
Abstract
The impact of noninvasive ventilation (NIV) on local and systemic inflammation is poorly characterized, particularly when compared with invasive mechanical ventilation (IMV). We sought to quantify the local and systemic inflammatory response of these 2 respiratory treatments in rats with lipopolysaccharide (LPS)-induced lung injury (LPS-injured) and healthy rats. Animals were subjected to 4 h of NIV or IMV treatments at noninjurious settings, or 4 h of control treatment in which healthy or LPS-injured animals remained spontaneously breathing under isoflurane anesthesia with no respiratory support. Cytokines were then quantified in the serum and lung tissue by multiplex enzyme-linked immunosorbent assay. Contrary to our hypothesis, there were no significant differences in cytokine levels in serum or lung when comparing the NIV- and IMV-treated groups; this was true in both LPS-injured and healthy rats. However, within the LPS-injured group, pulmonary levels of interleukin (IL)-1α, IL-6, and tumor necrosis factor α were significantly lower in the NIV-treated group than in control but not in the IMV-treated group compared with control. We conclude that NIV, unlike IMV, could attenuate local inflammation.
Introduction
Noninvasive ventilation (NIV) encompasses various methods of mechanical respiratory support that are associated with 5-fold fewer complications than invasive mechanical ventilation (IMV) (Carron and others 2013). Furthermore, NIV can prevent progression to IMV and reduce mortality across various patient populations and disease processes (Vital and others 2013; Faria and others 2015; Yaman and others 2016; Lemyre and others 2017; Osadnik and others 2017; Franklin and others 2018).
Thus, NIV is commonly used as a first-line intervention for support. Although these clinical benefits of NIV have been reasonably accepted, its impact on mechanical stress, local inflammation, and systemic inflammation—factors associated with ventilator-induced lung injury (VILI)—has had little investigation.
Ventilator-induced lung injury is mediated by interrelated physical and biological forces that synergistically cause release of various inflammatory mediators (Tremblay and Slutsky 2006; Beitler and others 2016). Although cytokine expression is highly variable, possibly due to heterogeneous models and injury methods, interleukin (IL)-1, IL-6, IL-8, and tumor necrosis factor α (TNFα) are elevated in most reports (Halbertsma and others 2005). Owing to this paucity of biochemical data in NIV-treated respiratory failure, we sought to quantify its effects on local and systemic inflammation in healthy and lung-injured rats. We hypothesized that use of NIV is associated with less local and systemic inflammation than IMV.
