
Abstract
Cytokine release syndrome (CRS) is the most common on-target toxicity of chimeric antigen receptor (CAR) T cell therapy. However, the prognostic significance of CRS has not been well elucidated. The aim of our study was to evaluate the association between CRS and efficacy after anti-CD19 CAR-T therapy in a retrospective cohort of 22 patients with relapsed/refractory B cell hematological malignancies. The complete remission (CR) rates after CAR-T therapy were 68%, and median value for progression-free survival (PFS) was 6.8 months. Eight of 22 (36.4%) patients showed ≥ grade 2 CRS. Statistical analysis found that patients with ≥ grade 2 CRS had higher CR rates and longer PFS than those with < grade 2 CRS. Moreover, bridging hematopoietic stem cell transplantation was another independent predictor for PFS. These data suggested that appropriate CRS may be beneficial to the efficacy of CAR-T therapy. The Clinical Trial Registration number is NCT03110640, NCT03302403.
Introduction
Although therapeutic advances have considerably improved survival for patients with B cell hematological malignancies in the past decades, about 20%–30% of these patients still relapse and become refractory. Prognoses for these patients remain very poor; only 30%–40% can respond to salvage chemotherapy (Kantarjian and others 2010; Gokbuget and others 2012; Crump and others 2017). Therefore, there is an urgent need for more effective treatments for patients with relapsed/refractory (r/r) B cell hematological malignancies, in which anti-CD19 chimeric antigen receptor (CAR) T cell therapy is proposed as a potential solution, with high response rates of ∼80%–90% (Neelapu and others 2017; Maude and others 2018; Park and others 2018; Locke and others 2019). Recently, Food and Drug Administration approved 4 anti-CD19 CAR-T cells for the treatment of r/r B cell acute lymphoblastic leukemia (B-ALL) and non-Hodgkin lymphoma (B-NHL), including Lisocabtagene maraleucel (Abramson and others 2020), Brexucabtagene autoleucel (Wang and others 2020), Tisagenlecleucel (Maude and others 2018), and Axicabtagene ciloleucel (Neelapu and others 2017), which paved the way for the wider clinical application of CAR-T therapy. However, factors associated with complete and durable remissions after anti-CD19 CAR-T therapy for r/r B cell hematological malignancies have not been well characterized.
Cytokine release syndrome (CRS), the most common toxicity of CAR-T therapy, is a systemic hyperinflammatory response initiated by CAR-T cell activation and characterized by fever and hypotension. In addition, hypoxia, capillary leak, coagulation disorders, and organ dysfunction have also been reported in severe CRS (Lee and others 2014; Brudno and Kochenderfer 2016). It is established that the CRS is an on-target toxic effect, which reminds us that, besides safety, the CRS may also be related to the efficacy of CAR-T therapy (June and Sadelain 2018). Nowadays, most reports focus on the effect of CRS on safety after CAR-T therapy. In our study, we aimed to analyze the prognostic significance of CRS in patients with r/r B cell hematological malignancies treated with anti-CD19 CAR-T cells.
Materials and Methods
Patients
We retrospectively researched 22 r/r B-ALL and B-NHL patients, who treated with anti-CD19 CAR-T therapy between December 2016 and May 2020 at The First Affiliated Hospital of Wenzhou Medical University. All enrolled patients had primary refractory disease after at least 2 lines of therapy or relapsed disease. The anti-CD19 CAR-T cells were administrated after the lymphodepletion chemotherapy with fludarabine and cyclophosphamide (FC) regimen (fludarabine 25–30 mg/m2 on day −4 to −2, cyclophosphamide 500 mg/m2 on day −4 to −3). The CAR used in our study included an anti-CD19 single-chain variable fragment, 4–1BB co-stimulatory domain, and CD3ζ T cell activation domain (HRAIN Biotechnology and CARSGEN Therapeutic, Shanghai, China). The study was approved by the ethics committee of the First Hospital Affiliated of Wenzhou Medical University and performed in accordance with the tenets of Helsinki Declaration, and written informed consent was provided by all participants. The Clinical Trial Registration number is NCT03110640, NCT03302403.
