
Abstract
The gout-induced continuous deposition of urate in the kidney tissues is the main cause of renal injury, for which cystatin C (Cys C) is an important indicator. This research analyzed the correlation between general renal injury indicators and serum Cys C level, and further investigated the potential of Cys C in renal injury diagnosis. A total of 140 gout patients with renal injury (GRI) were recruited and grouped by their glomerular filtration rate (GFR). Urea nitrogen, uric acid, creatinine, and Cys C levels in the serum were evaluated. The diagnostic efficacy of serum Cys C was evaluated by the nonparametric receiver operating characteristic analysis. Serum Cys C level was increased with decreased GFR in GRI. Urea nitrogen, uric acid, and creatinine levels in the serum showed positive correlations with Cys C level. The area under the curve for serum Cys C was 0.8589 (P < 0.001). In conclusion, this research demonstrated that the serum Cys C level was a precise diagnostic marker for GFR and renal damage evaluation, and showed a significant diagnostic value for renal injury in patients with gout.
Introduction
As a common metabolic disease, gout is caused by a significantly increased production of uric acid due to abnormal purine metabolism (Hainer and others 2014). A large amount of urate is deposited in the synovium, bursa, and cartilage of the joints, which triggers a series of inflammatory and pathological reactions (Perez-Ruiz and Dalbeth 2019). With economical and social progression, people's living standard has been significantly improving in recent years. The intake of a large amount of high-protein foods and a faster pace of life have led to a gradual increase in the incidence of gout (Chen and others 2017). In severe cases, renal injury is caused during the pathogenesis of gout (Kanji and others 2015), as the result of continuous deposition of urate in the kidney tissues (Johnson and others 2013). Impaired renal function not only affects the health of the patient but also brings a serious economic burden to the patient. When gout patients with renal injury (GRI) cannot get effective and timely intervention at an early stage, it is likely to cause various vascular lesions, which could become seriously life-threatening (Pascual and others 2018). Therefore, early diagnosis of kidney injury in patients with gout and timely intervention have become a key clinical research direction.
Clinically, serum blood urea nitrogen (BUN) and creatinine are usually used to identify abnormal kidney function at an early stage (Levey and others 1999). Cystatin C (Cys C) is another important kidney injury indicator. As a 13-kD nonglycosylated protein, Cys C is an inhibitor of cysteine protease expressed in almost all nucleated cells. The serum level of Cys C is not significantly altered by diet, gender, or body muscle mass (Woo and others 2014; Kashani and others 2017). However, systemic inflammation and the use of corticosteroid can influence Cys C serum level (Stevens and others 2009). Cys C is freely filtered by the glomerulus and not secreted by renal tubules. Thus, serum Cys C level is reported to have a strong correlation with the glomerular filtration rate (GFR) (Nejat and others 2010; Wan and others 2013). As an inflammatory disease, the pathogenesis of gout is related to the expression of the matrix degrading proteinase cathepsin B and its endogenous inhibitor Cys C (Chu and others 2010). Previous research has shown that the renal damage of male gout patients can be indicated by the serum level of Cys C (Choe and others 2010). Another research also indicated that Cys C showed clinical significance for early diagnosis of renal injury in gout patients (Zhang and others 2019). However, these studies on the correlation between Cys C and renal injury in gout patients have some limitations: they did not analyze the relationship between Cys C and other indicators, or classify and analyze the degree of kidney damage associated with gout.
Based on these results, this research aimed to classify the degree of kidney damage in patients with gout, demonstrate the correlation between general renal injury indicators and serum Cys C level, and further reveal its diagnostic significance for renal injury.
Methods
Patient eligibility
All gout patients and healthy control were recruited from the Qingdao Municipal Hospital from 2018 to 2019. This research was approved by the Ethics Committee of Qingdao Municipal Hospital. In this research, a total of 187 gout patients were recruited and grouped by estimated GFR. Meanwhile, the healthy control group was composed of 35 healthy people with matched age and gender. In this research, a total of 21 patients withdrew from the observation because of the loss of contact or unwillingness to continue the research.
