
Abstract
Rheumatoid arthritis (RA) is a chronic incurable inflammatory autoimmune disease. T follicular helper (Tfh) cells expressing different markers play critical roles in the development of RA. However, their specific mechanisms of action and association with RA clinical parameters are not clear. We therefore performed a cohort study to investigate the effects of different Tfh cell markers on RA pathogenesis. We retrospectively reviewed clinical data from 30 patients diagnosed with RA and 30 healthy controls (HCs) who visited our hospital. Based on X-ray findings, the patients were divided into a joint bone erosion group (n = 17) and a non-erosive joint bone group (n = 13). Using flow cytometry, we determined the frequencies of five peripheral blood CD4+ Tfh cell types characterized by different markers, and examined these cell types for correlations with clinical parameters. RA patients exhibited higher frequencies of CD4+CXCR5+, CD4+CXCR5+ICOS+, CD4+CXCR5+OX40+, and CD4+CXCR5+CD40L+ Tfh cells than HCs. CD4+CXCR5+, CD4+CXCR5+CD40L+, and CD4+CXCR5+OX40+ Tfh cell frequencies positively correlated with disease activity score-28 with erythrocyte sedimentation rate (DAS28-ESR), while those of CD4+CXCR5+ and CD4+CXCR5+CD40L+ Tfh cells were related to rheumatoid factor (RF) and anti-cyclic citrullinated peptide (CCP) antibodies. In RA patients without joint bone erosion, CD4+CXCR5+CD40L+ Tfh cell frequencies were positively correlated with both RF and DAS28-ESR. Serum anti-CCP antibody levels and CD4+CXCR5+ICOS+ Tfh cell frequencies were also positively correlated. Circulating CD4+CXCR5+CD40L+ Tfh cells appear to play critical roles in RA pathogenesis, and restricting CD4+CXCR5+CD40L+ Tfh cells may be a therapeutic strategy for controlling RA.
Introduction
Rheumatoid arthritis (RA) is a chronic inflammatory disease characterized by autoimmunity that triggers chronic joint inflammation and tissue destruction (Gadeval and others 2021). The prevalence of RA has been increasing annually, and its global prevalence currently reaches up to 0.5%–1% in adults, incurring a considerable burden on health care systems globally. RA develops following autoantibody production, including rheumatoid factor (RF) and anti-cyclic citrullinated peptide (CCP) antibodies, which are associated with disease activity and bone destruction (Bugatti and others 2016; Conigliaro and others 2016).
RA is commonly treated with disease-modifying antirheumatic drugs (DMARDs), glucocorticoids, nonsteroidal anti-inflammatory drugs (NSAIDs), or surgery; however, none of these treatments can result in a complete cure of RA, and only help to relieve pain, reduce joint inflammation, and prevent joint destruction.
At present, abnormal activation of CD4+ T cells and T cell-dependent B cells is considered to be the main cause of RA, and therefore, regulating cellular immunity has emerged as a potential treatment strategy (Chemin and others 2019).
T follicular helper (Tfh) cells, a novel CD4+T subset, can stimulate B cell differentiation to generate germinal centers (GCs), which play key roles in the maturation and proliferation of B cells and in promoting antibody production (Zhu and others 2016). The immunoregulatory molecules C-X-chemokine receptor type 5 (CXCR5), inducible T cell co-stimulator (ICOS), programmed death-1 (PD-1), CD40 ligand (CD40L), and OX40 play crucial roles in this process (Lu and others 2021). Tfh cell imbalance is observed in various systemic autoimmune diseases. We previously reported that the frequency of circular Tfh cells was elevated in RA patients, indicating that Tfh cells are associated with the pathogenesis of RA (Xu and others 2020). However, the specific mechanism of action of Tfh cells in RA is not clear, and the association between specific Tfh cell markers and RA clinical parameters has not been reported.
The objective of this retrospective observational study was to measure the levels of different circulating Tfh (cTfh) cell markers in RA patients, and to investigate their relationship with disease activity, autoantibody production, and joint bone erosion. We further aimed to determine the most critical Tfh cell marker in RA pathogenesis.
Materials and Methods
Patients and controls
The clinical data of 30 patients diagnosed with RA at the Department of Rheumatology and Immunology of the China-Japan Union Hospital of Jilin University were retrospectively reviewed.
