
Abstract
This study aims to investigate the relationship between dental caries and periodontal health by examining the clinical parameters and levels of some biochemical markers in the gingival crevicular fluid (GCF) of the teeth. In 22 children, 22 maxillary primary canine teeth and a pair of primary molars in a total of 38 quadrants were examined. The control group (C) consisted of children who had at least 1 caries-free primary maxillary canine. The test group (T) consisted of children who had a pair of primary molars where the interproximal contact was lost due to the caries in the same quadrant. Their primary molars were restored with compomer. The teeth were evaluated based on clinical values (plaque index, gingival index, and probing depth) and biochemical values in GCF before (C0
, T0
) and after a 6-month treatment (C1
, T1
). While total amounts of interleukin
Introduction
Dental caries is the most common disease in the oral cavity. It affects primary teeth more frequently and progresses more quickly in primary teeth than in permanent teeth due to its enamel structure (Murray and Majid 1978). A lot of interproximal smooth-surface caries were recorded in primary molar teeth (Arnold and others 1998).
Periodontal diseases are a pathological inflammatory condition of the bone support (periodontal tissues) surrounding teeth. The ideal environment for the development of the disease is developed by local facilitating factors such as interproximal caries and inadequate restorations contributing to food retention and food impaction, which create an ideal environment for the bacterial biofilm organization (Bimstein 1995; Page and others 2001). Most studies on periodontal diseases have focused on adults, but primary and mixed dentition has been neglected. Although periodontal diseases are common in adults, there are specific conditions in which this disease occurs in children, such as systemic disease, dental caries, hormonal changes, and so on.
Gingival crevicular fluid (GCF) is an exudate originating from gingival crevices or periodontal pockets around the teeth with inflamed gingiva (Cimasoni 1983). GCF contains a variety of materials, including leukocytes (mainly neutrophils), antibodies, complement proteins, various enzymes, and cytokines (Lamster and Grbic 1995). Therefore, GCF components or constituent measurements can show the alterations in the gingival tissue. Some studies report that poor oral hygiene, gingivitis, periodontitis or gingival injuries, and alveolar breakdown increase the levels of interleukin-1 beta (IL-1β), vascular endothelial growth factor (VEGF), and Osteocalcin (OC) in GCF (Matsuki and others 1993; Zhang and others 2002; Unlü and others 2003; Prapulla and others 2007). Tissue destruction in periodontal disease is the result of the direct toxic effects of the bacteria and the inflammatory response of the host (Genco 1992). A major contributer to the inflammatory response is IL-1β cytokine, a 17-kDa glycoprotein. Its production may be induced by microorganisms, microbial products, inflammatory agents, and antigens (Wilson and others 1998). It has an important role in regulating and increasing the inflammatory response. IL-1β levels in GCF increase in periodontal tissue with gingivitis or periodontitis (Toker and others 2008; Trombelli and others 2010). VEGF, 45-kDa homodimeric glycoprotein, is an angiogenesis and vascular permeability factor, which increases microvascular permeability. The increasing concentration of VEGF in periodontitis (Booth and others 1998; Unlü and others 2003; Güneri and others 2004) may be one of the reasons for the increasing vascularization and permeability and may indicate severe periodontitis (Sakallioğlu and others 2007). OC, a gamma-carboxyglutamic acid (Gla) protein in bones with 5.4 kDa, is a noncollagenous protein in mineralized tissues. OC is predominantly synthesized by osteoblasts under the control of 1.25-dihydroxyvitamin D3 and has an important role in bone turnover and bone formation. OC levels in GCF may reflect inflammation in periodontal diseases (Kunimatsu and others 1993). OC produced locally in GCF probably comes from either an alveolar bone resorption or an active local osteoblast synthesis (Nakashima and others 1994).