Inclusion criteria: All patients were diagnosed to meet Holmes' definition of gout and signed an informed consent. Exclusion criteria: (1) Patients with severe renal insufficiency; (2) patients with abnormal heart and liver functions; (3) patients with primary nephropathy or secondary hyperuricemia; (4) patients has a recent history of taking nephrotoxic drugs; (5) patients treated with drugs that interfere with uric acid metabolism; and (6) patients with complications including cardiovascular and cerebrovascular diseases, urinary system diseases, hypertension, and/or diabetes.
Glomerular filtration rate
In this research, GFR was estimated through creatinine clearance in a 24-h urine collection. All the gout patients enrolled in this research were divided into 4 groups based on the Kidney Disease Outcomes Quality Initiative (K/DOQI) guidelines. GRI-0: patients with normal GFR (≥90 mL/min/1.73 m2 and persistent albuminuria); GRI-I: patients with mildly decreased GFR (60–89 mL/min/1.73 m2 and persistent albuminuria); GRI-II: patients with moderately decreased GFR (30–59 mL/min/1.73 m2); and GRI-III: patients with severely decreased GFR (<30 mL/min/1.73 m2).
Sample collection
Urine samples and fasting venous blood samples were collected in the morning from participants in different groups. Before 8 o'clock of the previous night, the patients were instructed to fast, water, and not to take any heavy physical activity. Blood samples were collected from the forearm vein and then centrifuged for 30 min at 3,000 r/min. Blood supernatant was collected and stored at −80°C for testing. About 10 mL clean midstage urine was simultaneously collected in a sterile tube. The urine samples were centrifuged for 30 min at 3,000 r/min to collect the supernatant, which was stored at −80°C for testing.
Sample test
The serum concentrations of urea nitrogen, uric acid, and creatinine were evaluated by the COBAS INTEGRA 400 plus analyzer (Roche, Switzerland) according to the manufacturer's instruction. Cys C level in the serum was evaluated using the Cystatin C Detection Kit (ERKN, China) based on the manufacturer's instruction. Serum interleukin-1β (IL-1β) level was analyzed by the IL-1β ELISA Kit (Abcam, Waltham, MA).
Statistical analyses
In this research, statistical analyses were performed by SPSS version 17.0 software. The data were presented as mean ± standard deviation or number (n) and proportion (%). The differences in continuous variables from different groups were compared by analysis of variance test followed by a Dunn's multiple comparisons test. Linear correlations were verified using the Spearman's correlation analysis. The diagnostic values of serum Cys C were evaluated by nonparametric receiver operating characteristic (ROC) analysis. The area under the curve (AUC) showed the diagnostic accuracy. *P < 0.05, **P < 0.01, and ***P < 0.001, ns means no significance.
Results
Demographics and clinical characteristics of participants
Figure 1 shows the experimental diagram of this research. One hundred eighty-seven gout patients were assessed for eligibility and 140 of them were recruited in this trial. Another 35 healthy people were also involved in this study as the healthy control group. Based on the level of GFR, 140 gout patients were assigned into the GRI-0, GRI-I, GRI-II, and GRI-III groups. During this research, a total of 21 patients withdrew.
