
Abstract
Early diagnosis of coronary artery disease (CAD) in patients with chest pain is a challenge. Currently diagnosis of CAD is confirmed by coronary angiography, which is invasive and not easily available in developing countries. Therefore, it is imperative to establish noninvasive biomarker for early diagnosis of CAD in patients with angina and determine the diagnostic accuracy of inflammatory biomarkers of atherosclerosis in comparison to angiography and correlate with severity of CAD in patients with angina. Diagnostic accuracy study was carried out in tertiary care hospitals, Rawalpindi, Pakistan. Total of 58 patients aged 55.24 ± 11.61 years, with chest pain and troponin-I −ve, having coronary artery stenosis ≥50% were included as cases of CAD and 55 subjects having stenosis <50% were included as controls. Nuclear factor kappa-B (NF-κB), tumor necrosis factor-alpha (TNF-α), interleukin-6 (IL-6), and high-sensitivity C-reactive protein (hs-CRP) were analyzed on immunoassay analyzers. The receiver operating characteristic curve analysis revealed significant (P < 0.05) high area under curve (95% confidence interval) with sensitivity and specificity of NF-κB 0.76 (0.65–0.85), 73% and 65%; TNF-α 0.72 (0.61–0.81), 71% and 69%; IL-6 0.62 (0.52–0.71), 64% and 53% and hs-CRP 0.62 (0.52–0.71), and 53% and 56% in CAD patients compared to controls. There was significant positive correlation between NF-κB (r = 0.44), TNF-α (r = 0.37), IL-6 (r = 0.23), and hs-CRP (r = 0.23) with severity of CAD by Gensini score. The inflammatory biomarkers, especially NF-κB and TNF-α, have highest diagnostic accuracy and indicate severity of atherosclerosis in patients with angina. These markers may be used as noninvasive biomarkers to exclude healthy individuals before undergoing angiography.
Introduction
Coronary artery disease (CAD) is a chronic inflammatory disease and leading cause of death in the developed world (Kim et al, 2018). Worldwide prevalence of CAD is 10% (Kim et al, 2019). Prevalence of CAD in Pakistan is high, ∼17% (Hussain et al, 2014; Zubair et al, 2018). The pathogenesis of CAD is extremely complex, mainly including endothelial damage reactions, lipid infiltration, chronic inflammatory damage and vascular smooth muscle cells proliferation. Atherosclerosis is the pathological build-up of plaque within arterial vessel walls and contributes to increased levels of various inflammatory markers (Falk, 2006).
Among all, raised serum/plasma nuclear factor kappa-B (NF-κB), tumor necrosis factor-alpha (TNF-α), interleukin-6 (IL-6), and high-sensitivity C-reactive protein (hs-CRP) play important role in the development of CAD. One of the most potent proinflammatory cytokines is TNF-α, a cytokine identified to have an early pathogenic role in CAD (Akash et al, 2018; Mazidi et al, 2018; Rehman et al, 2017). TNF-α is secreted by macrophages, lymphocytes, natural killer cells, and vascular smooth muscle cells. TNF-α signaling is mainly mediated by p38 mitogen-activated protein kinase/NF-κΒ light-chain-enhancer of the activated B cell pathway, and this affects almost all cells involved in atherogenesis by promoting the expression of cytokines, adhesion molecules, migration, and mitogenesis of vascular smooth muscle and endothelial cells.
Oxidative stress, hyperglycemia, and inflammation induced production of NF-κB leading to vascular endothelial damage, enhancing further inflammation, and are responsible to develop atherosclerosis of coronary arteries (Fan et al, 2018; Sifuentes-Franco et al, 2018). The development of cardiovascular disease is associated with activation of NF-κB, increased peroxynitrite, protein kinase-C, and Kelch-like erythroid cell-derived protein-nuclear factor erythroid 2-related factor. The aberrant expression of cyclin-dependent kinases and activation of transforming growth factor-βl causes the abnormal production of the extracellular matrix, which in turn enhances atherosclerosis (Robson et al, 2018). TNF-α stimulates the production of IL-6 from macrophages, lymphocytes, natural killer cells, and vascular smooth muscle cells. Various inflammatory mediators such as IL-6 and TNF-α through transcriptional stimulation of the CRP gene promote its release especially by hepatocytes (Del-Giudice and Gangestad, 2018; Sproston and Ashworth, 2018).