Several clinical studies have addressed the changes of IL-1β, VEGF, and OC in GCF in adults with periodontal diseases (Matsuki and others 1993; Zhang and others 2002; Unlü and others 2003; Prapulla and others 2007). In this study, first we processed the knowledge that the caries containing periodontium may exhibit findings similar to periodontitis. To prove this, we looked at the most studied markers IL-1β, VEGF, and OC in GCF in periodontal disease conditions. The aim of this study is to have an idea about the condition of the tooth and its surrounding tissues with the help of clinical and biochemical parameters in primary molars with interproximal caries and to investigate the effect of the restorations of these teeth on the course of the disease.
Materials and Methods
Patient selection
This study was conducted by Ataturk University's Department of Pedodontics Dentistry Faculty. It was approved by the local ethics committee of the medical school (October 26, 2010/30) and conducted in accordance with good clinical practice guidelines. According to the previous power analysis clarifying the changes of biochemical parameters in GCF, the estimated number of participants was 15 per group, with an alpha level of 0.05 and a power of 0.80 (Lee and others 1999).
Twenty-two children (12 girls, 10 boys), aged 5–8 (mean ± standard deviation: 7.05 ± 0.77), were included in this study and their parents signed the consent form.
The criteria for participation included: The presence of at least 1 caries-free maxillary primary canine At least 1 pair of clinically visible cavitations on the occlusal and interproximal smooth surfaces of their primary molar teeth depending on caries Having both primary first molar with disto-occlusal cavitation and primary second molar with mesio-occlusal cavitation in the same quadrant Perpetual food impaction between these primary molars and complaint of uncomfortable chewing on this side
Patients were excluded from the study if they had any systemic diseases or if they had taken antibiotics or anti-inflammatory drugs in the last 30 days or if the soft tissue around the teeth had inflammation or fistula caused by pulpal problems. The study consisted of a test group of 38 primary first molars with disto-occlusal carious lesion and 38 primary second molars with mesio-occlusal carious lesion, which were in the same quadrant (20 maxillary, 18 mandibular). The control group consisted of 22-maxillary primary canines without carious lesions.
Determination of the groups
One group consisting of maxillary primary canines without caries was called “control group” (C) and the other consisting of primary molars with interproximal caries was called “test group” (T). Each group was divided into 2 subgroups (baseline and after 6 months) and called “baseline control” (C0 ), “baseline test” (T0 ), “after 6-month control” (C1 ), and “after 6-month test” (T1 ).
Restoration of primary molars
Seventy-six primary molars in 38 quadrants of 22 children were treated with compomer filling restoration (Glasiosite®; Voco, Cuxhaven, Germany).
All restorations were reevaluated clinically and radiologically after 6 months according to the United States Public Health Service (USPHS) criteria.
Clinical measurements
Periodontal examinations were carried out and recorded by the same investigator (G.D.). Four points (mesio-buccal, mesio-linguale/palatine, disto-buccal, and disto-linguale/palatine) of each primary maxillary canine tooth and 3 points (mesio-buccal, mesial, and mesio-linguale/palatine) of each primary second molar were selected for clinical measurements. The gingival conditions of the patients were evaluated with Silness–Loe plaque index (PI) (Silness and Loe 1964) and Loe gingival index (GI) (Loe 1967). Probing depth (PD) was recorded to the nearest millimeter with a Williams probe. The obtained scores were calculated by dividing the total score by the total number of surfaces scored. Simplified oral hygiene index (OHI-S) related to plaque was evaluated at baseline and after 6-month treatment. All participants and their families were given oral hygiene training at baseline.
GCF collection
Mesio-buccal sites of both the maxillary primary canines and primary second molars for each subject were selected for GCF sample collection. A total of 120 GCF samples were obtained. These consisted of 38 samples from primary second molars and 22 samples from maxillary primary canines at baseline and then 6 months later. To obtain the samples a paper strip (Periopaper®; Oraflow, NY) was placed in the pocket for 30 s. In the case of visible blood contamination, the strips were discarded. The paper strips with GCF were transported to a previously calibrated electronic gingival fluid measuring device (Periotron® 8000; Oraflow, Plainview, NY) for volume calculation. The periotron scores were converted into microliter (μL) using mL-converter software. The paper strips were put into 300 μL-Eppendorf tubes containing 100 μL of 2% bovine serum albumin in phosphate buffered saline. The samples were then mixed by vortex for 30 s and centrifuged at 10,000 rpm for 5 min at 4°C. The strips were thereafter removed from the tube to prevent the proteins from redepositing. The eluted GCF samples were stored at −80°C until the day of laboratory analysis.