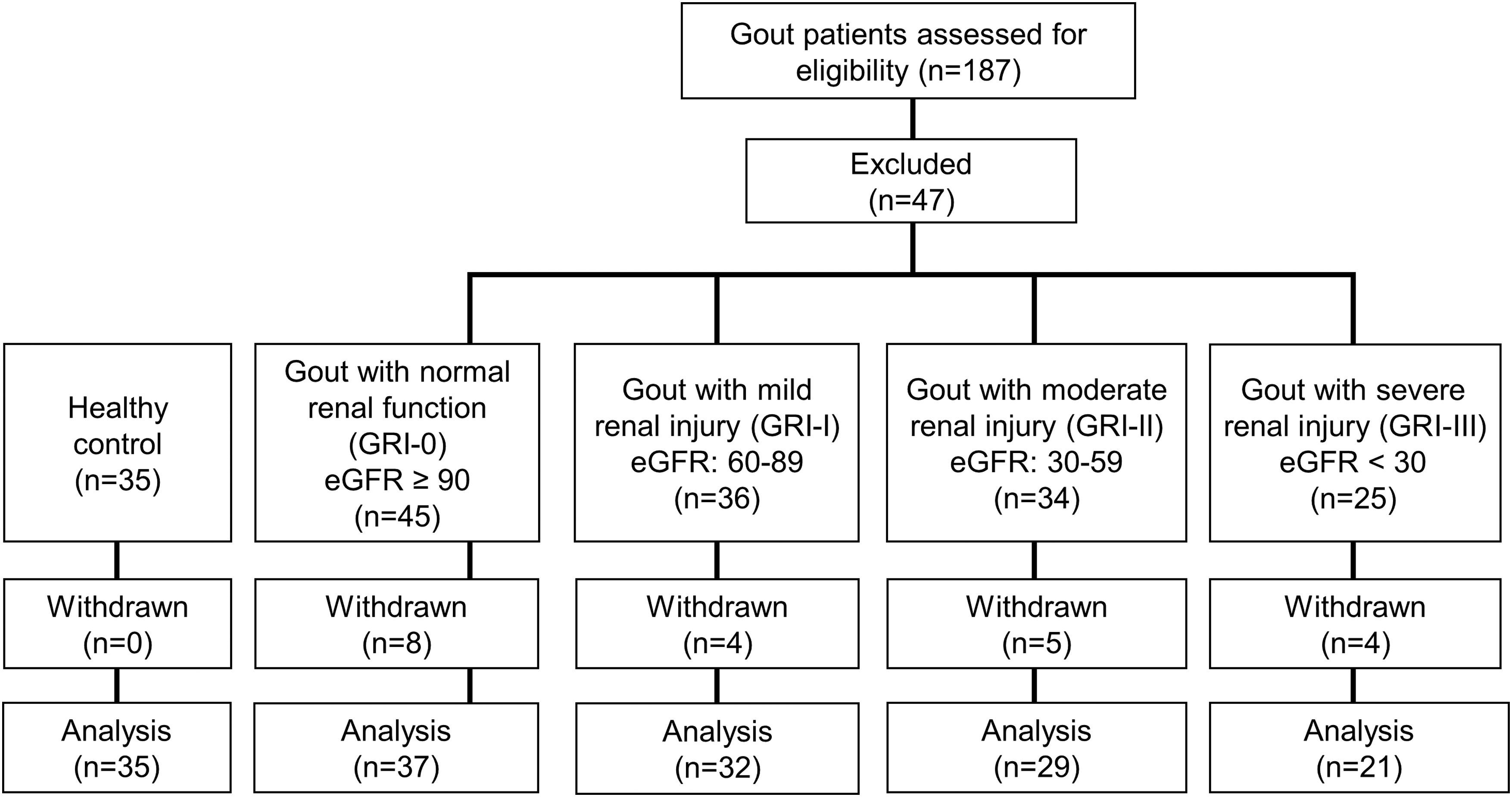
Experimental diagram in this study. eGFR, estimated glomerular filtration rate; GRI, gout patients with renal injury.
Participants' demographic and clinical characteristics are shown in Supplementary Table S1. No significant differences were found in the participants of different groups with respect to age, sex, distribution, and body mass index (all P > 0.05). Meanwhile, significant differences were found in gout duration, creatinine clearance, serum Cys C, serum uric acid, serum creatinine, and BUN among these groups (all P < 0.001).
