
Abstract
Soluble cell adhesion molecules (sCAMs) are involved in the development of neoplastic diseases. sCAMs can block lymphocytes and promote angiogenesis and migration of breast cancer (BC) cells. Interleukin 6 (IL-6) and tumor necrosis factor α (TNF-α) enhance metastatic potential via upregulation of CAMs. We assessed soluble interleukin-6 receptor subunit alpha (IL-6Ra), TNF-R1, TNF-R2, E-selectin, P-selectin, VCAM-1, ICAM-1, and EpCAM in 89 women with stage I–III BC and 28 healthy women. Blood samples were obtained at the beginning of neoadjuvant/induction (N = 49) or adjuvant treatment (N = 40), and after 2 months. Surgery revealed complete response in 29.4% of patients, partial response in 67%, and stable disease in 5.9%. Achieving a pathological response was 4 times greater for baseline levels of sIL-6Ra >5.63 ng/mL [odds ratio (OR) = 4.1, 95% confidence interval (CI): 0.8–20.4, P = 0.08] and more than 6 times for soluble tumor necrosis factor receptor 1 (sTNF-R1) ≥ 0.97 ng/mL (OR = 6.2, 95% CI: 1.2–32.3, P < 0.05). Compared with the control group, serum sP-selectin, soluble epithelial cell adhesion molecule (sEpCAM), and sTNF-R2 concentrations were significantly higher in patients who started adjuvant therapy (P < 0.05) and preoperative therapy (P < 0.01). Baseline serum sIL-6Ra concentrations were significantly higher in patients before surgery than in patients after tumor resection (P < 0.05), independent of the follow-up time. The baseline serum soluble receptors of IL-6 (sIL-6R) and TNF-α (sTNF-R1) concentrations have a predictive value for preoperative therapy in patients with BC.
Introduction
Breast cancer (BC) is the most frequently diagnosed cancer and the second leading cause of cancer death in women (NCCN, 2022). Despite the implementation of screening programs, more effective regimens, and widely used perioperative treatments, many women die from disease relapse (Hankinson et al, 2020). Therefore, BC requires a multidisciplinary approach and a combination of therapies, such as surgery, radiation therapy, chemotherapy (CTH), hormone therapy (HTH), immunotherapy, and targeted therapy. The choice of therapy depends on the tumor size, hormone receptors, human epidermal growth factor receptor 2 (HER2) status, desire for breast preservation, and recurrence risk. Systemic therapies may be administered before or after the main treatment, such as mastectomy or breast conservation therapy (BCT). Adjuvant therapies are used after surgery to kill remaining BC cells.
In turn, preoperative therapy helps to reduce the size of the tumor, decreases the invasiveness of surgery, and destroys the spread of BC cells. Initially, preoperative CTH (induction CTH) was administered only in locally advanced inoperable BC (Gasparini et al, 1992). Currently, however, the preoperative approach also includes neoadjuvant settings in patients with early stage BC and a high risk of progression based on core needle biopsy (Miller et al, 2014). However, predictors of neoadjuvant/induction therapy are largely unknown. A pathological complete response (pCR) to preoperative therapy was obtained in 17% of women, according to a large meta-analysis (Li et al, 2017). Patients with estrogen receptor/progesterone receptor (ER/PR) negative and HER2 amplified BC phenotypes are more likely to experience pCR (Haque et al, 2018; Katayama et al, 2021). Thus, the search for new predictors of pCR to preoperative therapy is still justified.
Notably, soluble cell adhesion molecules (sCAMs) such as soluble intercellular adhesion molecule 1 (sICAM-1), soluble vascular cell adhesion molecule 1 (sVCAM-1), sE-selectin, sP-selectin, and soluble epithelial cell adhesion molecule (sEpCAM) are frequently studied in oncology. In numerous studies, elevated serum levels of sCAMs have been observed in patients with malignant tumors compared with those with benign diseases (Altomonte et al, 1999; O'Hanlon et al, 2002; Shariat et al, 2004). Relationships between sCAM levels and survival outcomes have been reported (Bewick et al, 2004; Hebbar et al, 1998; Zhang and Adachi, 1999). Their higher concentrations indicated patients with shorter progressionfree survival (PFS) or overall survival (OS) in metastatic BC (Bharti et al, 2018; Bulska-Będkowska et al, 2022; Hebbar et al, 1998; Zhang and Adachi, 1999) and patients with other cancers (Liu et al, 2020; Shah et al, 2012; Shimura et al, 2018).
sCAMs are also involved in the development of neoplastic diseases (Borsig and Laubli, 2019). In vitro sCAMs block lymphocytes, promote angiogenesis, and migration of BC cells (Fukushi et al, 2000; Strell et al, 2010; Tsakadze et al, 2004). Therefore, sCAMs should be studied as potential predictors for preoperative therapy.