Biochemical assay
The samples were brought to room temperature. The levels of IL-1β and VEGF in GCF were measured by enzyme-linked immunosorbent assay (ELISA) (eBioscience® Platinium ELISA, NY, for IL-1β; RayBiotech, Inc., Norcross, GA, for VEGF) at 450 nm, and the analysis was performed according to the manufacturer's instructions using human recombinant standards in Biochemistry Laboratory. OC measurements in GCF were made using an electrochemiluminescence technique.
The measured values were recorded in pg/mL for IL-1β and VEGF and ng/mL for OC. The values of sensitivity for IL-1β, VEGF, and OC were 0.3 pg/mL, 10 pg/mL, and 0.5 ng/mL, respectively. The levels below the limits of the assay's detectability were 0. The results were multiplied by the dilution factor for IL-1β ( × 2).
The measured values (mL) were converted into μl. Total amounts of IL-1β, VEGF, and OC in GCF were measured.
Statistical analysis
Data analysis was performed using the statistical package SPSS 16 (2008; SPSS Inc., Chicago, IL). The data were first analyzed for the normal distribution with the Shapiro–Wilk test. GCF measurements for the total amounts of IL-1β and VEGF demonstrated skewed distributions; therefore, logarithms of the geometric means of variables were used in the analysis.
Statistical analysis was performed using Pearson correlations and Student's t-tests for all GCF measurements (IL-1β, VEGF, OC) and using Spearman's Rank correlations, Mann–Whitney U, and Wilcoxon Signed Rank tests for clinical parameters. The Wilcoxon Signed Rank test was used to compare OHI-S between baseline and after 6 months of the treatment. The correlation between clinical and laboratory parameters was evaluated with Spearman's Rank test.
Results
In this study, all participants' clinical values, which are OHI-S, PI, GI, PD, and GCF volume, and biochemical values, which are IL-1β, VEGF, and OC in GCF, were evaluated at baseline and after 6 months in primary molars with interproximal caries and primary canine without caries.