Methods
To test our hypothesis, rats were divided into healthy lung and lipopolysaccharide (LPS)-induced lung injury (LPS-injured) groups. Rats allocated to the healthy group were then divided into control, NIV, or IMV treatment. Rats allocated to the LPS-injured group received intratracheal LPS, then received NIV or IMV treatment. Control rats in the LPS-injured group received no respiratory support. A sham group receiving only endotracheal 0.9% NaCl (vehicle) was also included in the LPS group. Figure 1 illustrates the groups and treatments.
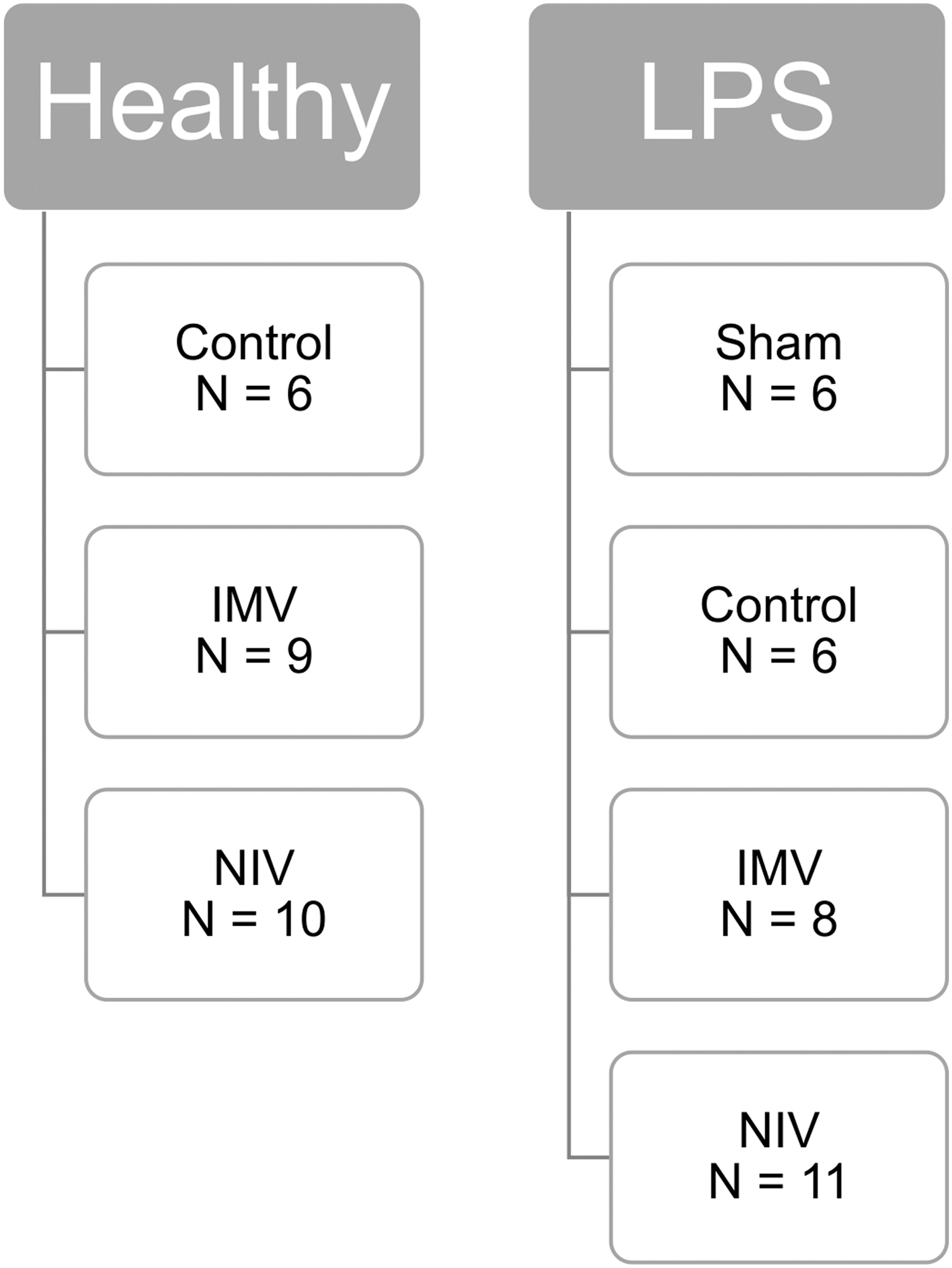
Allocation of 56 rats into healthy versus LPS-injured groups and treatment. LPS, lipopolysaccharide.
Animal preparation and general methodology
All animal procedures were performed in accordance with the National Institutes of Health guidelines with protocols approved by the Loma Linda University Institutional Animal Care and Use Committee. Male Sprague-Dawley rats [Crl:CD(SD); Charles River, San Diego, CA] were used for all protocols. Rats were allowed to acclimate for a minimum of 48 h and had access to food and water ad libitum.
We induced and maintained anesthesia with isoflurane 1.5%–2.5% in ambient FiO2. Standard monitoring included heart rate, respiratory rate, oxygen saturation, and core body temperature recorded every 2 sec (PhysioSuite, Kent Scientific Corporation, Torrington, CT). Expiratory CO2, positive end expiratory pressure (PEEP), and peak inspiratory pressure were continuously monitored and recorded every 15 min. All rats underwent 4 h of prescribed respiratory treatment.
Both NIV and IMV were delivered by a small animal ventilator (AVS-1 Cycle-Triggered Ventilator, CWE, Inc., Ardmore, PA) with a PEEP of 5 cmH2O and tidal volumes of 8–10 mL/kg of body mass in both the NIV and IMV groups. Nonventilated control and sham rats were maintained on 1.5%–2.5% isoflurane in ambient air.
Noninvasive interface
To create an adequate seal, a 1 × 1 cm T-shaped incision was made in a rodent anesthesia mask (Braintree Scientific, Inc., Braintree, MA) with anterior aspect of snout within the cone and the expiratory limb of the circuit near the snout (Fig. 2).