The expression of CAMs in BC cells is induced by interleukin 6 (IL-6), tumor necrosis factor α (TNF-α), and other cytokines (Figenschau et al, 2018; Geng et al, 2013; Hutchins and Steel, 1994). In addition, there is an association between serum concentrations of sCAMs and major mediators of inflammation (Zhang and Adachi, 1999). IL-6 and TNF-α promote several protumorigenic activities through their respective receptors. Binding of IL-6 to the IL-6 receptor (IL-6R) activates distinct Janus tyrosine kinase/signal transducers and activators of transcription (JAK/STAT) and other signaling pathways (Taher et al, 2018). Soluble tumor necrosis factor receptor 1 (sTNF-R1) plays a role in nuclear factor kappa B (NF-κB) and c-Jun activation, which inhibits apoptosis and promotes the proliferation of cancer cells (Mercogliano et al, 2020).
Thus, among the inflammatory factors, soluble receptors of IL-6 (sIL-6R) and TNF-α (sTNF-R1 and sTNF-R2) deserve attention. Increased levels of IL-6 and TNF-α have been associated with shorter survival in several cancer types (Laino et al, 2020; Lu et al, 2012; Sanguinete et al, 2017). However, data regarding their receptors are limited. Their predictive value for preoperative therapy in patients with BC has not yet been investigated.
Therefore, this study aimed to assess the usefulness of the above-mentioned sCAMs and receptors of major mediators of inflammation in the prediction and monitoring of response to therapy for nonmetastatic BC.
Materials and Methods
Patients
This single-center study enrolled 105 women with BC and 28 apparently healthy women who were admitted to the Department of Internal Diseases and Oncological Chemotherapy between July 2014 and September 2019. Inclusion criteria for the study group were as follows: (1) histologically confirmed BC in a core-needle biopsy or a surgical biopsy, (2) BC of stage I–III according to the 8th edition of the American Joint Committee on Cancer (AJCC) (Giuliano et al, 2017), and (3) condition after mastectomy or BCT or condition before surgery.
The exclusion criteria were as follows: (1) development of a second malignant tumor in organs other than the breast or axillary lymph nodes during observation (n = 4), (2) thrombosis at the onset of diagnosis or during treatment (n = 2), (3) history of autoimmune disease (n = 6), and (4) hemolysis in blood specimens (n = 5). One patient met 2 exclusion criteria. Finally, the analysis included 89 patients, who were divided into 2 groups: 49 patients qualified for adjuvant therapy (subgroup 1) and 40 patients qualified for preoperative (neoadjuvant/induction) therapy (subgroup 2), and the control group included 28 healthy women.
The patients were treated with various regimens consisting of anthracycline- or taxane-based CTH, HER2 targeted therapy, and HTH. Regimens were selected according to the performance status of patients, biological subtypes of BC, and risk factors. Overall, in adjuvant therapy, 77% of patients (n = 38) received anthracycline without taxane (AC = 11, FAC = 2, FEC = 1, EC = 5) or subsequently with taxane (TAC = 1, AC/PXL = 3, AC/T = 5, EC/T = 2) and trastuzumab (AC/T/trastuzumab = 6, AC/PXL/trastuzumab = 2). Two patients received HTH (egistrozole), and 8 patients continued therapy with trastuzumab (n = 4) or taxane (n = 4) as monotherapy. One patient was followed-up without any treatment.
Preoperative therapy was based on anthracycline without taxane (AC = 1, FEC = 1) or with taxane (AC/T = 8, AC/PXL = 6) and trastuzumab (AC/T/trastuzumab = 3, AC/PXL/trastuzumab = 5, AC/T/trastuzumab/pertuzumab = 1, AT/trastuzumab = 1), which was continued after surgery. Three patients received HTH (egistrozole = 1, tamoxifen = 2), 1 patient received trastuzumab as monotherapy, 10 patients continued therapy with taxane and trastuzumab (PXL/trastuzumab = 6, T/trastuzumab = 4).
Surveillance was conducted in accordance with the recommendations of the National Comprehensive Cancer Network (NCCN). Patients underwent physical examination 2–4 times per year for 5 years, and then annually. In the case of clinical signs and symptoms suggestive of recurrent disease, laboratory and imaging studies for metastases were performed.