No issues were reported on the survival of compomer restorations of primary molars with interproximal caries after 6 months according to the USPHS criteria.
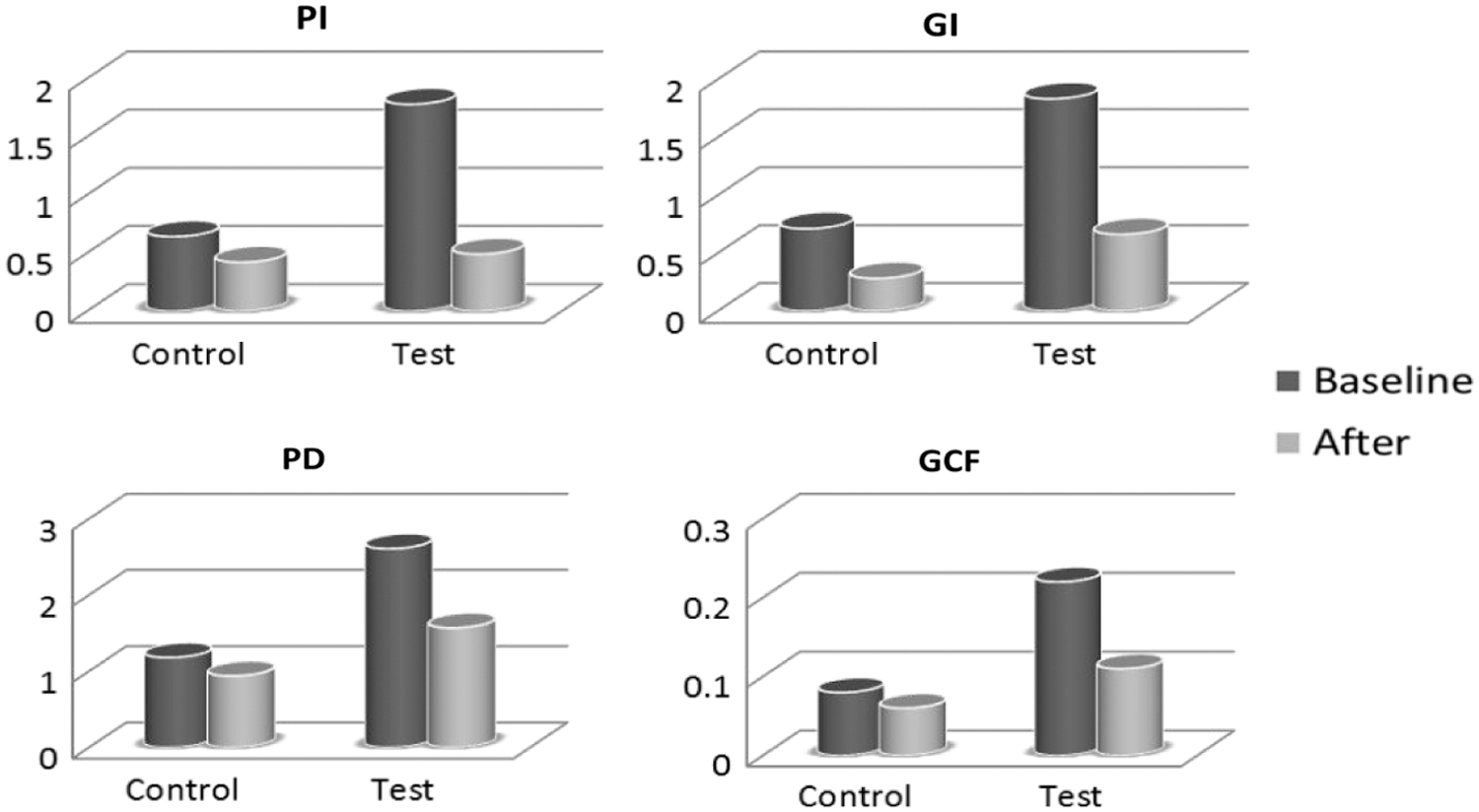
The values of clinical parameters in test group were statistically higher than the control group at baseline (P < 0.01) (Table 1, Fig. 1). Similarly, at baseline, the total amounts of IL-1β, VEGF, and OC were statistically higher in the test group than in the control group (P < 0.01, P < 0.05, respectively) (Table 2, Fig. 2).
The comparison of the mean clinical values between control and test groups at baseline and after.

The comparison of the mean biochemical values between control and test groups at baseline and after.
Mean ± Standard Deviation of Clinical Parameters in Groups
Mann–Whitney U test.
Wilcoxon Signed Rank test.
GCF, gingival crevicular fluid; GI, gingival index; PD, probing depth; PI, plaque index; SD, standard deviation.
Mean ± Standard Deviation of Biochemical Parameters in Groups
Student's t tests.
Wilcoxon Signed Rank test.
IL-1β, interleukin
After 6 months, all clinical parameters (GI, PD, and GCF volume) except PI were statistically higher in the test group than in the control group (P < 0.01) (Table 1). However, no statistically significant difference was found between the control and test groups for biochemical parameters (P < 0.05) (Table 2).
When the baseline and after 6-month values were compared, a statistically significant decrease was observed in all clinical parameters and the values of the total amounts of IL-1β and VEGF in both control and test groups after 6-month follow-up visits (P < 0.05) (Tables 1 and 2). However, no statistically significant difference was observed for the total amounts of OC in both control and test groups (P > 0.05, Table 2). In addition, OHI-S values were higher at baseline (1.18 ± 0.27) than the values after 6 months (0.65 ± 0.13) (P < 0.01).