Serum Cys C showed negative correlation with creatinine clearance in GRI
As shown in Fig. 2A, decreased GRI correlated with decreased creatinine clearance. Simultaneously, enhanced severity of renal injury in gout patients was correlated with increased serum Cys C level (Fig. 2B). Spearman's correlation indicated that creatinine clearance showed a negative correlation with serum Cys C level in patients (Fig. 2C).
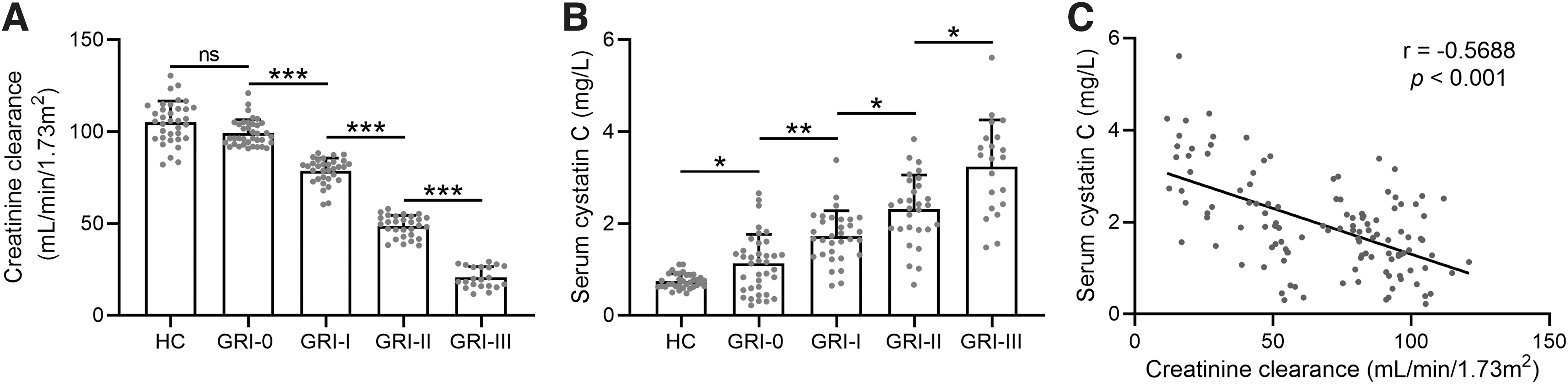
Relationship between serum Cys C and creatinine clearance in GRI
Enhanced severity of renal injury of gout patients elevated 3 indexes of kidney injury
In this research, we analyzed 3 different indexes of kidney injury: serum uric acid, serum creatinine, and BUN. As shown in Fig. 3A–C, all these 3 indexes were significantly elevated by enhanced renal injury in gout patients.
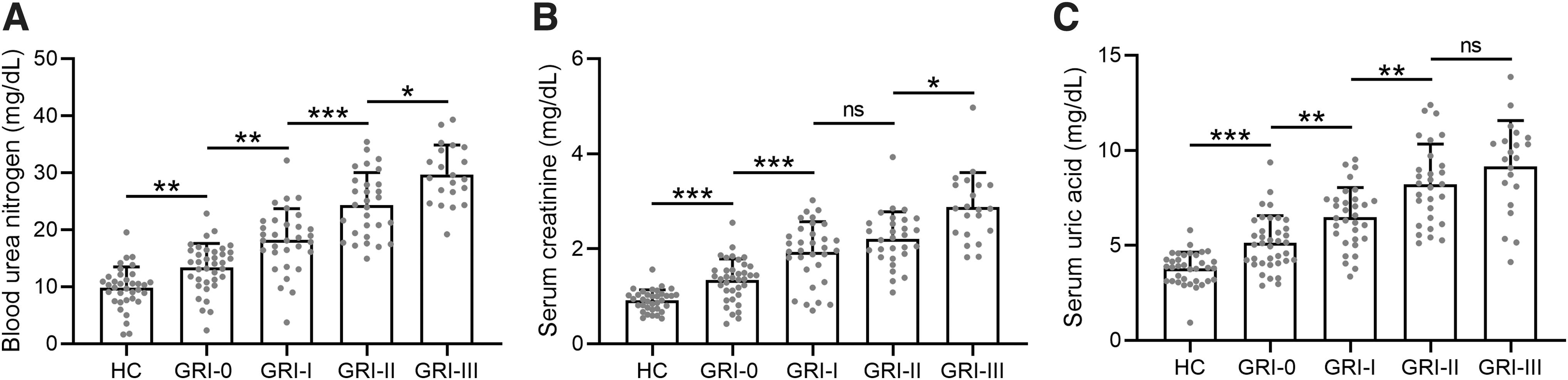
Levels of urea nitrogen, creatinine, and uric acid in serum of participants in different groups.