Besides the liver, other sites supposed to release CRP are endothelial cells, macrophages, smooth muscle cells, and lymphocytes. It stimulates the release of M-1 phenotype in macrophages and increases the production of inflammation-induced cytokines involved in atherosclerosis of coronary arteries (Sproston and Ashworth, 2018; Thiele et al, 2014).
Angina pectoris is chest pain caused by reduced blood supply to heart muscle. It may feel as pressure or squeezing in chest. The discomfort can occur in shoulders, arms, neck, jaw, or back. It can also present as shortness of breath or even may feel like indigestion (Braunwald et al, 2002). Angina is categorized as either stable angina or unstable angina according to American College of Cardiology (ACC)/American Heart Association (AHA) guidelines (Fihn et al, 2012; Marini et al, 2017). Currently diagnosis of CAD in patients with angina is based on clinical history and can only be confirmed by coronary angiography, which is invasive and not easily available in secondary/tertiary care hospitals. The patients presented with chest pain and undergoing coronary angiography have 9%–20% chance of normal coronary arteries (Asghar et al, 2017).
Other diagnostic options for CAD are stress tests, including invasive nuclear testing and exercise tolerance test, but boarder line or nondiagnostic results are found in early stages of CAD in patients with angina. Biochemical markers involved in the pathogenesis of atherosclerosis and raised in the patients of angina are yet to be validated for diagnosis of CAD in comparison to angiography. It is mandatory to diagnose CAD in patients with angina at an early stage to avoid myocardial infarction (MI) and cardiac complications.
The aim of this study was to determine the diagnostic accuracy of inflammatory biomarkers of atherosclerosis (NF-κB, TNF-α, IL-6 and hs-CRP) in comparison to angiography for diagnosis of CAD in patients with angina. Determine the correlation of the biomarkers of atherosclerosis with severity of stenosis and extent of CAD by Gensini score (GS). The raised levels of serum/plasma inflammatory cytokines and proteins, including NF-κB, TNF-α, IL-6, and hs-CRP, may be proved as the noninvasive biomarkers for the diagnosis of CAD in patients with angina
Materials and Methods
Study population
This diagnostic accuracy study was conducted at Armed Forces Institute of Pathology (AFIP), National University of Medical Sciences (NUMS) in collaboration with Armed Forces Institute of Cardiology (AFIC), NUMS, Rawalpindi, Pakistan, from October 2021 to April 2022. We followed the Declaration of Helsinki and Institutional Ethics Review Board approval (AFIC IERB No. 9/1/R&D/2020/50) was obtained before start of the study.
Total of 122 patients reported to AFIC Rawalpindi with angina was recruited in the study based on ACC/AHA guidelines (Fihn et al, 2014). Among these, 9 patients were excluded because either they did not fulfil inclusion criteria (n = 6) or not willing to participate (n = 3). Out of 113 patients, 58 cases of both genders, aged 25 to 70 years, were included in the study by consecutive sampling technique. The patients of angina having high sensitivity troponin-I (hs-trop-I) negative and coronary artery stenosis ≥50% were diagnosed as cases of CAD as per guidelines (Fihn et al, 2014) and included in the study after informed consent.
Fifty-five subjects having <50% coronary artery stenosis were included as controls (Cury et al, 2016; Kalkan et al, 2017). A known history of other cardiovascular diseases, for example, prinz-metal angina, atrial fibrillation, congestive heart failure and MI, a history of either percutaneous intervention or coronary artery bypass grafting, severe hepatic or renal dysfunction, and recent infection or active chronic inflammatory disease during the last 6 weeks, were excluded.
Patient's history of cardiovascular risk factors, including smoking, diabetes mellitus (DM), hypertension, dyslipidemias, family history of ischemic heart disease, and drug history, was recorded. Physical examination, echocardiography (ECG), and trop-I were carried out to exclude MI.
