotherapy. SVR could not be assessed due to the high dropout rate that was related mainly to early transplantation. Constitutional symptoms and hematological side effects were the most frequently reported side effects to IFN therapy in these patients.
Footnotes
Acknowledgments
This work has been partially funded by the “Egyptian Liver Care Society.” The authors would like to thank Mrs. Laila Aly and Mrs. Nariman Mostafa for their secretarial work and patient care throughout the work.
Author Disclosure Statement
No competing financial interests exist.