This study was approved by the Bioethics Committee of the Medical University of Silesia in Katowice (KNW/0022/KB1/2/15, KNW/0022/KB1/2/I/15/16, KNW0022/KB1/2/III/15/16/18/19) before the commencement of the study. Informed consent was obtained from all patients.
Measurement of sCAM and cytokines
Fasting peripheral blood samples (5 mL) were obtained from patients at the beginning of adjuvant therapy or preoperative therapy and after 2 months from the first assessment. Blood sampling was performed once for the control group. The samples were collected in serum separator tubes and allowed to clot for 30 min. Before centrifugation at 3,000 rpm for 10 min to obtain serum, the samples were transferred to tubes and instantly stored in liquid nitrogen until analysis. The serum concentrations of the soluble forms of E-selectin, P-selectin, VCAM-1, ICAM-1, EpCAM, interleukin-6 receptor subunit alpha (IL-6Ra), TNF-R1, and TNF-R2 were determined using a multiplex technique (RnD MN) according to the manufacturer's instructions.
In brief, 25 μL of serum was mixed with 25 μL of a premixed bead cocktail, incubated for 1 h, and washed using an automatic magnetic washer. Next, 25 μL of biotinylated antibody cocktail was added and the samples were incubated at room temperature for another 30 min. After the subsequent washing step, the streptavidin-R-phycoerythrin complex was added and incubated for another 20 min. After subsequent washing, beads were suspended in sheath fluid and bead fluorescence readings were taken using the Bio-Plex 200 System with a high PMT (High RP1) setting and analyzed using Bio-Plex Manager version 6.1.0.727 (Bio-Rad Laboratories).
Data analysis
Diabetes mellitus was diagnosed based on fasting serum glucose levels >125 mg/dL in 2 separate tests or medications taken (ADA, 2010). Hypertension was considered if the mean systolic blood pressure from 2 measurements was ≥140 mmHg and/or diastolic blood pressure was ≥90 mmHg or if antihypertensive drugs were used (Mancia et al, 2013). Body mass index was calculated as the weight (kg) divided by the square of the height (m).
Response to preoperative treatment was analyzed according to the Pinder classification (Park et al, 2016). A short pCR was reported if no residual cancer tissue or only cancer in situ was found after surgery in the breast tissue and axilla. Pathological partial response (pPR) was recorded when the minimal residual disease was found (<10% of invasive tumor left) or there was a 10%–50% invasive tumor left or >50% invasive cancer tissue left with the post-CTH effect. A pathological no response (pNR) was reported if there were no signs of response in the breast tissue.
Statistical analysis
Statistical analyses were performed using STATISTICA 13.0 PL (TIBCO Software, Inc., Palo Alto, CA), StataSE 13.0 (StataCorp LP), and R software (R Core Team, 2013; R Foundation for Statistical Computing, Vienna, Austria;
Homogeneity of variances was assessed using the Levene's test. Nominal and ordinal data were compared using the χ2 test. Comparisons between groups for interval data and longitudinal data were performed using mixed models (with either raw variables or after logarithmic transformation in the case of non-normal data distribution). Post hoc tests were performed using 1-way analysis of variance (ANOVA) with the Benjamini-Hochberg correction for multiple testing. To find cutoffs for sCAMs, a nonparametric receiver operating characteristics (ROC) analysis was performed using the Youden index. The association between binomial variables was expressed as odds ratios (OR) with a corresponding 95% confidence intervals (CIs) and P value.
Taking into account, the effect size f = 0.40, noncentrality parameter λ = 16.32, critical F value = 3.09, and the following assumptions given below, the sample size was calculated for 1-way ANOVA, with the G*Power software (v. 3.1.9.7). The following assumptions were made: the CI is 95% (type I error α = 0.05), the power of the test is 0.80 (type II error), the number of groups is 3, standard deviation within each group is 22. The overall sample size of the study group should be 102 subjects (with calculated power of 0.955). Taking a 10% of drop-out, the final sample size should be not less than 112 subjects.
Results
The study group consisted of 89 women with stage I–III BC aged 31–79 years (average age 57 ± 11 years). Patients treated with adjuvant therapy were significantly older than those treated with neoadjuvant/induction therapy (subgroup 1 versus 2, 59 ± 10 versus 54 ± 11, P < 0.05). The subgroups differed in tumor size and stage (P < 0.05) but not in lymph node involvement. In both subgroups, most patients had hormone-receptor-positive/HER2 negative (HR+/HER2) BC. Hypertension was diagnosed in more than half of the patients. Characteristics of the study group and subgroups, including age, histology, staging, grading, receptor status, and comorbidity, are shown in Table 1.