Toxicity and efficacy assessment
After CAR-T cell infusion, the patients' physical condition was closely monitored within 14 days. On days 1, 3, 5, 7, 10, 14, 21, and 28, the peripheral blood was drawn for the assessment of circulating CAR-T cell and cytokine levels. From day 29 to 6 months postinfusion, the CAR-T cell level and treatment response were assessed monthly. After 6 months, the follow-up is performed at an interval of 3 months. Thereinto, the treatment response of NHL was assessed by computed tomography (CT) and positron emission tomography/computed tomography (PET/CT). CRS and neurotoxicity were diagnosed and graded according to the American Society for Transplantation and Cellular Therapy (ASTCT) consensus grading system (Lee and others 2019). The treatment response and remission status were assessed according to the National Comprehensive Cancer Network 2019 guidelines (Brown and others 2019) and Lugano 2014 classification (Cheson and others 2014) for ALL and NHL, respectively. During follow-up, if the patient has any suspicious symptoms of relapse, the efficacy evaluation was immediately taken.
Statistical analyses
Statistical analysis was performed using SPSS version 25.0 (IBM Corp, Armonk, NY). Comparisons of categorical variable and continuous variable were made with the use of the Fisher's exact test and Wilcoxon rank-sum test, respectively. Progression-free survival (PFS) was defined as the time from CAR-T cell infusion until disease progression or death. PFS was evaluated using Kaplan–Meier curves and compared using the log-rank test. To evaluate independent predictors of PFS, the stepwise forward Cox regression analysis was used. P < 0.05 was considered statistically significant.
Results
Patient characteristics
A total of 12 patients with r/r B-ALL and 10 patients with r/r B-NHL (9 cases of diffuse large B cell lymphoma and 1 case of follicular lymphoma) received anti-CD19 CAR-T cell infusion. The median age was 44.5 years (16–70 years). Before CAR-T treatment, they had received a median of 10 treatment courses (5–26 treatment courses) and 1 patient with r/r B-NHL who received autologous hematopoietic stem cell transplantation (HSCT) had failed. After CAR-T treatment, 5 patients with ALL had bridged allogeneic HSCT, including 2 cases of sibling HSCT and 3 cases of haploidentical HSCT.
Toxicity
The most common CAR-T treatment-related adverse events observed were CRS and neurotoxicity. Nineteen out of 22 patients (86%) developed different degrees of CRS: 11 cases (50%) of grade 1, 5 cases (23%) of grade 2, 2 cases (9%) of grade 3, and 1 case (4%) of grade 4. Moreover, the serum levels of cytokines were also analyzed. In our study, the elevated cytokines were mainly interleukin (IL)-6 and interferon (IFN)-γ (Fig. 1A, B), so the total peak levels of cytokines were defined as the sum of the highest levels of IL-6 and IFN-γ. As expected, patients with ≥ grade 2 CRS had higher cytokine levels than those with < grade 2 CRS (P = 0.001) (Fig. 1C). About neurotoxicity, 2 cases (9%) showed grade 1 headache and vomiting, 2 cases (9%) showed grade 3 seizures, and 1 case (5%) showed grade 4 persistent seizures. However, no patients died directly from CRS and neurotoxicity.

The cytokines are shown in patients with CRS after CAR T cell therapy.
The patient with grade 4 CRS developed high-grade fever without a documented source of infection on day 6 after CAR-T infusion. On day 9, grade 2 CRS was diagnosed due to fever, hypotension not responsive to intravenous fluids, and increased significantly serum cytokines levels (Lee and others 2019). Thus, the patient was treated with tocilizumab. The next day, hypoxemia occurred and tocilizumab was given again. However, the CRS had not improved on day 11 and the patient developed seizure and more severe hypoxemia that required mechanical ventilation. According to ASTCT consensus grading system (Lee and others 2019), the patient was diagnosed as grade 4 CRS and neurotoxicity and treated with methylprednisolone immediately. Fortunately, the CRS and neurotoxicity were obviously improved on day 14 and then the methylprednisolone was gradually reduced. Moreover, the patient achieved complete remission (CR) on day 28 after CAR-T infusion and her PFS was up to 29.4 months without bridging HSCT (Fig. 1D).
Relationship between CRS and CAR-T cell expansion
All CAR-T cells were derived from recipients, and the median infusion dose was 2.04 × 106/kg (1–12.73 × 106/kg). Twenty-one out of 22 patients (95%) were detected with CAR-T cell expansion (Fig. 2A, B). The median peak time, duration, and peak levels of CAR-T cells were 9 days (3–36 days), 41 days (0–177 days), and 99,350 copies/μg genomic DNA (gDNA) (88–630,000 copies/μg gDNA), respectively. Our results showed that patients ≥ grade 2 CRS had higher peak and area under the curve (AUC) of CAR-T cell levels within the first month (Fig. 2C, D).