Serum Cys C showed positive correlation with indexes of kidney injury in GRI
The correlations between serum level of Cys C and the 3 different kidney injury indexes were also analyzed. In GRI, serum uric acid, serum creatinine, and BUN all exhibited positive correlations with serum Cys C (Fig. 4A–C).
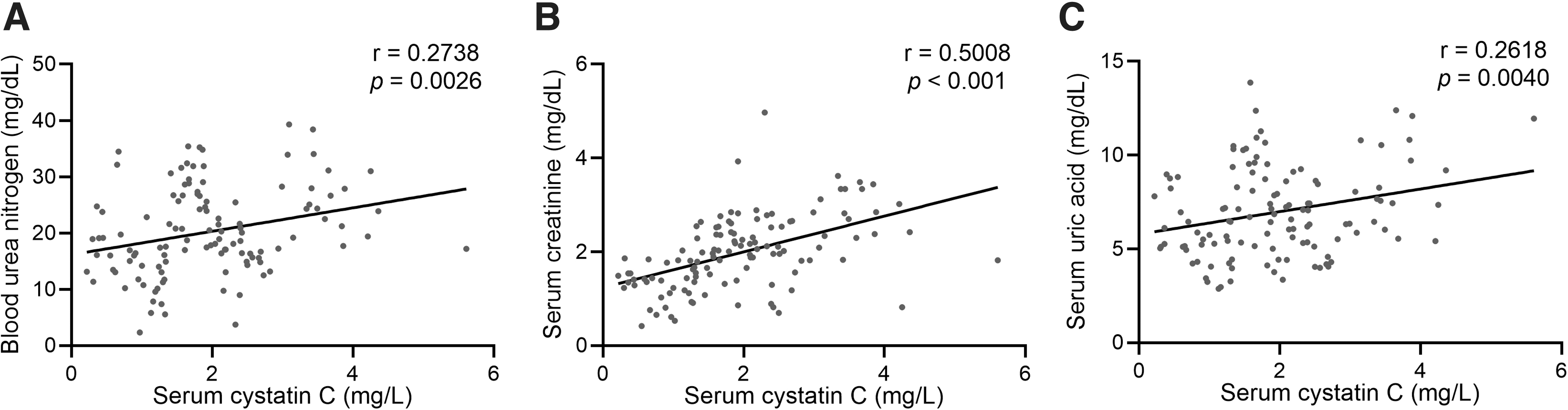
Relationship between serum Cys C and renal injury indexes in GRI Spearman's correlations of serum Cys C level with BUN level
Serum Cys C showed positive correlation with serum IL-1β concentration in GRI
We further analyzed the serum IL-1β concentration of GRI. As shown in Supplementary Fig. S1A, serum IL-1β level was significantly elevated by enhanced renal injury in gout patients. Furthermore, serum IL-1β level also exhibited a positive correlation with serum Cys C (Supplementary Fig. S1B).
Diagnostic accuracy of serum Cys C for renal injury in gout patients
ROC analysis was used to evaluate the diagnostic accuracy of serum Cys C. Results illustrated that the AUC for serum Cys C was 0.8589 (Fig. 5, P < 0.001), suggesting that serum Cys C was an effective marker in the diagnosis of renal injury in gout patients.