The eligibility criteria were as follows: (1) adult patients (>18 years); (2) RA diagnosis based on the 1987 revised criteria of the American College of Rheumatology (Arnett and others 1988); and (3) use of glucocorticoids (the equivalent of prednisone ≤10 mg/day), NSAIDs, and/or DMARDs. The exclusion criteria were as follows: (1) renal or hepatic disorders; (2) significant infections; (3) tumors or other rheumatic diseases aside from RA; (4) pregnant women; and (5) RA patients with a history of biological therapy or high-dose glucocorticoids (equivalent to >10 mg/day prednisone) within 6 months of the study. The detailed clinical characteristics and laboratory features of the included patients with RA are shown in Table 1. We also selected 30 age- and sex-matched healthy controls (HCs) for comparison.
Clinical and Laboratory Parameters in Rheumatoid Arthritis Patients and Healthy Control Participants
Normally distributed data are shown as the mean ± SD, other continuous variables are shown as the median (IQR).
Anti-CCP, anti-cyclic citrullinated peptide; CRP, C-reactive protein; DAS28 (ESR), disease activity score with 28 joints using ESR (Prevoo and others 1995); ESR, erythrocyte sedimentation rate; HC, healthy control; IQR, interquartile range; RA, rheumatoid arthritis; RF, rheumatoid factor; SD, standard deviation.
The institutional review boards of the China-Japan Union Hospital reviewed the study and approved the protocol. Informed consent was obtained from all patients and volunteers Registration number (2018011501).
Clinical data and laboratory tests analysis
All patients with RA were followed up to obtain clinical data (Table 1). Serum RF and C-reactive protein (CRP) levels were determined using immunoturbidimetry. Their erythrocyte sedimentation rates (ESRs) were measured using the Westergren method, and the levels of serum anti-CCP antibodies were detected using commercial enzyme-linked immunosorbent assays. The disease activity score-28 with ESR (DAS28-ESR) was calculated (Prevoo and others 1995).
To analyze the effects of Tfh cells on joint bone erosion, the included RA patients were divided into a joint bone erosion group (n = 17) and a nonerosive joint bone group (n = 13) based on their plain X-rays.
Sample collection
For Tfh cell testing, peripheral blood mononuclear cells (PBMCs) were isolated from blood samples collected from all participants using Ficoll® density gradient centrifugation. PBMCs were washed and resuspended in phosphate-buffered saline (PBS) containing 5% fetal bovine serum. The purity of the cell preparations was analyzed using flow cytometry.
Flow cytometry
For flow cytometry, blood samples were stored in tubes containing heparin sodium and examined within 4 h of collection. PBMCs were isolated as described above, and reacted with the following anti-human monoclonal antibodies: peridinin-chlorophyll-protein (PerCP)-conjugated anti-CD4, allophycocyanin-conjugated anti-CXCR5, P-phycoerythrin-conjugated anti-ICOS, PerCP-conjugated anti-PD-1, fluorescein isothiocyanate (FITC)-conjugated anti-CD40L, and FITC-conjugated anti-OX40 (all from eBioscience, Inc., San Diego, CA). The cells were assessed, and the frequencies of CD4+CXCR5+, CD4+CXCR5+ICOS+, CD4+CXCR5+OX40+, CD4+CXCR5+PD1+, and CD4+CXCR5+CD40L+ Tfh cells were recorded.
Briefly, the cells were resuspended in 100 μL PBS and incubated in the dark at 25°C for 30 min with the corresponding monoclonal antibodies. These were then washed twice with PBS, and the samples were analyzed using a flow cytometer (FACSCanto II; BD Bioscience, Franklin Lakes, NJ). All staining was performed according to the manufacturer's protocol, the same gates were applied to all samples, and each sample was run separately.
Statistical analysis
Statistical analyses were performed using Statistical Package for the Social Sciences (version 24.0; SPSS®, Chicago, IL). Data are summarized as median and range for non-normally distributed data or as mean ± standard deviation for normally distributed data. Statistical significance between groups was determined using the Mann–Whitney U-test, Wilcoxon signed-rank test, and Student's t-test, as appropriate. Pearson's correlation analysis and Spearman rank correlation analysis were used for analyzing associations between the variables. GraphPad Prism® (version 7.0; GraphPad Software, Inc., San Diego, CA) was used for figure production. Statistical significance was set at P < 0.05.