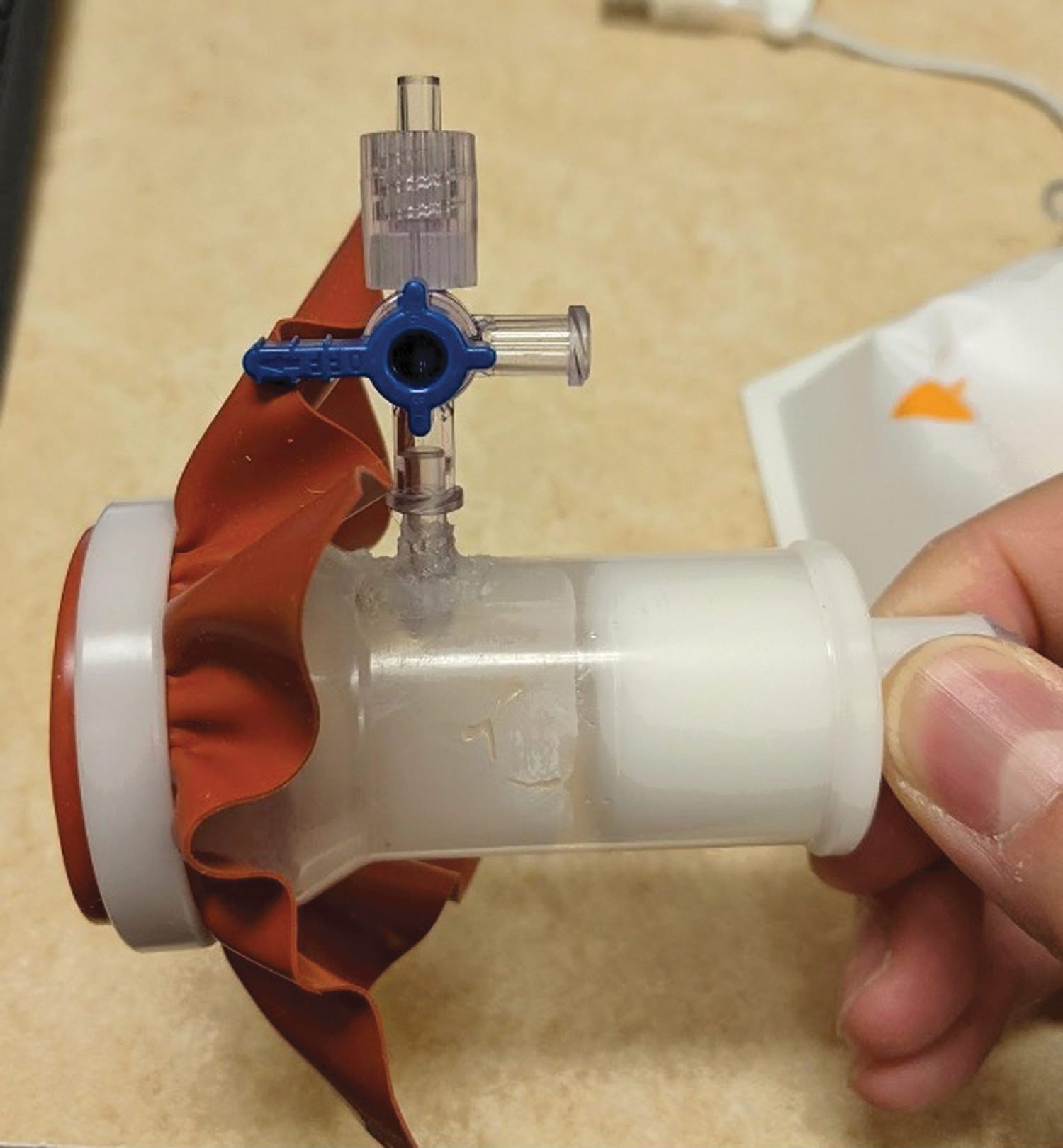
Noninvasive interface with the expiratory limb at the superior aspect of the mask, inspiratory limb to the right, and the snout interface at the left.
Intubation and invasive interface
Under isoflurane anesthesia, rats were intubated using a digital otoscope (USB Digital Ear Otoscope; Teslong Technology, Shenzhen, China) and a 16-gauge × 50 mm IV catheter (Introcan Safety; B. Braun Medical, Inc., Bethlehem, Pennsylvania) (Supplementary Video S1).
Lung injury model
All rats in the LPS group were transiently intubated through digital laryngoscopy as already outlined. We used 1,000 μg/kg of purified LPS (Escherichia coli 0111:B4, L4391; Sigma, St. Louis, MO) as an inflammatory stimulus, which was directly instilled into the trachea using a previously published technique (Jansson and others 2004; Balan and others 2011; Gresham and others 2011). Rats were allowed to acclimate for 30 min after LPS instillation then divided into the prescribed treatments.