Characteristics of the Study Group and Subgroups of Patients Treated with Adjuvant Therapy (Subgroup 1) and Preoperative Therapy (Subgroup 2)
N, number, mean ± standard deviation, median (lower quartile–upper quartile).
BC, breast cancer; HER2, human epidermal growth factor receptor 2; HR, hormone-receptor.
The mean follow-up period was 45 ± 18 months (range: 14–81 months). During the surveillance, 10 (11.2%) patients had disease progression and 8 (9%) died. The average disease-free survival was 23 ± 12 months (range: 6–42 months) and the OS was 37 ± 11 months (range: 18–52 months).
In subgroup 1, mastectomy was performed in 54% (n = 27) of patients. The remaining patients were treated with breast-conserving therapy (n = 19), a 2-stage procedure (n = 3), and removal of recurrence within the scar (n = 1). Lymphadenectomy was performed in 62% of patients (n = 32). The pathomorphological examination of resection specimens revealed angioinvasion in 10% of patients (n = 5), adipose tissue invasion in 26% (n = 13), invasion of the node capsule in 14% (n = 7), and positive margins in 22% (n = 11).
The median serum concentrations of sCAMs and cytokines at baseline in both the subgroups and healthy controls are shown in Table 2. Significant differences in serum sP-selectin, sEpCAM, sIL-6Ra, and sTNF-R2 levels were observed between groups. Compared to the control group, serum sP-selectin, sEpCAM, and sTNF-R2 concentrations were significantly higher in patients starting adjuvant therapy (43.4 versus 31.6 ng/mL, P < 0.05; 0.83 versus 0.47 ng/mL, P < 0.05; 1.54 versus 0.13 ng/mL, P < 0.001, respectively) and preoperative therapy (43.0 versus 31.6 ng/mL, P < 0.01; 0.93 versus 0.47 ng/mL, P < 0.01; 0.51 versus 0.13 ng/mL, P < 0.001, respectively) (Fig. 1).
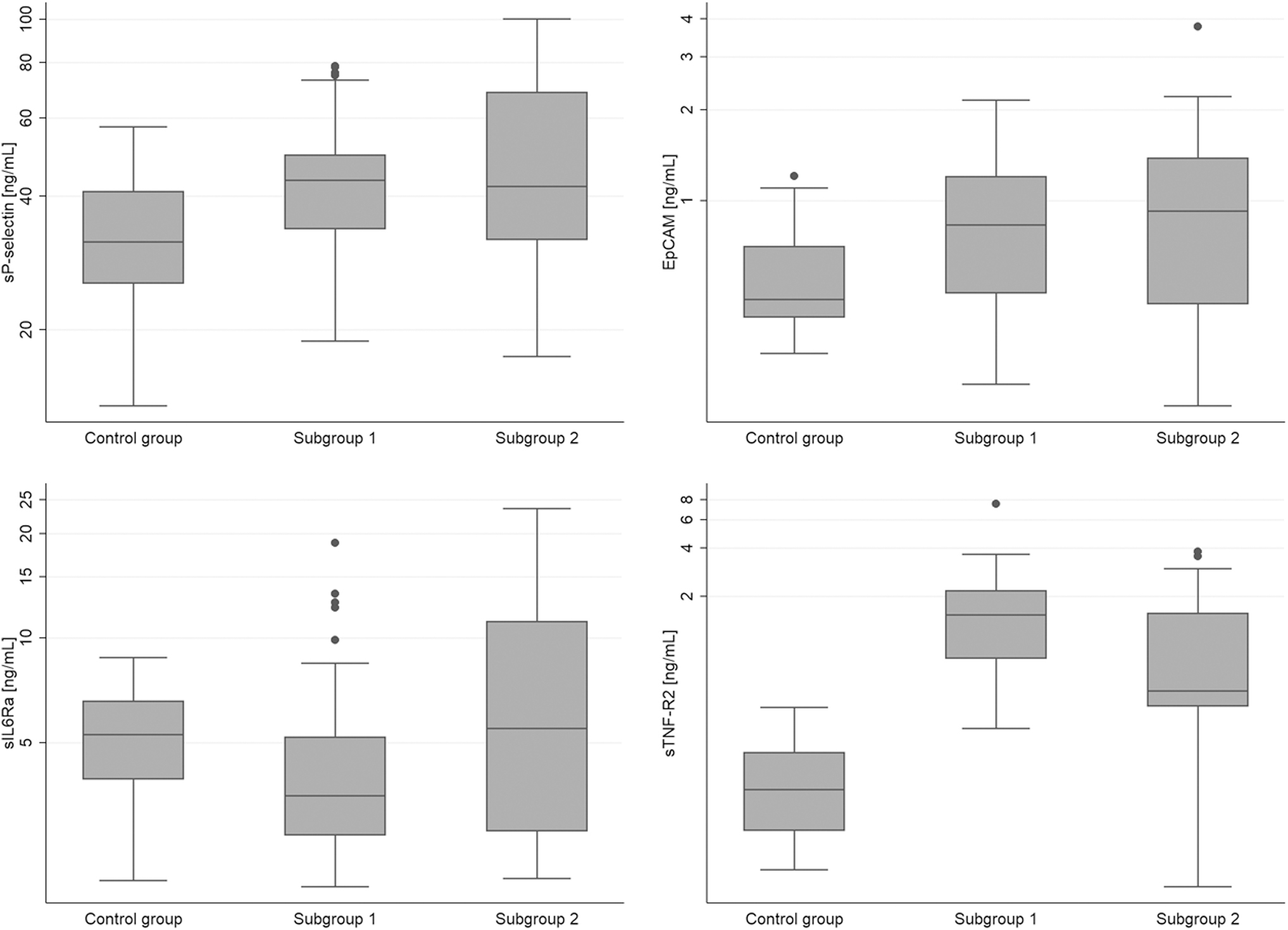