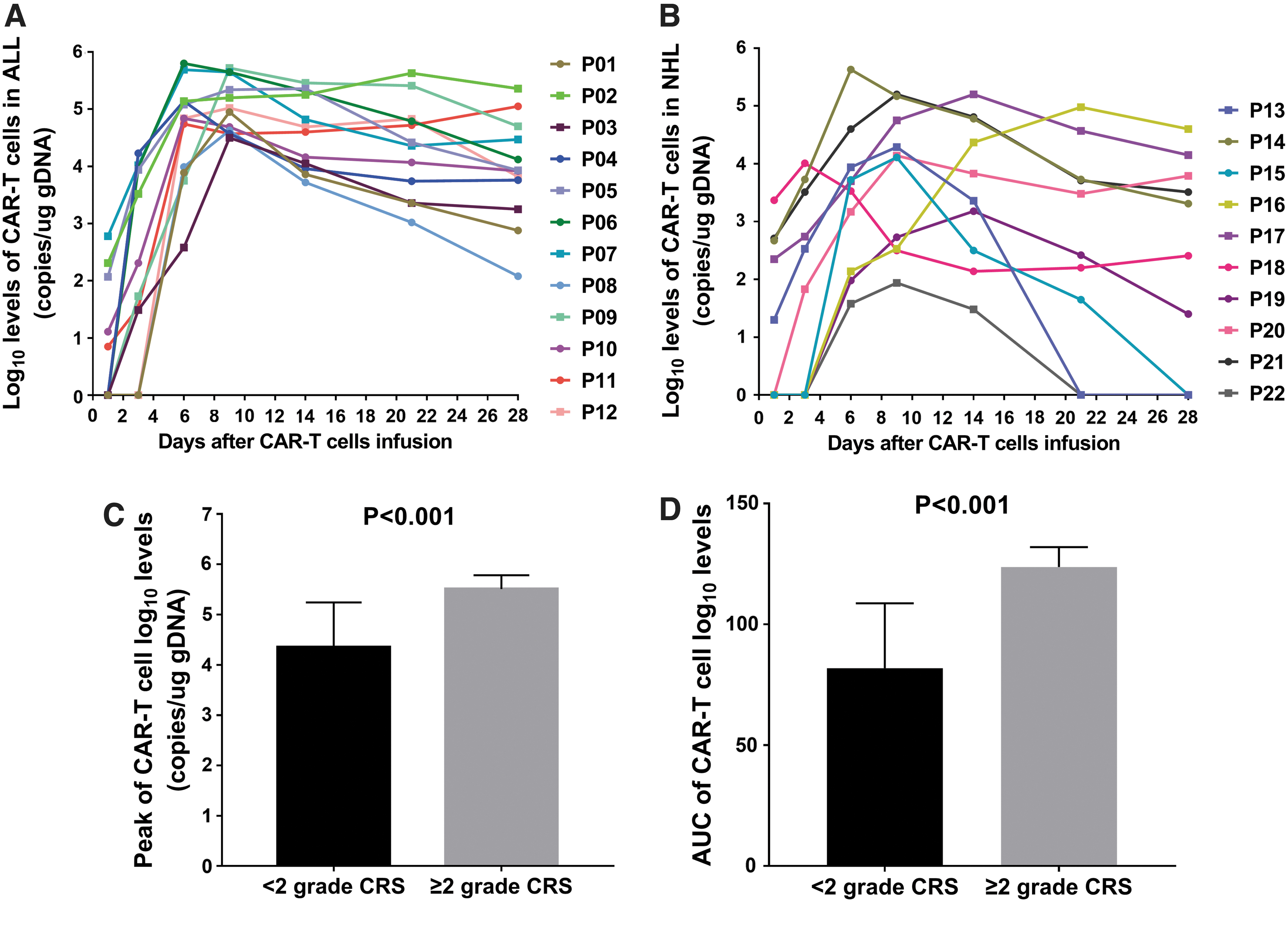
Patients with ≥ grade 2 CRS have higher levels of CAR T cells.
Relationship between CRS and initial response rates
All 22 patients survived for >30 days and were evaluated for response. The overall response rates without additional therapy after CAR-T cell infusion was 82% (18/22), and 68% (15/22) of the patients achieved CR. Further analysis found that patients with ≥ grade 2 CRS exhibited higher CR rates than those with < grade 2 CRS (P = 0.022) (Fig. 3A).