The values of the mean and standard deviation of clinical and biochemical parameters and P values are shown in Tables 1 and 2, respectively.
When clinical parameters were compared with each other, a positive correlation was found between IL-1β and VEGF, while OC had no correlation with IL-1β and VEGF in all groups. IL-1β and VEGF had a positive correlation with GI and PI in all groups (Table 3). The parameters correlating positively with each other are shown in Table 3.
The Parameters Correlating Positively with Each Other
P < 0.05, ** P < 0.01.
Discussion
In this study, the effect of interproximal caries on periodontal health, whether the damage of caries to periodontium is reversible, and the extent to which periodontal damage will improve when the agent is eliminated were investigated. The severity of the condition, which is severe as if it were a periodontal disease in clinical and radiological examination, with more concrete evidence, IL-1 β, VEGF, and OC, was asked to be put forward. Although these markers have been included in many studies about periodontal disease (Matsuki and others 1993; Zhang and others 2002; Unlü and others 2003; Prapulla and others 2007), no study has been encountered in the literature to emphasize the severity of caries. However, one of the reasons of the tooth loss is caries that affect the periodontium.
Periodontitis is a disease characterized by inflammation and can cause destruction of the tooth-supporting tissues (Bimstein 1995). Kurtiş and others (2005) found that PI, GI, PD, and clinical attachment level (CAL) values were lower in the control group than in the groups with periodontitis. In this study, in accordance with Kurtiş and others, clinical findings (PI, GI, PD, and GCF volume) in T0 , which exhibited similar symptoms to periodontis, were higher than in other groups. For PD, we did not look into the differences between control and test groups because of different anatomical structures of teeth (canine tooth and primary molar tooth). Only the differences between C0 and C1 and between T0 and T1 were evaluated.
After 6 months, in primary molars which regained the missing interproximal contact points because of restorative treatment of them, the values of all clinical parameters (PI, GI, PD, and GCF volume) showed a decline. This situation exhibits that interproximal contact points of teeth indicate good clinical status. Hans and others (2012) reported that PI, GI, PD, and CAL values dropped in adult chronic periodontitis after periodontal treatment, which is similar to our findings due to the removing of the irritation factor. In this study, in primary canine teeth, the results at the beginning and after 6 months may be similar to those of primary molars due to the oral hygiene education and caries-free oral cavity.
There are various bacterial species and host-derived factors embedded in a matrix of bacterial products in a dental biofilm or dental plaque. This biofilm can stimulate the inflammation in gingival tissue. The inflammation results in the enhancement of the GCF (Loe and Holm-Pedersen 1965), and as a result, it indicates gingivitis (Loe and Holm-Pedersen 1965). Like Sandalli and Wade, we also found a positive correlation between PI and GCF volumes (Sandalli and Wade 1971). In addition, we found a positive correlation between GI and GCF volumes and PD and GCF volumes as recorded by Yücel and others (2008) in deep pockets compared to shallow pockets in primary molars.
Previous studies observing periodontal mediators have generally focused on adult populations and compared cytokine levels in tissues, saliva, or fluids of periodontally healthy subjects with periodontitis. Consequently, the data on the levels of periodontal disease markers in children with a periodontal problem resulting from dental caries and food impaction remain inadequate. To our knowledge, in children's GCF, while there are few studies on IL-1β (Lerner and others 1998; Ulker and others 2008), there are no studies on the levels of VEGF and OC. In literature, we did not find any studies measuring IL-1β, VEGF, and OC levels in children's GCF, except our previous study. In our previous study (Duruk and others 2017), we showed poor oral hygiene in epileptic children with clinical (PI, GI, and PD) and biochemical (IL-1β and VEGF in GCF) parameters. In epileptic children, these parameters were higher than in healthy children (P < 0.001). We attributed this to the fact that epileptic children and their families don't care about their oral health. In the present study, the OHI-S scores significantly decreased after the motivational training program for oral hygiene; however, the levels of IL-1β and VEGF in GCF decreased in the caries-free control group.