Serum sP-selectin, sEpCAM, sIL-6Ra, sTNF-R2 concentrations in BC patients treated with adjuvant therapy (subgroup 1), preoperative therapy (subgroup 2), and in control group. BC, breast cancer; sEpCAM, soluble epithelial cell adhesion molecule.
Serum Concentrations of Soluble Cell Adhesion Molecules and Cytokines at Baseline in Patients Treated with Adjuvant Therapy (Subgroup 1), Preoperative Therapy (Subgroup 2), and in the Control Group
Median (lower quartile–upper quartile).
sICAM-1, soluble intercellular adhesion molecule 1; sTNF-R1, soluble tumor necrosis factor receptor 1; sVCAM-1, soluble vascular cell adhesion molecule 1.
Baseline serum sIL-6Ra concentrations were significantly higher in patients before surgery than in patients after tumor resection (5.51 versus 3.52 ng/mL, P < 0.05). A borderline difference in serum sTNF-R2 concentration was found between subgroups 1 and 2 (1.54 versus 0.51 ng/mL, P = 0.06), while other assessed parameters did not differ between subgroups.
In subgroup 2, patients received neoadjuvant therapy in stages I–II (n = 26), and induction CTH in stage III (n = 14). There were no differences in the serum concentrations of sCAMs and cytokines between subsequent stages in subgroup 2. After preoperative therapy, definitive surgery revealed pCR in 10 patients (29.4%) and pPR in 22 patients (67%). The remaining 5.9% (n = 2) of patients showed stable disease.
In the ROC analysis, baseline sIL-6Ra and sTNF-R1 levels had a predictive role in determining the pathologic response to treatment (Fig. 2A, B). The odds of achieving a pathological response were 4 times greater in patients with higher levels of sIL-6Ra (OR = 4.1, 95% CI: 0.8–20.4). The obtained cutoff value was ≥5.63 ng/mL (70% sensitivity and 64% specificity of prediction, P = 0.08). The area under the curve (AUC) for sIL-6Ra was 0.78 (95% CI: 0.62–0.95).