Results
Increased frequencies of peripheral blood Tfh cells in RA patients
The characteristics of study participants are summarized in Table 1. We examined peripheral blood CD4+CXCR5+, CD4+CXCR5+ICOS+, CD4+CXCR5+PD1+, CD4+CXCR5+OX40+, and CD4+CXCR5+CD40L+ Tfh cell frequencies in RA patients (n = 30) and age-matched HCs (n = 30) using flow cytometry. The frequencies of CD4+CXCR5+ (P = 0.028), CD4+CXCR5+ICOS+ (P < 0.001), CD4+CXCR5+CD40L+ (P < 0.001), and CD4+CXCR5+OX40+ (P < 0.001) Tfh cells in RA patients were significantly higher than those in the HCs (Fig. 1A–D). However, the frequency of CD4+CXCR5+PD1+ Tfh cells in peripheral blood of RA patients was not significantly higher than that in HCs (P = 0.115) (Fig. 1E).
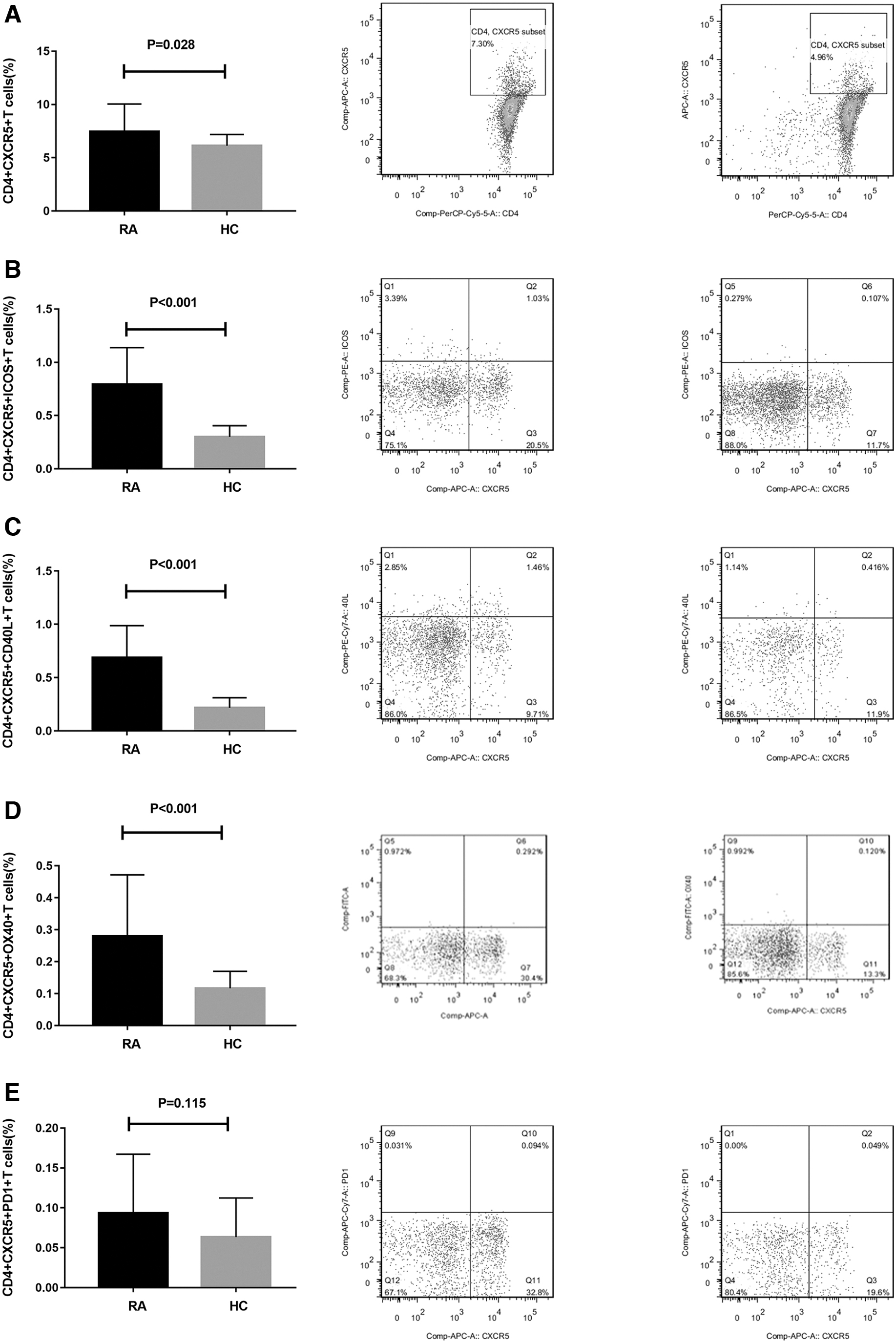
Tfh cell markers in peripheral blood of RA patients and HCs. We measured peripheral blood Tfh cell frequencies in RA patients (n = 30) and age-matched HCs (n = 30) by flow cytometry.