Coronary angiography
All patients were examined by invasive coronary angiography to verify the presence of CAD. Angiographies were evaluated independently by two cardiologists according to ACC/AHA guidelines (Fihn et al, 2014; Mohammed et al, 2020). The GS was calculated by multiplying the severity coefficient, that was assigned to each coronary artery stenosis according to the degree of luminal narrowing (reductions of 25%, 50%, 75% 90%, 99%, and complete occlusion given GS of 1, 2, 4, 8, 16, and 32, respectively), with the coefficient identified based on the functional importance of the myocardial area supplied by that segment (Kalkan et al, 2017; Sinning et al, 2013).
Laboratory tests
Blood samples were collected in the ethylene diamine tetra acetic acid and gel tubes from all the patients and controls. Hs-trop-I (ARCHITECT 1000i; Abbott), glycosylated hemoglobin (HbA1c), serum total cholesterol (Total-C), triglycerides (TGs), low-density lipoprotein cholesterol (LDL-c), high-density lipoprotein cholesterol (HDL-c), alanine transaminase (ALT), and creatinine were analyzed on automated chemistry analyzer (Architect Ci 4100 System; Abbott). NF-κB and TNF-α were analyzed by sandwich enzyme linked immunosorbent assay (ELISA), Elabscience (Houston, TX); IL-6 by chemiluminescent immunoassay Cobas e 601, Roche (Japan); hs-CRP by nephelometry (PA120; Genrui); malondialdehyde (MDA) by competitive-ELISA, Elabscience and homocysteine by ADVIA Centaur HCY assay, competitive immunoassay using direct chemiluminescent technology (Bastani et al, 2018; Patel et al, 2017).
Statistical analysis
Sample size was calculated by MedCalc, using AUC 0.754 (Karadeniz et al, 2015; Min et al, 2017), Type 1 error (Alpha) 0.05, Type 2 error (Beta) 0.10, and null hypothesis 50%, sample size became 51, each for cases and controls. For all statistical analyses, SPSS 22 was used. Frequencies and percentages were calculated for qualitative variables. Categorical variables were compared using chi square test. The quantitative data were presented as means ± standard deviations or median and interquartile range (IQR). Continuous variables were compared using independent sample t-test and nonparametric data were analyzed by Mann–Whitney U test and Quade's ANCOVA.
Receiver operating characteristic (ROC) curve was drawn to see diagnostic accuracy for biomarkers of atherosclerosis. Spearman's correlation was performed to determine the correlation of biomarkers (NF-κB, TNF-α, IL-6, and hs-CRP) with severity of CAD according to stenosis on angiography and GS. A 2-tailed P < 0.05 was considered significant.
Results
Baseline characteristics
Out of 113 patients, 58 patients of CAD and 55 controls were evaluated by clinical methods, ECG, biomarkers, and angiography. The baseline characteristics of the patients of CAD and controls are shown in the Table 1. The patients of CAD with angina were significantly (P = 0.006) older 55.24 ± 11.61 years than the controls 49.18 ± 11.54 years. The majority of patients who participated in the study were overweight with a BMI of >23 kg/m2 as per Asian population criteria. Most of the parameters did not reveal any significant difference between 2 groups. Most of the participants were taking a normal diet and medicines as advised by the physician.
Baseline Characteristics of Study Participants (N = 113)
Bold values indicate the Significant P value.
Data were expressed as number (percentage) = n (%) and mean ± standard deviation; chi square test for qualitative and independent sample t-test for quantitative parameters between cases of CAD and control groups; P value <0.05 was significant.
ALT, alanine transaminase; CAD, coronary artery disease; HbA1c, glycosylated hemoglobin; HDL-c, high-density lipoprotein-cholesterol; HTN, hypertension; LDL-c, low-density lipoprotein-cholesterol; Total-C, total cholesterol; VLDL-c, very low-density lipoprotein-cholesterol.