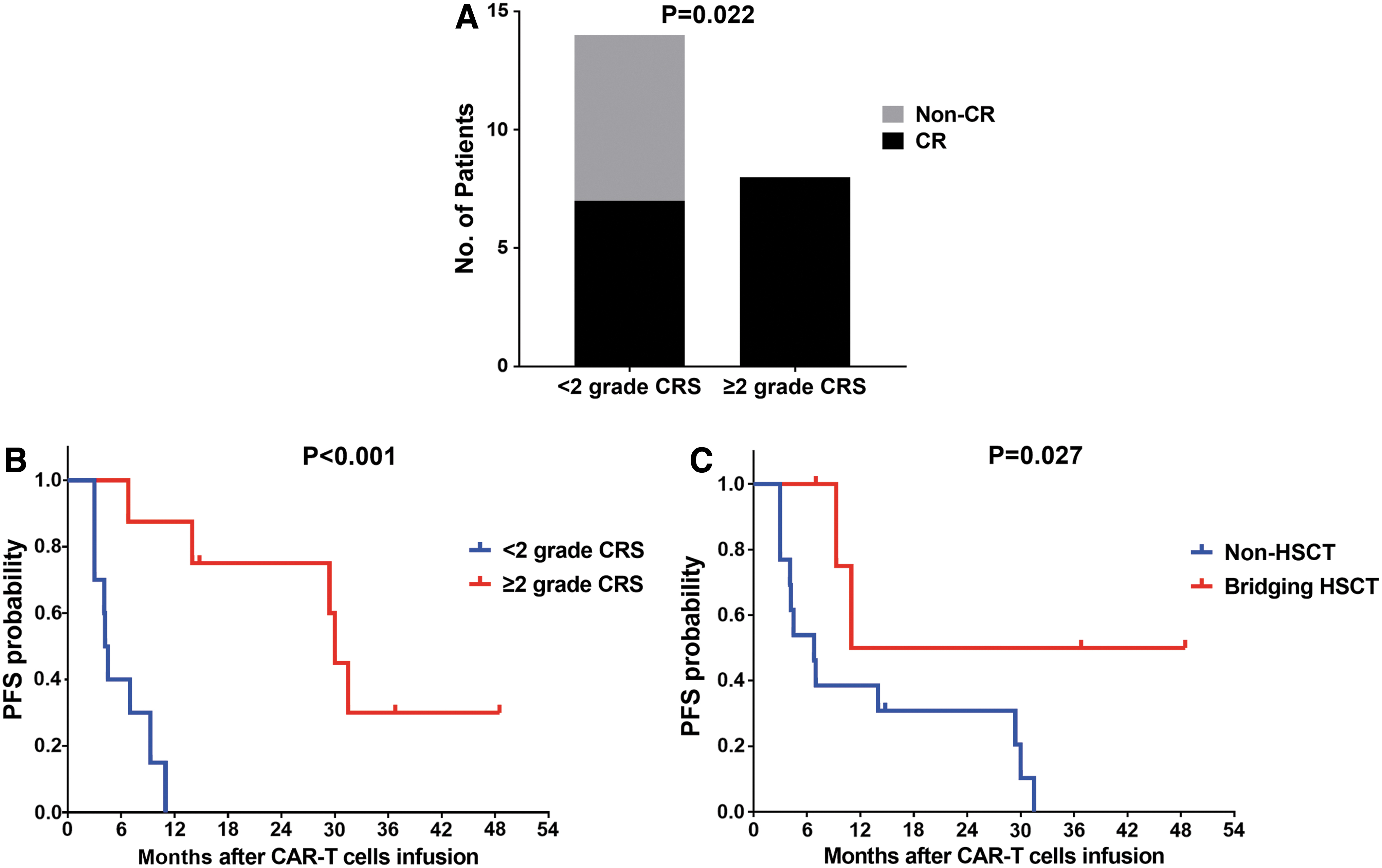
Patients with ≥ grade 2 CRS have better prognosis after CAR T cell therapy.
Relationship between CRS and PFS
With a median follow-up of 36.8 months, median value for PFS was 6.8 months. The rates of PFS at 6 months, 1 year, 2 years, and 3 years after CAR-T infusion were 55% (12/22), 32% (7/22), 23% (5/22), and 9% (2/22), respectively. To explore the relevant factors affecting PFS, we analyzed whether the PFS was related to patient's clinical characteristics, including gender, age, disease type, times of relapse, tumor burden, CAR-T cell dose, CRS grading, peak CAR-T cells, CAR-T cell duration, and bridging HSCT. In univariate analysis, we found that CRS grading (P < 0.001), peak CAR-T cells (P = 0.001), CAR-T cell duration (P = 0.019), and bridging HSCT (P = 0.027) were significantly associated with PFS (Table 1). Multivariable Cox-regression analysis showed that only CRS grading (P = 0.002) and bridging HSCT (P = 0.008) were 2 independent predictors for PFS. Patients with ≥ grade 2 CRS (hazard ratio [HR] = 0.010, 95% confidence interval [CI]: 0.001–0.174) or bridging HSCT (HR = 0.056, 95% CI: 0.007–0.468) had the longer PFS (Table 1; Fig. 3B, C).