Positive correlations between peripheral blood Tfh cell frequencies and disease activity in RA patients
To analyze the potential role of different Tfh cell markers in RA patients, we measured the correlation between the different Tfh cell marker subtype frequencies and the clinical parameters of RA patients. The frequencies of CD4+CXCR5+ (r = 0.533, P = 0.002), CD4+CXCR5+CD40L+ (r = 0.440, P = 0.015), and CD4+ CXCR5+OX40+ (r = 0.594, P = 0.001) Tfh cells in RA patients were positively correlated with the disease activity index DAS28-ESR (Fig. 2A–C). However, there was no significant association between the other subtypes of Tfh cells and disease activity in RA patients (Fig. 2D, E). These data suggest that CXCR5, OX40, and CD40L contribute to the occurrence and development of RA by influencing its disease activity.
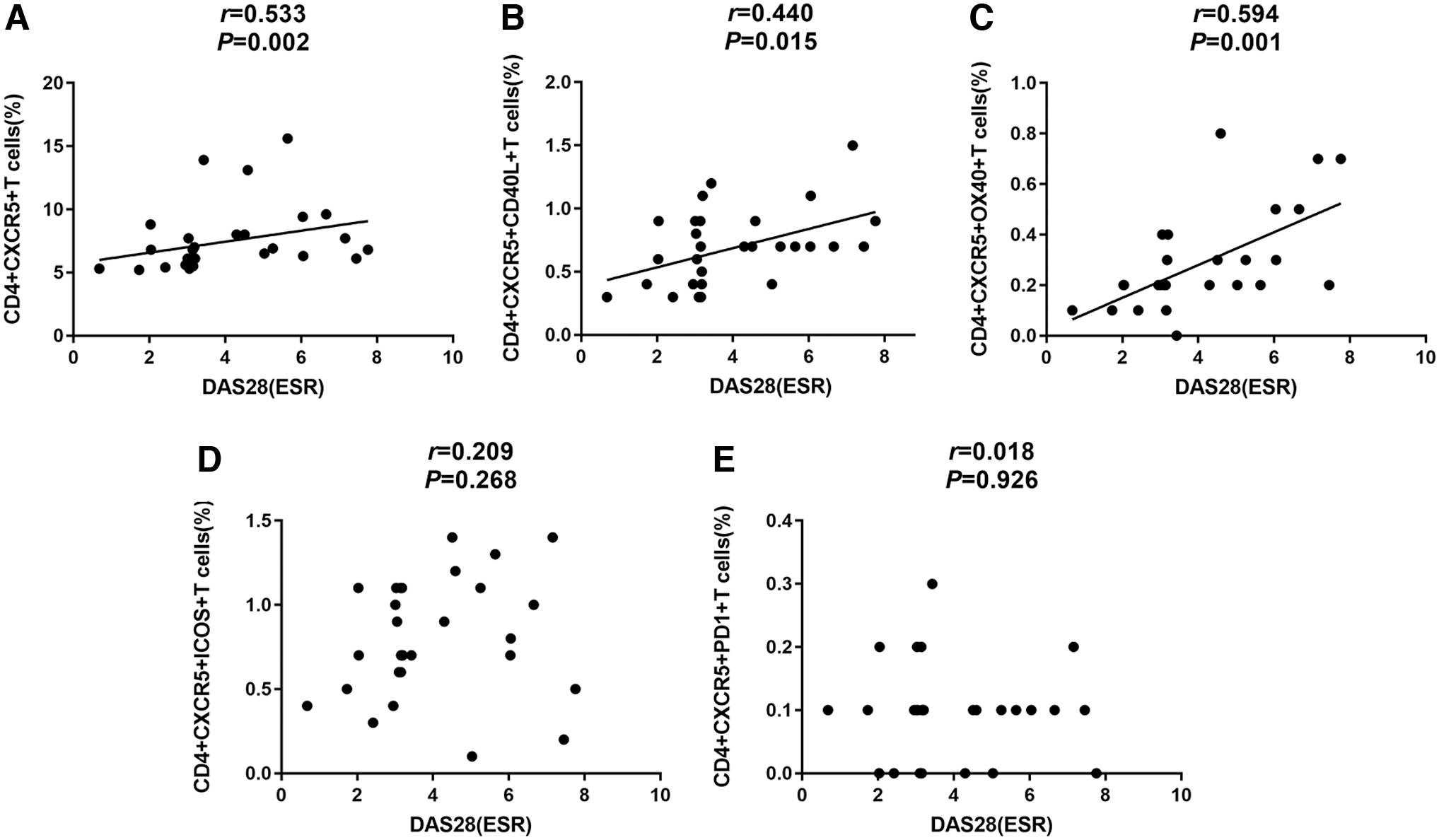
Positive correlations between circulating Tfh cell marker frequencies and disease activity in RA patients.