Biochemical markers
The CAD patients with angina had significant high levels median (IQR) of inflammatory biomarkers, including plasma NF-κB (P = 0.001), serum TNF-α (P = 0.002), plasma IL-6 (P = 0.028), and serum hs-CRP (P = 0.049) compared with controls (Fig. 1 and Table 2). However, plasma MDA (P = 0.895) and serum homocysteine (P = 0.931) were not significantly elevated in the patients of CAD compared to controls. After covariates analysis, NF-κB, TNF-α, IL-6, and hs-CRP were significantly elevated, differentiating patients of CAD from controls. These inflammatory markers of atherosclerosis are raised due to CAD rather than the effects of confounders.

Comparison of inflammatory biomarkers of atherosclerosis between patients of CAD (n = 58) and controls (n = 55). CAD, coronary artery disease.
Comparison of Biochemical Markers and Angiography Scores Between Coronary Artery Disease Patients with Angina (n = 58) and Controls (n = 55)
Bold values indicate the Significant P value.
Data were expressed as median (inter quartile range); Mann–Whitney U test and ANCOVA (Quad's)* analysis between patients of CAD and control groups; P value <0.05 was significant.
CA, coronary artery; hs-CRP, high sensitivity C-reactive protein; hs-trop-I, high sensitivity troponin-I; IL-6, interleukin-6; MDA, malondialdehyde; NF-κB, nuclear factor kappa-B; TNF-α, tumor necrosis factor alpha.
ROC curve analysis
The ROC curve analysis (Fig. 2 and Table 3) revealed significant (P = 0.000) high area under curve [confidence interval (95% CI)] for plasma NF-κB 0.76 (0.65–0.85) with cutoff 4.9 ng/dL, sensitivity 73%, and specificity 65%. Similarly, serum TNF-α AUC was significantly (P = 0.000) elevated 0.72 (0.61–0.81) with cutoff 5.79 pg/mL and sensitivity and specificity of 71% and 69%, respectively. Plasma IL-6 was also significantly (P = 0.027) increased AUC 0.62 (0.52–0.71) with cutoff 3.95 pg/mL, sensitivity 64%, and specificity 53%, and serum hs-CRP was significantly (P = 0.033) elevated AUC 0.62 (0.52–0.71) with cutoff 2.0 mg/L, sensitivity 53%, and specificity 56% in CAD patients compared to controls.
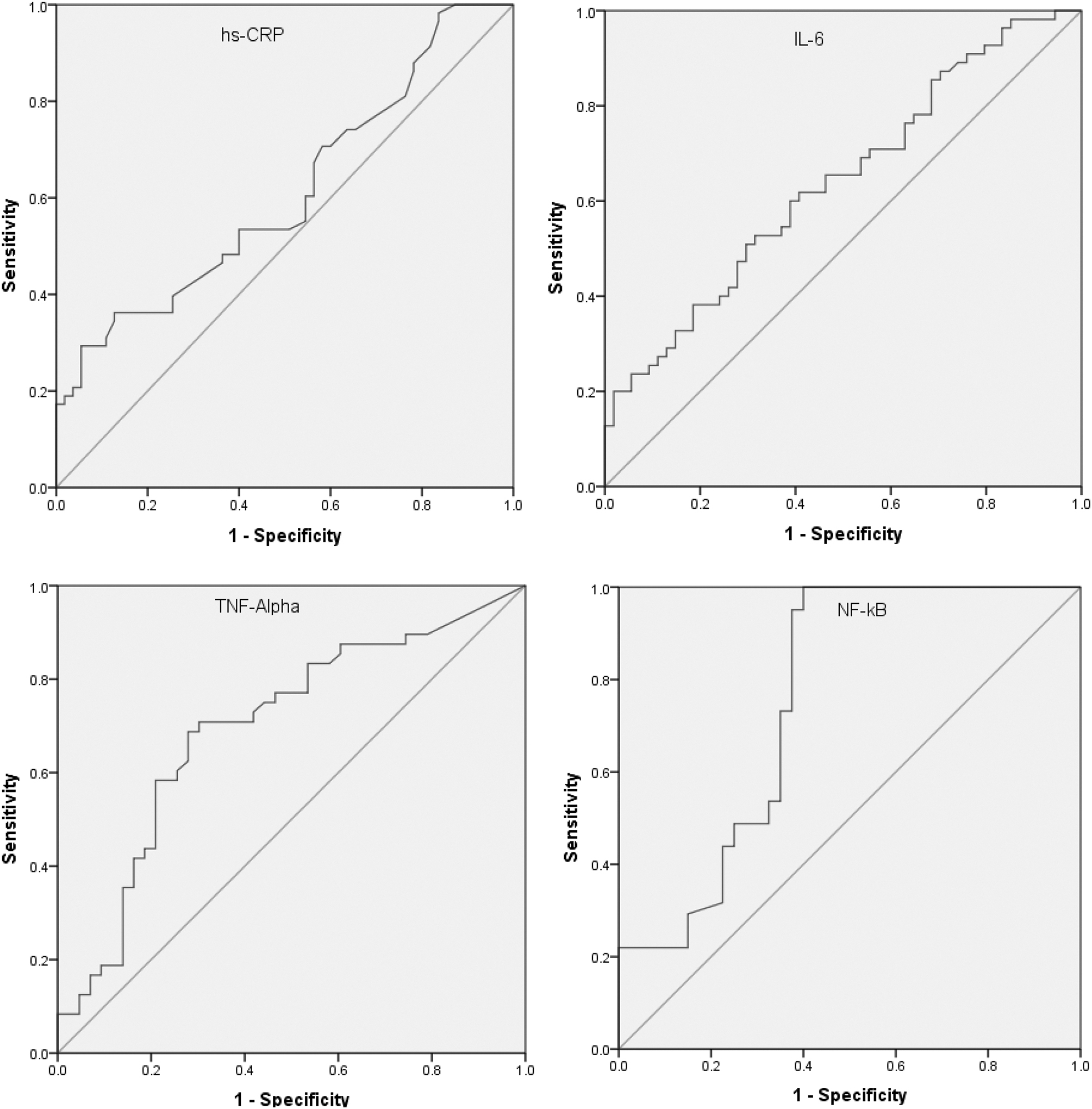