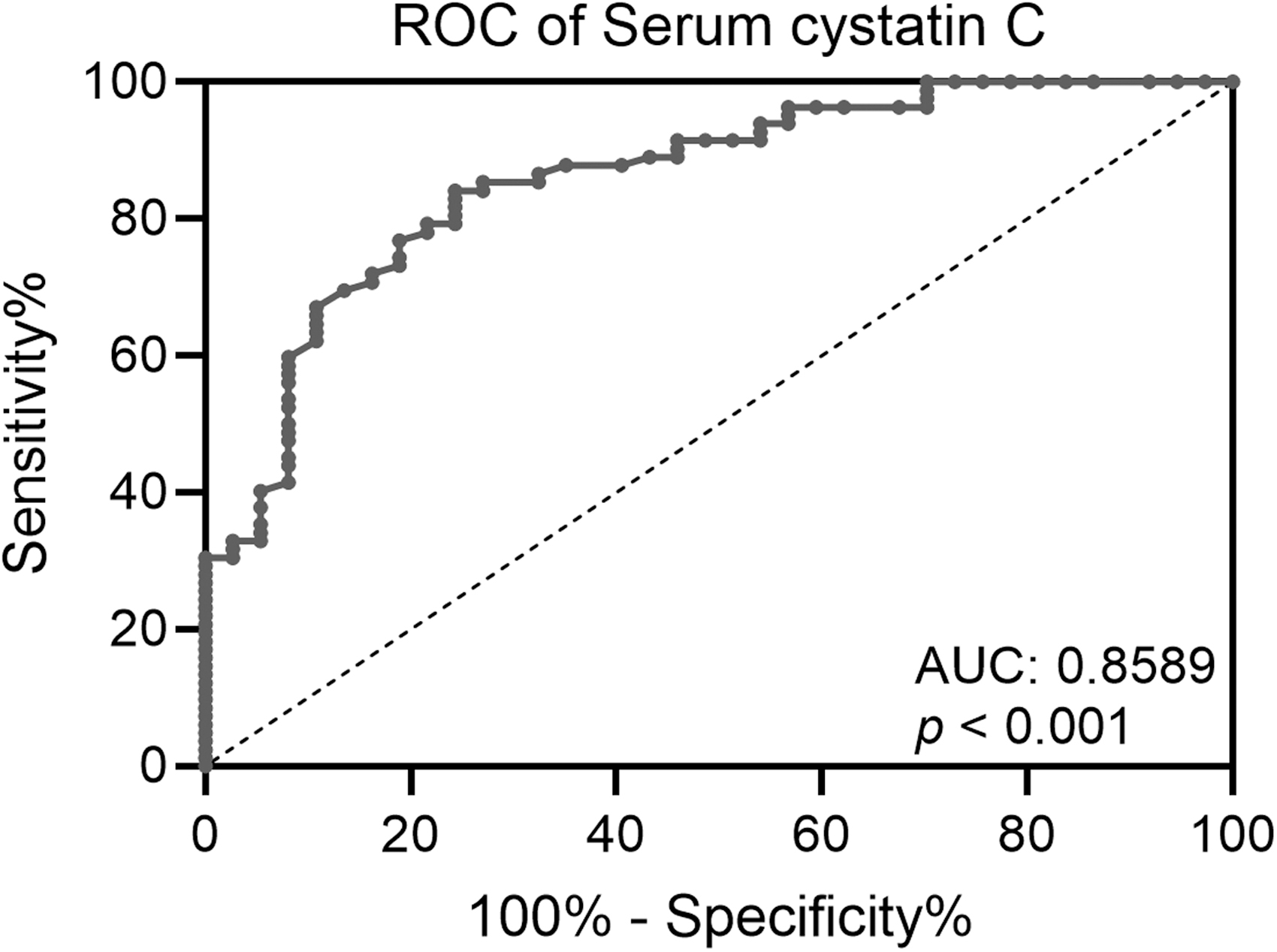
ROC analysis of serum Cys C in GRI. ROC, receiver operating characteristic.