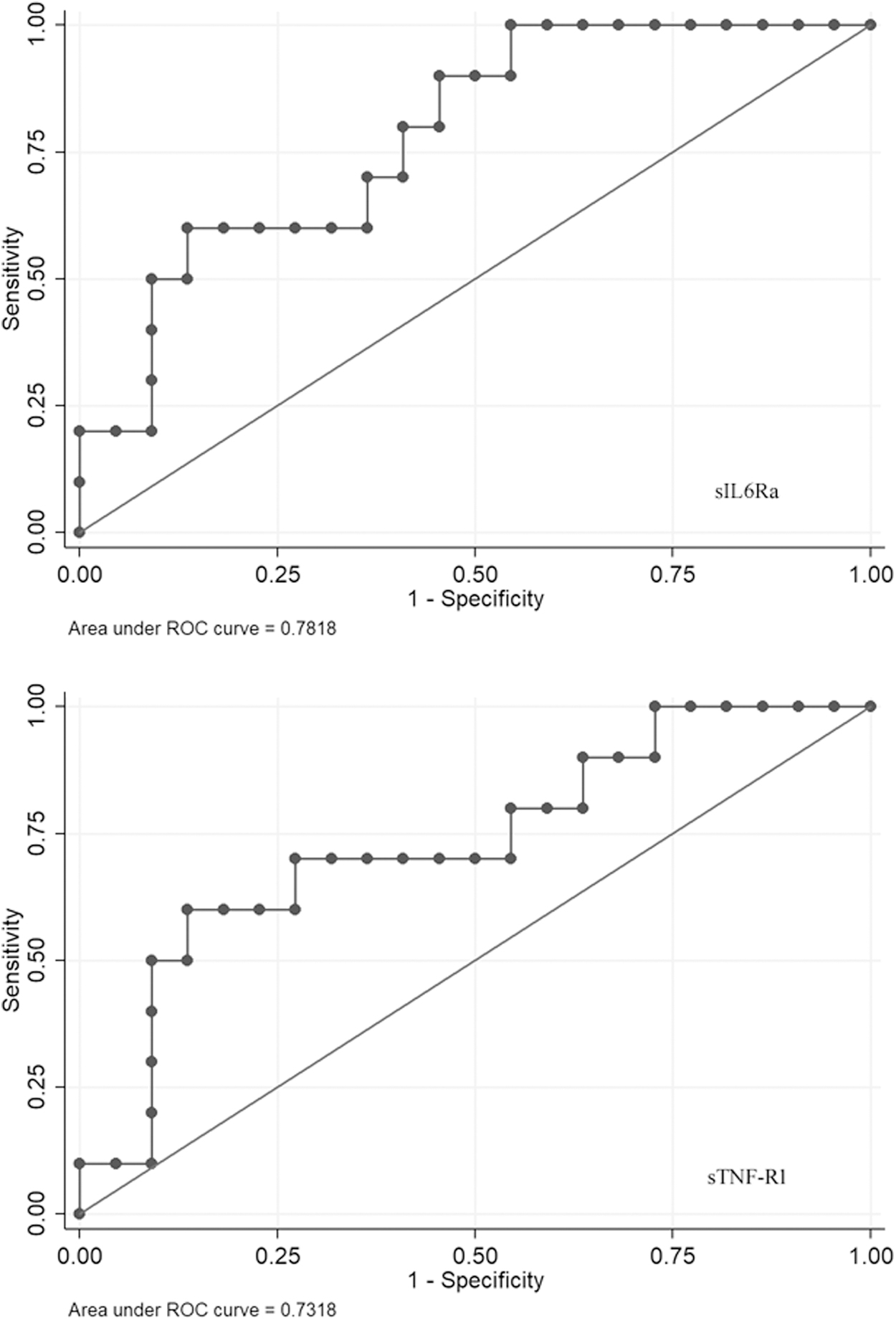
Predictive accuracy of serum concentrations of sIL-6R
Similarly, higher levels of sTNF-R1 were more than 6 times associated with the achievement of response to preoperative therapy (OR = 6.2, 95% CI: 1.2–32.3). The obtained cutoff value was ≥0.97 ng/mL (70% sensitivity and 73% specificity of prediction, P < 0.05). The AUC for sTNF-R1 was 0.73 (95% CI: 0.53–0.93).
Serum sIL-6Ra and sTNF-R1 concentrations in BC patients with a pathological response and no response to neoadjuvant/induction therapy are shown in Fig. 3.

Serum sIL-6Ra, sTNF-R1 concentrations in BC patients with pathological response and no response to preoperative therapy.
The relative percentage changes in baseline serum concentrations of sCAMs and other cytokines are shown in Table 3. There were no statistically significant differences between the subgroups in the relative percentage changes in the baseline values of serum concentrations of sCAMs and other cytokines.
Percentage Relative Change of the Initial Value of Serum Concentrations of Soluble Cell Adhesion Molecules and Other Assessed Parameters in the Patients Treated with Adjuvant Therapy (Subgroup 1) and Preoperative Therapy (Subgroup 2)
Mean ± standard deviation.