Univariate and Multivariable Analyses for Progression-Free Survival
ALL, acute lymphoblastic leukemia; CAR-T, chimeric antigen receptor T; CI, confidence interval; CRS, cytokine release syndrome; HR, hazard ratio; HSCT, hematopoietic stem cell transplantation; NHL, non-Hodgkin lymphoma.
Discussion
Although the association between CRS and safety of CAR-T therapy is well described (Lee and others 2014; Brudno and Kochenderfer 2016), the prognostic significance of CRS remains a matter of discussion. In multiple myeloma, retrospective analysis revealed that CD19, natural-killer group 2 member D (NKG2D) or kappa light chain targeted CAR-T cells have a lower CRS incidence, with these treatments being less effective than B-cell maturation antigen (BCMA) CAR-T cells (Zhou and others 2020), which suggests that CRS may be beneficial to the efficacy of CAR-T therapy. The aim of this study was to clarify the prognostic implication of CRS in r/r B-ALL and B-NHL patients treated with anti-CD19 CAR-T cells. As expected, we found that patients with ≥ grade 2 CRS had higher CR rates and longer PFS than those with < grade 2 CRS. However, due to the limited number of cases in this study, our findings need larger multicenter and prospective studies to further validate.
CRS is a systemic hyperinflammatory response. Indeed, consistent with previous reports (Teachey and others 2016; Lee and others 2019), we found that ≥ grade 2 CRS was associated with significantly increased cytokines levels, mainly including IL-6 and IFN-γ. We know that high-dose cytokines can regulate the host immune response to tumor cell, as well as directly induce cancer cell death, but low-dose cytokines has no significant therapeutic effect (Chulpanova and others 2020). Moreover, Kochenderfer and others (2017) and Fraietta and others (2018) demonstrated that the patients with CR had significantly higher levels of cytokines than those with partial remission and nonremission after anti-CD19 CAR-T therapy. Thus, a putative mechanism by which ≥ grade 2 CRS improves CAR-T cell efficacy may be that significantly increased cytokines can help to induce deeper remissions in r/r B cell hematological malignancies patients. We noticed that CRS is not unique to CAR-T therapy and often occurs with other conditions, including severe acute respiratory syndrome coronavirus 2 infection (COVID-19) (Moore and June 2020). A recent report showed that the patient with Hodgkin lymphoma experienced spontaneous remission after SARS-CoV-2 infection, which may be the result of the tumor killing of cytokines produced in response to infection (Challenor and Tucker 2021). Another report described that the patient who experienced spontaneous regression of high-grade B-NHL may also be due to the infection-induced cytokines release (Buckner and others 2012). These findings are in agreement with our earlier speculation. Moreover, consistent with previous clinical trials (Neelapu and others 2017; Park and others 2018), we found that ≥ grade 2 CRS was significantly associated with high peak and AUC of CAR-T cell levels within the first month, which may be another possible explanation of the relation between ≥ grade 2 CRS and better prognosis.
Considering HSCT is a standard therapy for patients with r/r hematological malignancies (Duarte and others 2019), we also evaluated the effect of bridging HSCT on PFS after CAR-T therapy. Consistent with the study of Hay and others (2019), we found that bridging HSCT was associated with longer PFS. Conversely, Park and others (2018) demonstrated that bridging HSCT had no significant effect on PFS. In other words, whether bridging HSCT could further improve PFS after CAR-T therapy is controversial. Our study suggested that CAR-T bridging to allo-HSCT can be considered for eligible patients.
Conclusion
We found that patients with ≥ grade 2 CRS had better prognosis after CAR-T therapy, which reminds clinicians that, to balance safety and efficacy, we should appropriately control CRS after CAR-T therapy instead of pursuing the lowest severity of CRS or even eliminating CRS.
Footnotes
Authors' Contributions
R.D. and S.Z. conducted the study, provided patient care, analyzed the data, and wrote the article. S.J., Y.C., Y.M., L.S., and C.X. participated in the clinical care and analyzed the data. K.Y. conceived of the study, participated in the clinical care, supervised the research, and reviewed the article. All authors read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the grant of Wenzhou Municipal Science and Technology Bureau (No. 2018ZY014), Zhejiang Provincial Natural Science Foundation of China (No. LY20H080005), and the Start-up Funding for PhD of The First Affiliated Hospital of Wenzhou Medical University (No. 2018QD009).