Discussion
The incidence of gout has recently increased significantly among the Chinese population (Luo and others 2018). In patient with blood uric acid level >420 μM/L, the incidence of gout is significantly increased (Ruoff and Edwards 2016). Chronic cases of gout can cause different degrees of kidney damage. However, there is still controversy whether kidney damage is caused by complex factors, including therapeutic drugs, insulin resistance, hormonal changes, and untreated high blood pressure, or by excessive deposition in kidney tissues that causes kidney damage, cell death, and tissue hypoxia (Jaffe and others 2019). The early stage of kidney injury can be characterized by slow progress and no significant symptoms, which is usually difficult to be diagnosed in clinic and hence easily ignored (Yoon and others 2013). However, early detection of kidney damage in patients with gout and the performance of active intervention can not only prevent and alleviate the deterioration of renal functions, but also significantly improve the quality of life of patients (Fei and others 2019). Currently, changes in GFR are mainly used as a clinical indicator of early renal function damage, but this method is limited by its poor sensitivity (Murty and others 2013). GFR is evaluated through creatinine clearance, but changes in serum creatinine level can only be detected when GFR is dropped to less than half of healthy level (Hoste and others 2015). At the same time, different detection schemes and endogenous factors can also affect its accuracy, while renal biopsy is affected by its invasive nature and cannot be widely performed. Therefore, finding sensitive indicators to monitor early renal dysfunction of gout patients has a significant effect on the early treatment of renal dysfunction and prognosis of patients.
As a type of low-molecular-weight protein, Cys C is mainly expressed and secreted in body fluids and tissues. Its biochemical effect is achieved mainly through inhibiting cysteine proteases (Tramonti and others 2012). In recent years, researchers reported that Cys C can sensitively reflect changes in GFR, and it is stably expressed in the human body while not being susceptible to hemolysis, bilirubin, or inflammation (Beetham and others 2018). The filtration of Cys C in the circulation is mainly completed by the glomerulus, whereas its catabolism is completed by the proximal renal tubular epithelial cells and cannot be reabsorbed by the renal tubules (Bjork and others 2018). Therefore, the filtration function of the glomerulus has a significant impact on the level of Cys C. In addition, Cys C is positively charged and has a larger molecular weight than serum creatinine, making it easily for Cys C to be filtered by the glomerulus (Filler and others 1999). The permeability change in the glomerular filtration membrane can be indicated by Cys C, which is a good indicator of changed GFR (van Echteld and others 2014).
Since the body's glomerular filtration function can be reflected by Cys C, it is speculated that Cys C can be used to evaluate early renal function damage. Since 1985, serum Cys C has been considered a GFR indicator (Simonsen and others 1985). Furthermore, the GFR indicator function of Cys C has been suggested in several systemic diseases, such as coronary vascular disease, hypertensive nephropathy, type 2 diabetic nephropathy, and solid organ transplantation (Mussap and others 2002; Artunc and others 2005; Ozer and others 2005; Ling and others 2008). There are some studies demonstrating that serum Cys C is a renal function marker in rheumatic diseases (Bokarewa and others 2007). Many studies have compared the diagnostic accuracy of serum Cys C and creatinine levels in clinical situations (Zahran and others 2007). Although serum creatinine is a widely used renal function marker, it is unreliable due to the effects of age, gender, muscle mass, and abnormal renal tubular regulation. Compared with creatinine, Cys C has some advantages, because serum Cys C level is not affected by these factors (Herget-Rosenthal and others 2007). Therefore, many researchers prefer serum Cys C over serum creatinine as the GFR indicator (Dharnidharka and others 2002). A recent study found that the diagnostic accuracy of serum Cys C level was better than serum creatinine using the ROC curve (Choe and others 2010). Although the research analyzed the significance of serum Cys C in the diagnosis of renal injury in patients with gout, it was limited to male patients, and it did not analyze the relationship between serum Cys C and other indicators, or the degree of gout-associated renal injury. Another research also reported that serum Cys C has a certain clinical significance for the diagnosis of early renal injury in patients with gout (Zhang and others 2019).