In the mixed models' analysis of longitudinal data, differences with time were observed for sVCAM-1, sTNF-R1, and sTNF-R2, and for sIL-6Ra and sTNF-R2, differences between groups were noted (Table 4). The sVCAM-1 values increased significantly during follow-up in both subgroups (P < 0.05 and P < 0.001, respectively). The values of sTNF-R1 increased only in subgroup 1, but not in subgroup 2 (P < 0.05 and P = 0.70, respectively). The values of sTNF-R2 increased during follow-up in both subgroups (P < 0.01 and P < 0.001, respectively); moreover, the initial values were higher in subgroup 1 than in subgroup 2 (P < 0.01), but no differences were noted after 3 months (P = 0.09).
Serum Concentrations of Soluble Cell Adhesion Molecules and Other Assessed Parameters Through the Follow-Up in the Patients Treated with Adjuvant Therapy (Subgroup 1) and Preoperative Therapy (Subgroup 2)
T0, baseline; T2M, level after 2 months.
Regarding the values of sIL-6Ra, there were statistically significant differences between both subgroups at the beginning and after 2 months of treatment (P < 0.05), with higher values in subgroup 2, independent of the follow-up time.
Discussion
In the present study, we analyzed the serum levels of sCAMs and selected cytokines in a single-center cohort of women with nonmetastatic primary BC who qualified for adjuvant or preoperative therapy. We failed to show differences in sCAMs levels in relationship to the I–III clinical stage of BC and prognostic significance in achieving a pathological response. Notably, we demonstrated that elevated baseline concentrations of sIL-6R and sTNF-R1 were associated with a pathological response to neoadjuvant or induction therapy. To the best of our knowledge, no previous study has reported the predictive value of these cytokines in determining the pathological response to preoperative therapy in patients with BC.
Previously, Won et al (2013) revealed that higher serum levels of sIL-6R are associated with shorter relapse-free survival in women with ER-positive BC. Similarly, pretreatment serum sTNF-R1 concentrations were considered a prognostic factor for OS in patients with all stages of BC. Survival was estimated to be worse in patients with higher concentrations of sTNF-R1 (Fuksiewicz et al, 2010). However, these studies did not include women who had received preoperative therapy. The preoperative setting offers clinical advantages, such as reduced tumor size, metastatic risk, and patient mortality, allows for monitoring of treatment response, helps to test the effectiveness of potential new therapies, and identifies biochemical and molecular changes that differentiate patients who benefit from treatment (Asaoka et al, 2020).
Based on our results, we hypothesized that the baseline concentrations of sIL-6Ra and sTNF-R1 might reflect the immune system's ability to fight cancer. Patients with a more efficient immune system probably achieve a pathological response to preoperative therapy. Our hypothesis is supported by the results of Yeh et al (2010) who observed an association between higher sIL-6R levels and improved survival in patients with colorectal cancer.
Notably, the major inflammatory cytokines and their receptors induce the opposite effects. Depending on signal strength, TNF-R1 can stimulate cell survival or promote apoptosis and cell death (Ihnatko and Kubes, 2007; Martínez-Reza et al, 2017). The majority of biological effects of TNF-α, including cytotoxicity and proliferation, occur via TNF-R1 activation (Wajant et al, 2003). Under inflammatory conditions, mTNF-R2 can transform into sTNF-R2, and sTNF-R2 neutralizes TNF-α and decreases IL-6 expression (Yang et al, 2018). Increased serum sTNF-Rs levels were found in BC patients compared to controls (Tesarová et al, 2000).
In turn, IL-6 may participate in tumor cell growth, angiogenesis, immunomodulation of the tumor microenvironment, and stromal cell activation (Taher et al, 2018). Myeloid-derived suppressor cells, M2 macrophages, and BC cells are considered the main sources of IL-6 in the tumor microenvironment (Masjedi et al, 2018; Taher et al, 2018). Recently, Bent et al (2021) demonstrated that microenvironmental IL-6 inhibits CTH-induced anticancer immunity. IL-6 can interact with cells via its membrane-bound form (mIL-6R), known as classic signaling, or via sIL-6R (trans-signaling), with the same affinity (Peters et al, 1998). The binding of IL-6 to sIL-6R activates trans-signaling pathways in all cells, as well as in cancer cells (Bharti et al, 2018). Trans-signalling promotes proinflammatory processes as opposed to classic signaling, which is anti-inflammatory (Taher et al, 2018). The protumor action of sIL-6R has been demonstrated in ovarian cancer (Lo et al, 2011) and pancreatic cancer (Lesina et al, 2011).