High levels of autoantibodies and increased frequencies of peripheral blood Tfh cells in RA patients
Previous studies have shown that RA autoantibody production is directly linked to inflammation and pain (Fang and others 2019). To analyze the association between autoantibodies (anti-CCP antibodies and RF) and peripheral blood Tfh cells, we compared the frequencies of different Tfh cell marker subtypes and the levels of autoantibodies in RA patients. The frequencies of CD4+CXCR5+ (r = 0.406, P = 0.026) and CD4+CXCR5+CD40L+ (r = 0.429, P = 0.018) Tfh cells were positively correlated with anti-CCP antibodies (Fig. 3A, B), whereas there was no significant association between other Tfh cell marker subtype frequencies and anti-CCP antibodies (Fig. 3C).

Correlation of peripheral blood Tfh cell marker frequencies and autoantibodies production in RA patients.
Furthermore, CD4+CXCR5+ (r = 0.453, P = 0.012) and CD4+CXCR5+CD40L+ (r = 0.423, P = 0.020) Tfh cell frequencies were also positively correlated with RF (Fig. 3D, E), whereas there was no significant association between other Tfh cell marker subtype frequencies and RF (Fig. 3F). These data suggest that the markers CXCR5 and CD40L play important roles in the pathogenesis of RA autoantibody production.
Relationship between frequencies of Tfh cell subtypes and joint bone erosion in RA patients
Recently, a direct link has been proposed between autoantibody production and the degree of bone erosion in RA (Fang and others 2019). Therefore, in this study, patients with RA were grouped according to whether they had joint bone erosions according to X-ray findings. We compared the five different Tfh cell subsets between the two groups as shown in Fig. 4, whereas there was no significant difference found between the two groups. In patients without joint bone erosions (n = 13), CD4+CXCR5+CD40L+ Tfh cell frequencies were positively correlated with the presence of RF (r = 0.512, P = 0.009; Fig. 5A) and DAS28-ESR (r = 0.617, P = 0.036; Fig. 5B).

Tfh cell markers in peripheral blood of RA patients with joint erosion or not. RA patients were grouped into a joint bone erosion group (n = 17) and a nonerosive joint bone group (n = 13).