Tissue preparation
After the 4-h experimental period, the rats were subjected to 4% isoflurane and terminal percutaneous cardiac puncture to extract whole blood. The right and left lungs were extracted, rinsed with saline, and immediately frozen at −80°C. Blood was allowed to clot for 30 min at room temperature then centrifuged at 1,000 g for 10 min. The resulting serum was extracted and stored at −80°C.
To extract tissue supernatant, the entire right lung was homogenized with 1,000 μL of protein isolation buffer. The homogenate was gently rocked for 1 h at 4°C, then centrifuged twice at 14,000 g for 20 min at 4°C. The resulting supernatant was aliquoted and either frozen or used immediately for protein and cytokine quantification.
Protein and cytokine quantification
Supernatant protein concentration was quantified using a Pierce BCA Protein Quantification Kit (Thermo Fisher Scientific, Waltham, MA) using standard clear 96-well plates using a BioTek Synergy HT microplate reader with 590 nm filter (BioTek Instruments, Inc., Winooski, VT).
Multiplex enzyme-linked immunosorbent assay (ELISA) was performed according to the provided instructions from a 9-plex rat inflammation kit and analyzed on a Q-View Imager LS (Quansys Biosciences, Logan, UT). Serum cytokine concentration was expressed as pg/mL of fluid and in lung supernatant as pg/mg of total protein.
Statistics and data analysis
Data were analyzed using a univariate general linear model [2-way analysis of variance (ANOVA)] in SPSS v.27 (IBM, Armonk, NY). We elected not to use nonparametric testing because it would limit the classes of comparison. The general linear model is robust for moderately skewed data. Cytokine values above or below the detection limits of our hardware and software were derived by multiple imputation with constraints set to 0 for each variable. Five imputations were performed with a linear regression model. Overall, 28% of data were imputed. Post hoc analyses for significant values in between-subject effects were performed with Tukey HSD. P-values <0.05 were considered statistically significant.
Results
Ultimately, 56 rats underwent experimental protocols and 52 underwent cytokine analysis (Fig. 1). Four rats died before completion of the 4-h experimental period and were excluded. Between LPS-injured and healthy groups, significant differences were noted in weight, average heart rate, and average temperature. When comparing treatment cohorts within groups, significant differences were noted in weight and temperature. There was a significant interaction effect of the LPS-injured group and treatment on heart rate. Subanalysis showed the strong interactions of LPS injury and independent of other treatments. No significant differences were noted in average respiratory rate and oxygen saturation. Vital signs are summarized in Table 1.
Quantity, Weight, and Average Vital Signs of Rats During 4-H Ventilation Period
All values are reported as mean (±SD).
P = 0.001 between groups and P = 0.000 between interventions.
P = 0.002 between groups.
P = 0.048 between groups and P = 0.02 between interventions.
HR, hazard ratio; LPS, lipopolysaccharide; RR, relative risk; SD, standard deviation.
Pulmonary inflammation
LPS produced robust pulmonary inflammation with significantly greater IL-1α, IL-6, IL-12, interferon (IFN)γ, and TNFα levels, but similar IL-1β (P = 0.056) levels, in the LPS-injured group than in the healthy group.
In multiple comparisons within the LPS-injured group, there were no differences in pulmonary cytokine concentrations between NIV and IMV treatments. Pulmonary IL-1α, IL-6, and TNFα were significantly lower in the NIV-treated rats than in the nonventilated control rats; IL-1β was similar in NIV-treated rats compared with the nonventilated control rats (P = 0.056); IL-6 was significantly lower in the IMV-treated rats than in the control rats; IL-1α, IL-6, and TNFα were significantly lower in the sham rats than in the control rats.
In multiple comparisons within the healthy rat group, there were no differences in pulmonary cytokine concentration across control, NIV-, and IMV-treated animals. The results of VILI-associated cytokines within the lung are summarized in Fig. 3A–D.