sIL-6R is produced via proteolysis of the ectodomain of mIL-6R by metalloproteinases, such as ADAM17 and ADAM10, and by alternative splicing of IL-6R messenger RNA (mRNA) (Taher et al, 2018). Possible sources of elevated serum levels of sIL-6Ra include tumor cells (Singh et al, 1995) and myeloid cells in the tumor microenvironment (Tsukamoto et al, 2017). ER-expressing BC cells mostly secrete the sIL-6R, while ER-negative cells mainly express the mIL-6R (Chiu et al, 1996). The majority of the analyzed patients were ER-positive (Table 1), which could explain the increased value of sIL-6R in the analyzed group (Table 2). It has been demonstrated that some breast carcinoma cell lines (MCF-7, T47D, BT20, HCC-1143, BT-474) produced sIL-6R in vitro (Celik and Bakar-Ates, 2021; Knüpfer and Preiss, 2010; Singh et al, 1995).
However, the ratio of sIL-6Ra of immune-derived to neoplastic origin is unknown. It has been shown that levels of sIL-6R were elevated in patients with other cancer types, such as melanoma, bladder, prostate, and colon cancer (Friebe et al, 2007; Kovacs, 2001; Shariat et al, 2004; Yeh et al, 2010). Higher concentrations were associated with grading and staging (Lo et al, 2011; Shariat et al, 2004; Yeh et al, 2010). However, we did not observe a difference in the serum concentrations of sIL-6R between the stages of BC in patients treated with preoperative therapy. Therefore, the serum concentrations of sIL-6R were most likely the result of an immune response to the tumor and not to tumor origin. This hypothesis is supported by the higher concentrations of sIL-6R in patients before tumor resection than in women after radical surgery.
The concentrations of sCAMs assessed in this study were similar in a group of women who started adjuvant and preoperative therapy. The high levels of sCAMs in women after surgery may be a result of the inflammatory process, typically during tissue repair. On the contrary, tumor-elicited inflammation be induced at the onset of neoplastic disease. Therefore, the concentrations of sCAMs in both groups did not differ. This hypothesis is supported by a higher concentration of sE-selectin, sICAM-1, and sVCAM-1 in BC in comparison to benign tumors, and correlations between sCAMs concentration and tumor grading, TNM staging, tumor size, lymph node involvement, and the presence of metastases (Altomonte et al, 1999; O'Hanlon et al, 2002; Sheen-Chen et al, 2004).
To date, studies on the predictive value of sCAMs in preoperative therapy have not been conducted. First, we investigated the association between any sCAMs and the achievement of a pathological response to CTH. We did not observe any association between sCAMs and the response to preoperative therapy. Previously, Karabulut et al (2014) conducted a similar analysis in patients with locally advanced and metastatic disease. Similar to our results, they revealed no relationship between serum sVCAM-1 and sEpCAM levels and palliative CTH response. In turn, Zhang and Adachi (1999) observed higher baseline serum sICAM-1 and sE-selectin levels in patients with metastatic BC who achieved progressive disease than in patients with complete response, partial response, and stable disease.
However, their study was conducted in the Japanese population. It is worth noting that sE-selectin and sICAM-1 levels differ according to ethnicity (Lutsey et al, 2006). This is probably why we did not observe a predictive value of these sCAMs in Caucasian women in our study. In several studies, the relationship between other sCAMs, such as sP-selectin and sVCAM-1, and race/ethnicity was found (Bielinski et al, 2015; Miller et al, 2003).
In summary, baseline serum sIL-6R and sTNF-R1 concentrations predicted response to preoperative treatment in a single-center cohort. Our findings require confirmation in a larger cohort, enabling sensitivity analyses of biological BC subtypes and CTH regimens. This may be useful for the selection of CTH used in preoperative therapy in patients with BC.
Conclusions
Baseline serum sIL-6R and sTNF-R1 concentrations have predictive values for preoperative therapy in patients with BC.
Serum sCAM levels do not reflect the clinical stage of patients with nonmetastatic BC.
Footnotes
Authors' Contributions
W.B.-B.: methodology; data curation; writing—orginal draft; and funding acquisition. P.C.-F.: methodology and writing—review and editing. S.C.-J.: methodology. A.J.O.: formal analysis. T.F.: methodology and writing—review and editing. J.C.: conceptualization; writing—review and editing; and supervision.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Medical University of Silesia, Katowice, Poland (No. PCN-2-086/N/0/K).