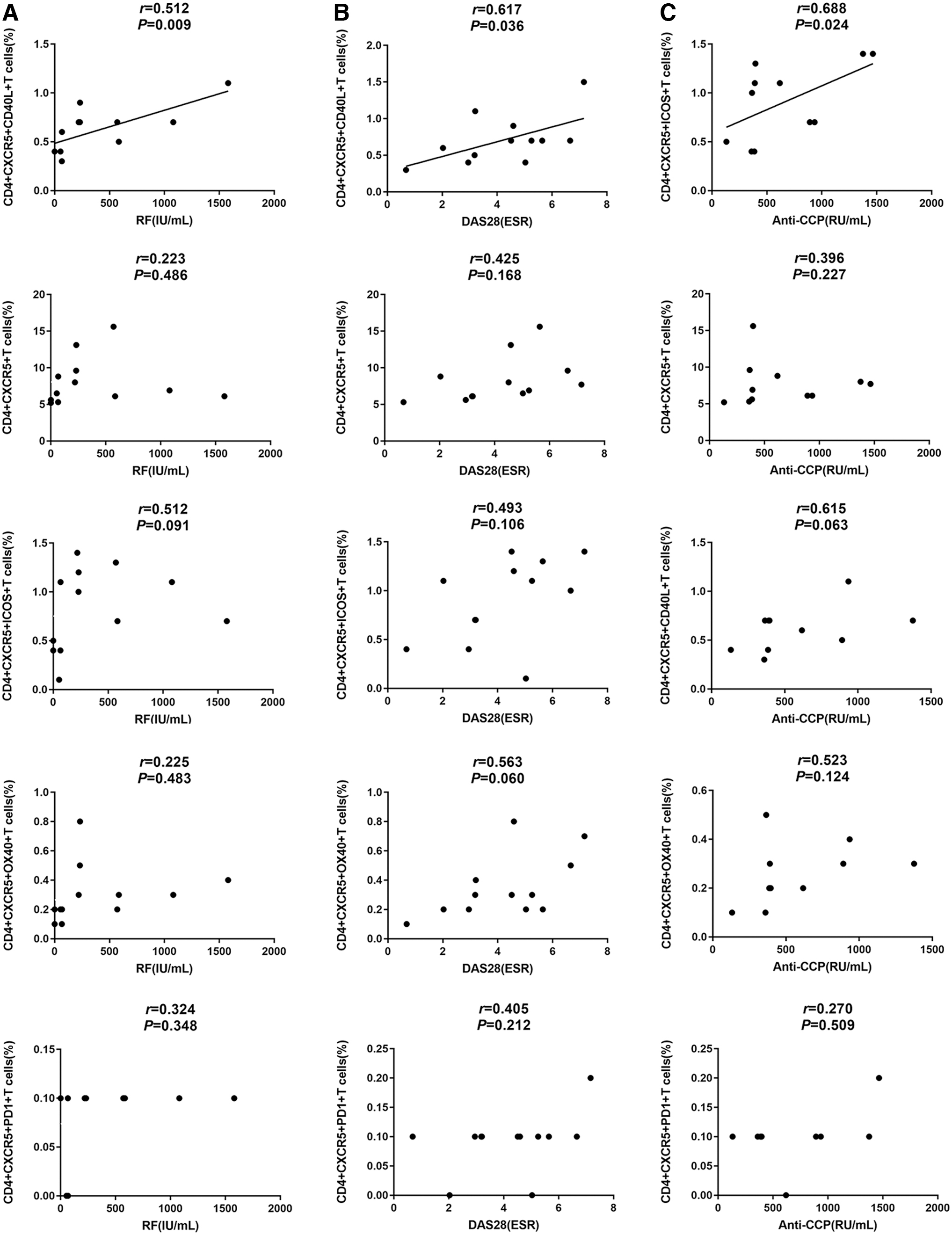
Positive correlation between Tfh cells in RA patients without joint bone erosion. RA patients were grouped into a joint bone erosion group (n = 17) and a nonerosive joint bone group (n = 13).
In addition, serum anti-CCP antibody levels and peripheral blood CD4+CXCR5+ICOS+ Tfh cell frequencies were also positively correlated (r = 0.688, P = 0.024; Fig. 5C). However, in RA patients with joint bone erosions (n = 17), there was no significant association between different Tfh cell marker subtype frequencies and clinical data.
Discussion
In this study, we employed flow cytometry to analyze different Tfh cell marker subtypes in patients with RA. We found that peripheral blood Tfh cell markers CXCR5, ICOS, OX40, and CD40L were imbalanced in RA patients, and that the levels of CXCR5, OX40, and CD40L were related to disease activity. Furthermore, CXCR5 and CD40L levels were correlated with autoantibody production. Importantly, ICOS and CD40L levels were only associated with autoantibody production in RA patients without joint bone erosion, suggesting that blocking these molecules in a timely manner may prevent the progression of RA.
The pathogenesis of RA is still unclear. It is generally believed that RA is related to various immune cells and autoantibodies (Weyand and Goronzy 2021). Tfh cells are a subset of CD4+ T cells that facilitate GC reactions by providing the signals required for antibody production and the generation of long-lived antibody-secreting plasma cells (Lu and others 2021). Previous studies have shown that Tfh cells are involved in the pathogenesis of RA by inducing the proliferation of B lymphocytes in the GCs and producing a large number of anti-CCP antibodies (Ma and others 2012; Wang and others 2018).