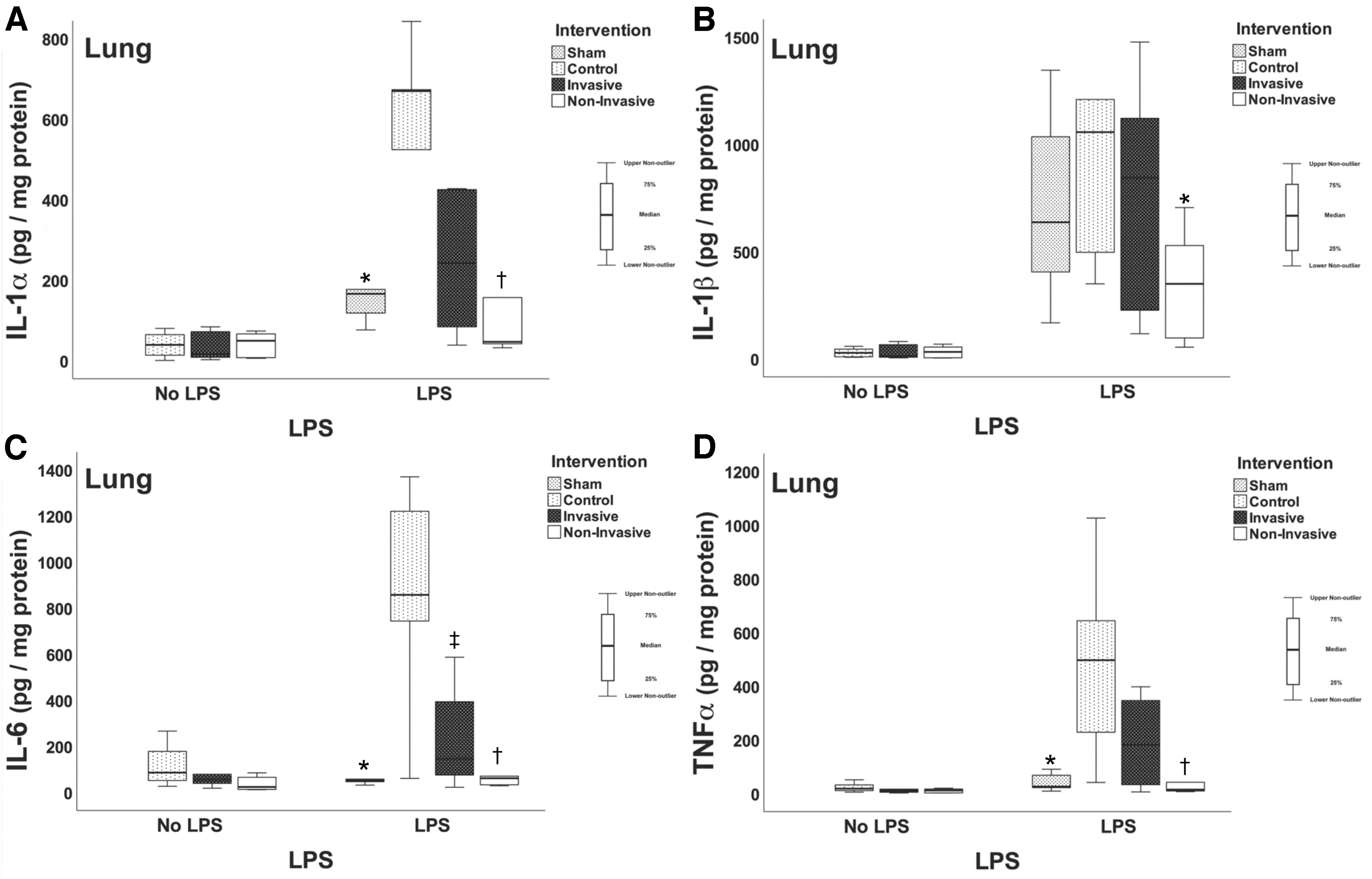
Graphical representation of only pulmonary IL-1α, IL-1β, IL-6, and TNFα divided between group (no LPS vs. LPS) then by intervention. NIV is associated with lower cytokine values compared with control.
Systemic inflammation
In the serum, between the healthy and LPS-injured groups, IL-1α, IL-12, and IFNγ concentrations were significantly higher in the healthy group than in the LPS-injured group. IL-1β, IL-6, and TNFα were similar between the healthy and LPS-injured groups. In multiple comparisons, there were no significant differences in serum cytokine concentration between the different respiratory interventions between treatments (data from serum are not shown).
Discussion
In this study, we compared the impact of NIV and IMV on systemic and local inflammation in healthy and LPS-injured rats. We found that there were no differences in cytokine concentration, locally or systemically, between these 2 modes of ventilation in both healthy and LPS groups. Furthermore, in the healthy group of rats, both NIV and IMV failed to induce a systemic or local inflammatory response greater than nonventilated controls. Interestingly, in LPS-injured rats, treatment with NIV reduced inflammation compared with control, indicating a possible local protective effect of NIV in the setting of pulmonary inflammation.