In periodontitis, pathogenic bacteria in the subgingival plaque cause a subepithelial infiltration by inflammatory cells, which produces and releases IL-1β (Matsuki and others 1993). As a result, IL-1β concentration in GCF increases in periodontal tissue with gingivitis or periodontitis (Toker and others 2008; Trombelli and others 2010), and VEGF is increased by gingival fibroblasts in response to vesicle and outer membrane protein from periodontopathic bacteria. IL-1β, IL-6, and PGE2 can induce VEGF release (Ben-Av and others 1995). In our study, the total amounts of IL-1β and VEGF in GCF showed positive correlations. The highest scores of the total amounts of IL-1β and VEGF were found in primary molars with approximal caries. These teeth were periodontally destructed teeth due to food impaction, and the laboratory results clearly demonstrated the condition of the teeth. The teeth were restored to investigate whether this negative situation was reversible or not, and the results after 6 months showed that the condition was reversible because the total amounts of both cytokines in GCF of these teeth decreased (P < 0.01) and showed that these values were similar to the values of control group (P > 0.05). These laboratory results were consistent with clinical findings. Likewise, many studies in adults have shown that the biomarkers in GCF of teeth with periodontitis increased but a decrease was detected after the periodontal treatment (Toker and others 2008).
The total OC levels in GCF are higher in T0 than in C0 statistically. This is contrary to the finding of Lee and others who reported that the diseased and healthy sides showed the same results (Lee and others 1999). In line with the results of our study, Kunimatsu and others (1993) showed that OC levels in the diseased side were higher than in the healthy side. The level of OC in T0 may have incresed as a result of the alveolar bone resorption in the septal area depending on interproximal tooth caries, connected directly to the gingival crevices and extending below the gingival margin. This type of caries may have stimulated osteoblastic and odontoblastic activities to balance the bone turnover in the interproximal area. In addition, OC levels in T0 showed a positive correlation with PD, which is one of the most significant signs of periodontal breakdown and alveolar bone resorption.
In our study, there were no significant differences between the groups for OC, except in T0 . The cause of these similar values between groups for OC may be the physiological root resorption by odontoclasts/cementoclasts in primary teeth and alveolar bone remodeling by osteoblasts and osteoclasts during the child's skeletal growth. The imbalance between bone formation and resorption during bone remodeling can cause OC expression. The researchers point out that OC levels in GCF increase during bone formation and resorption (Nakashima and others 1994). In this study, although OC release in GCF was the highest in T0, bone resorption detected, this release was detected in all other groups.
In this study, the results for IL-1β, VEGF, and OC, which are important markers of periodontal disease, were supporting the clinical findings. The level of these 3 biomarkers increased in GCF of the teeth with interproximal caries at baseline, and the level of IL-1β and VEGF decreased after the dental treatment. Based on all these, it can be called a reversible periodontal disease for interproximal caries.
In summary, this study confirms that although OC is limited, IL-1β and VEGF are effective for evaluating the condition of periodontium in teeth with interproximal caries and can, thus, be used as a laboratory tool for assessing the severity of interproximal caries.
Limitations
Since there were no similar studies on this subject, no comparison could be made with other studies.
Conclusions
This study was demonstrated with clinical and biochemical methods that interproximal caries are a major threat to periodontal health. In teeth with interproximal caries, periodontal tissues might show symptoms of periodontitis. Their restoration in accordance with the anatomical form of teeth is important to regain periodontal health.
Early diagnosis of dental caries and treatment of them has the greatest impact on teeth and periodontal health. IL-1β and VEGF cytokines can be used as a biomarker to show the severity of interproximal caries. Further studies are needed to evaluate the relationship between dental caries and periodontal diseases and to identify new biomarkers in child population. This study will shed light on future studies on the subject.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Scientific Research Foundation of Ataturk University (grant 2010/140).