Moreover, in our previous study, we found that interleukin (IL)-29 may contribute to RA by inhibiting Tfh cell production by decreasing STAT3 activity and downregulating BCL6 expression, suggesting that Tfh cells affect the development of RA through the IL-29-BCL6-STAT3 pathway (Xu and others 2020). However, Tfh cells express various surface markers with different functions. The specific roles of these markers in RA are not yet understood; thus, it is important to determine the markers that play a major role in the pathogenesis and progression of RA. Toward this end, we aimed to explore the relationship between different Tfh cell marker subtypes and clinical parameters in patients with RA.
We confirmed that Tfh cell frequencies were increased in RA patients compared with those of age- and sex-matched HCs, especially CD4+CXCR5+, CD4+CXCR5+ICOS+, CD4+CXCR5+CD40L+, and CD4+CXCR5+OX40+ Tfh cells. This suggests that CXCR5, ICOS, OX40, and CD40L play important roles in the pathogenesis of RA.
We speculate that this is related to the CXCR5/CXCL13 signaling pathway. A recent study suggested that CXCL13 is a specific ligand of CXCR5 and that it can activate the protein kinase B (AKT) signaling pathway in a CXCR5-dependent manner (Zhao and others 2021). Greisen and others (2014) found that CXCL13 levels in the sera of patients with RA increased significantly and correlation with disease activity. In addition, various inflammatory factors such as IL-6 and tumor necrosis factor-alpha can regulate the participation of serum CXCL13 in the inflammatory response (Lu and others 2021).
Moreover, Tfh cells, which migrate to lymphoid follicles through the chemotactic actor CXCL13, were also found to bind to CD40 on the surface of B lymphocytes to induce CD40-CD40L–dependent B cell activation (Rashu and others 2019). These reports are consistent with our results, which showed that CD4+CXCR5+ and CD4+CXCR5+CD40L+ Tfh cell frequencies were related to disease activity, indicating that CXCR5 and CD40L play significant roles in RA severity and can be considered possible markers of RA clinical activity.
OX40-OX40L signaling can activate the downstream nuclear factor-k-gene binding (NF-κB), phosphatidylinositol 3-kinase (PI3K), and AKT pathways, which can ultimately prolong the survival time of T cells and further enhance the function of effector T cells. Previous studies have shown that OX40L stimulates CD4+ T cell expression of Tfh cell-related molecules and prolongs cell survival, which promotes B lymphocytes to produce more inflammatory factors that aggravate the condition of RA patients (Laustsen and others 2014; Jiang and others 2017). Huang and others (2020) found that OX40 inhibition could reverse the progression of RA by PD-1 blockade. Congruent with other studies, we also showed that OX40 is associated with RA disease activity (Kurata and others 2019).
Autoantibodies, which are secreted by plasma cells after antigen stimulation, are important early indicators of RA (Mustila and others 2011). Several studies have shown that RA patients with positive autoantibodies have more serious conditions, and a high risk of joint damage and disability (Bugatti and others 2016; Conigliaro and others 2016). Orr and others (2017) found that anti-CCP+ RA patients developed more erosions and had higher levels of serum CXCL13, indicating that CXCL13 may promote RA autoantibody production. Importantly, CXCR5 can stimulate the production of CD40L, which binds to CD40 on the surface of B lymphocytes and promotes their maturation by antibody class switching and the development of antigen-specific memory B cells (Rashu and others 2019).
Our previous study showed a positive correlation between peripheral blood CD4+CXCR5+CD40L+ Tfh cell frequencies and serum levels of anti-CCP antibodies in patients with RA (Xu and others 2020). In this study, we also found that CD4+CXCR5+ and CD4+CXCR5+CD40L+ Tfh cell frequencies were related to autoantibody production (RF and anti-CCP), indicating that CXCR5 and CD40L may participate in RA autoantibody production by promoting the maturation of B cells, producing a large number of autoantibodies, and ultimately increasing RA disease activity.