NIV reduces work of breathing and dyspnea compared with spontaneous breathing alone (Kallet and Diaz 2009). Physiologically, NIV improves dynamic lung compliance, ventilation–perfusion matching, and gas exchange in both primary and secondary pulmonary disease (Kallet and Diaz 2009). Moreover, the application of heat and humidity in NIV reduces local TNFα, IL-6, and IL-8 when compared with spontaneous breathing alone (Chidekel and others 2012; Jiang and others 2015). Our cytokine findings for NIV in lung injury significantly contribute toward and support the limited current clinical literature.
Carvalho and others (2015) demonstrated decreasing inflammation in neonates with respiratory distress syndrome treated with nasal continuous positive airway pressure, though there was no comparison group. Miao studied several non-VILI–associated cytokines in acute asthma exacerbation and demonstrated higher levels in the standard oxygen therapy group relative to the bilevel positive airway pressure group (Miao 2018). In the comparison with IMV, the preservation of spontaneous breathing with NIV may also limit the risk of VILI while still providing controlled tidal volume and transpulmonary pressure support in mild lung injury (Saddy and others 2013; Xia and others 2014).
Invasive ventilation is a life saving measure with no alternatives in severe respiratory failure. However, clinical data suggest improved outcomes with NIV compared with IMV for mild-to-moderate illness (Honrubia and others 2005; Yanez and others 2008; Lindenauer and others 2014). Our research adds depth to this comparison by demonstrating no change in cytokine levels when controlling for positive pressure modality. This is consistent with the literature suggesting that clinical context and complications influence outcomes. For example, IMV may be complicated by ventilator-associated pneumonia, pneumonitis, airway injury, pneumothorax, sedative and paralytic use, neuropathy, and other complications (Principi and others 2010; Nourdine and others 1999).
Since the fundamental distinction between the 2 treatment groups was method of positive pressure delivery, the lack of difference between cytokine values between IMV and NIV is not surprising. Our study was strengthened by utilizing these treatments in a controlled scenario that minimized iatrogenic VILI by choosing near-physiological and noninjurious settings to imitate real-world ICU management, thus isolating the inflammatory response (Beitler and others 2016). In addition, we utilized a “two-hit” model, as pulmonary inflammation may be heightened by injurious IMV settings (Hoegl and others 2018).
A 4-h ventilation period was chosen as multiple VILI-associated cytokines rise and fall within this time frame (Van Snick 1990; Tracey and Cerami 1993; Jansson and others 2004). Whole lung was used rather than bronchial-alveolar lavage to evaluate total cytokine levels rather than those produced by intraluminal cells. Although there were statistical differences in the average temperature and heart rate during the 4-h ventilation period, these were all within the physiological norm for rats.
In this preliminary study assessing the potential inflammatory effects of NIV, we were faced with limitations. Cytokine values were obtained at a single time point and not longitudinally. Lack of a commercially available rodent NIV mask and interface necessitated our own custom design and assembly from available masks. The inherent limitations of fluorometric ELISAs imply an upper and lower limit of detection, therefore, values outside the detection limit were imputed before 2-way ANOVA application. There is no exact rodent IL-8 homolog, thus limiting its analysis. Future studies can address these limitations.
To summarize, in both healthy and injured lungs, systemic and pulmonary inflammation was similar when NIV and IMV were utilized at moderate settings. More importantly, with mild lung injury, NIV may reduce local inflammation by preserving spontaneous breaths, supporting or reducing transpulmonary pressure, limiting tidal volumes, and supplying warmed humidified air. Our results are encouraging from the perspective of clinical practice because they provide evidence that NIV is an intervention that may reduce or attenuate proinflammatory cytokine release and mitigate further damage to the lung parenchyma.
Footnotes
Acknowledgments
The authors thank Loma Linda University Department of Pediatrics and Loma Linda University Animal Care Facility.
Authors' Contributions
B.C.W. contributed to conceptualization, methodology, investigation, data curation, visualization, writing—original draft, writing—review and editing, and funding acquisition. R.P.L. was involved in conceptualization and writing—review and editing. M.A. carried out conceptualization and writing—review and editing. J.A. carried out methodology, investigation, and writing—review and editing. D.D.D. carried out methodology, formal analysis, visualization, and writing—review and editing. C.G.W. was in charge of conceptualization, methodology, resources, supervision, writing—review and editing, and funding acquisition.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by Loma Linda University Pediatric Research Initiative Grant No. 71-558517-7198 and NIH Grant No. 5R21HD092941-02.
Supplementary Material
Supplementary Video S1