Based on the above reports, this research aimed to classify the patients with gout and kidney injury, and then investigate the relationship between serum Cys C and general renal injury indicators, to reveal its diagnostic significance. In this research, the degree of gout-associated renal injury was evaluated by creatinine clearance, based on which all gout patients in this research were divided into 4 different groups: GRI-0, GRI-I, GRI-II, and GRI-III. The results of Spearman's correlation demonstrated that creatinine clearance showed a negative correlation with serum Cys C level. Thus, an increased serum Cys C level indicated elevated severity of renal injury in gout patients. We also analyzed 3 different indexes of renal injury: BUN, serum creatinine, and serum uric acid. In GRI, the levels of BUN, serum creatinine, serum uric acid, and serum Cys C were all increased with elevated severity of renal injury. Thus, the level of serum Cys C exhibited positive correlations with these renal injury indexes. Finally, we evaluated the diagnostic accuracy of serum Cys C through ROC analysis. The results showed that Cys C displayed certain specificity and sensitivity in the diagnosis of early renal dysfunction in patients with gout, demonstrating a potential clinical value.
Evidence has demonstrated that Cys C is associated with various immune responses in inflammatory autoimmune diseases and various tumors (Zi and Xu 2018). Besides, for the measurement of GFR, the serum level of Cys C may have more clinical implications in GRI. It has been reported that cathepsin B and Cys C have positive correlations with inflammation markers in gout patients, such as leukocytes, matrix metalloproteinase (MMP)-9, and the plasminogen activator (PA)/plasmin system (Chu and others 2010). During the pathogenesis of gout, the PA/plasmin system plays a crucial function in the activation of latent MMPs and the control of matrix degradation (Mazzieri and others 1997; Daci and others 1999).
Gout, the most prevalent inflammatory arthritis worldwide, triggers the release of IL-1β and cathepsin B inflammatory mediators that constitute the hallmark of the disease. When cells are stimulated by danger signals or microbes, the inflammasomes are assembled in the cytosol (Martinon and others 2009; Horvath and others 2011). Monosodium urate/uric acid (MSU) is crystallized from uric acid released by injured cells (Shi and others 2003). The activation of nucleotide-binding oligomerization domain, leucine-rich repeat-, and pyrin domain-containing 3 (NLRP3) inflammasomes by the MSU crystals deposited in joint tissues is attributed to the pathogenesis of gout (Chen and others 2006; Martinon and others 2006). The abnormal inflammasome activation causes the enhanced release of IL-1β, leading to pathogenic inflammation. Thus, the inhibition of IL-1β is an effective treatment for acute gout (So and others 2010).
Cathepsin B is an intracellular cysteine protease, mainly localized in the lysosomes (Wu and others 2015). The destabilization and rupture of lysosomes are related to the internalized MSU crystals, causing the release of lysosomal proteases and cathepsins (Guo and others 2015). Previous research has shown that the release of cathepsin B from lysosomes participates in the activation of NLRP3 inflammasomes and the production of IL-1β (Orlowski and others 2015; Campden and Zhang 2019). In this research, we demonstrated that serum IL-1β concentration was positively correlated with serum Cys C in GRI, and revealed a positive correlation between serum Cys C level and the severity of renal injury in gout patients. Since Cys C plays a pathogenic part in GRI, it can be considered a potential therapeutic target.
Conclusion
In conclusion, this research demonstrates that serum Cys C level is a precise marker for GFR and renal damage evaluation, and shows a significant diagnostic value for renal injury in patients with gout.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
Supplementary Figure S1