Bone erosion is a hallmark of structural damage in RA (Cipolletta and others 2021). Bugatti and others (2016) suggested that anti-CCP antibodies and high levels of RF are associated with systemic bone loss in patients with early untreated RA. Based on our results, CXCR5 and CD40L are related to autoantibody production. As a previous study showed that RA patients positive for anti-CCP antibodies generally have a high degree of joint damage (Papadopoulos and others 2008), we speculated that Tfh cells may participate in the process of RA joint bone erosion. Therefore, we investigated the relationship between the frequencies of Tfh cell markers and RA joint bone erosion.
We found that in patients without joint bone erosions, CD4+CXCR5+CD40L+ Tfh cell frequencies were positively correlated with RF and DAS28-ESR. In addition, serum anti-CCP antibody levels and peripheral blood CD4+CXCR5+ICOS+ Tfh cell frequencies were positively correlated in these patients. A previous study showed that the ICOS Ligand (ICOSL)/ICOS interaction could enhance the accumulation of CD40L at the Tfh cell synapse, which increases the synapse area.
The resulting feed-forward loop allows for maximal T–B cell entanglement and reduces the CD40L expression threshold required for GC B cell survival and/or selection, which further increases the total GC output CD40L (Papa and others 2017). We believe that this positive feedback is promoted in the process of joint bone erosion. Our results further suggest that CD4+CXCR5+CD40L+ and CD4+CXCR5+ICOS+ Tfh cells may play important roles in the early stages of RA before joint bone destruction. Therefore, the detection of CD4+CXCR5+CD40L+ and CD4+CXCR5+ICOS+ Tfh cells can predict disease activity and may help to prevent RA progression.
PD-1 is an important negative marker of Tfh cells, which negatively regulates the expression of GC-related Tfh cells in reactive lymphoid tissue. Previous studies showed that PD-1 attenuated the normal GC response through PD-1 and PD-L1 interactions, which are required to maintain the stringency of affinity-based selection (Shi and others 2018). However, the specific role of CD4+CXCR5+PD1+ Tfh cells in RA patients is not yet clear. In this study, we found that the frequencies of CD4+CXCR5+PD1+ Tfh cells in peripheral blood of RA patients were not significantly higher than those of HCs, indicating that this subtype does not participate in RA development. However, Cao and others (2019) found that RA patients had more CD4+CXCR5+PD1+ Tfh cells in peripheral blood, which was positively correlated with ESR, RF, CRP, and anti-CCP antibodies.
This discrepant result may be related to the fact that the patients in the Cao and others' (2019) study had new-onset RA (disease duration <6 months), whereas we included patients with a broader disease duration spectrum. In addition, individual differences among RA patients may account for these conflicting findings. Thus, the results require confirmation in studies with larger sample sizes. Moreover, the effects of different drugs on Tfh cell markers require further study.
This study offers new insights into the role of Tfh cell subtypes as potential key factors in RA pathogenesis. We propose three novel findings: (1) Tfh cell markers CXCR5, ICOS, OX40, and CD40L may play important roles in the pathogenesis of RA; (2) CD4+CXCR5+ and CD4+CXCR5+CD40L+ Tfh cells are promising predictors of RA disease activity and autoantibodies production; and (3) in the early stages of RA before joint bone erosion, blocking CD4+CXCR5+CD40L+ Tfh cells and CD4+CXCR5+ICOS+ Tfh cells may prevent RA progression.
Conclusions
Our data provide evidence that Tfh cells are dysregulated in patients with RA. The immunoregulatory molecules CXCR5, CD40L, and OX40 were positively correlated with RA disease activity and autoantibody production. More importantly, we further revealed that the immunoregulatory molecules CD40L and ICOS were positively correlated with RA disease severity only in patients without joint bone erosion. These results indicate a strong association between increased circulating Tfh cells and RA, which highlights that CD4+CXCR5+CD40L+ Tfh cells are related to disease activity, autoantibody production, and joint bone erosion; therefore, this Tfh cell marker subtype could be a reliable detection index and therapeutic target for RA.
Further studies are needed to explore pathways related to different Tfh cell markers in RA patients and to confirm these results in studies with larger sample sizes.
Footnotes
Author Disclosure Statement
The authors declared no potential conflict of interests with respect to the research, authorship, and/or publication of this article. No author has a financial interest in any of the products, devices, or drugs mentioned in this study.
Funding Information
The authors received a grant from the Department of Finance of Jilin Province (2019scz033) for the research, authorship, and publication of this article.