ROC curve analysis of inflammatory biomarkers of atherosclerosis between CAD patients with angina (n = 58) and controls (n = 55). ROC, receiver operating characteristic.
Diagnostic Accuracy Analysis of Biomarkers of Atherosclerosis in Patients of Coronary Artery Disease (n = 58) Compared to Controls (n = 55)
AUC, area under curve; CI, confidence interval; DOR, diagnostic odds ratio; LR, Likelihood ratio; NPV, negative predictive value; PPV, positive predictive value.
CombiROC analysis of NF-κB, TNF-α, IL-6, and hs-CRP classified CAD patients with angina compared to controls AUC = 0.83, sensitivity 80%, and specificity 80%. However, no discriminating (P = 0.895) values AUC 0.51 (0.36–0.63) were found for MDA and homocysteine AUC 0.51 (0.38–0.61), P = 0.931, for early diagnosis of CAD in patients with angina.
Correlation of biomarkers with angiography
In all patients, significant positive correlation was found for NF-κB, TNF-α, IL-6, and hs-CRP with coronary artery stenosis and GS (Table 4). Plasma NF-κB levels 4.9 to 7.9 ng/dL classified the patients into moderate CAD (50%–70% stenosis) and for critical CAD (>70% stenosis) plasma NF-κB levels >7.9 ng/dL.
Spearman's Correlations of Biomarkers with Stenosis of Coronary Artery and Gensini Score (N = 113)
Bold values indicate the Significant P value.
P = Significant (p < 0.05), R = Better Correlation.
Discussion
To the best of our knowledge, there are no previous studies available to find out the diagnostic accuracy of NF-κB in comparison to angiography for the patients of CAD. Inflammatory biomarkers of atherosclerosis are needed to be validated in comparison to angiography for early diagnosis of CAD in patients with angina. In developing countries, it is challenging to diagnose CAD at an early stage. This is due to lack of awareness of CAD and limited availability of Cath lab facility. In current practice, atherosclerosis in coronary arteries is diagnosed by invasive technique of angiography. However, we planned to assess CAD by inflammatory biomarkers in the patients with angina. Notably, missing diagnosis of ischemic heart disease at early stages may lead to increased risk of morbidity and mortality (Alessandra et al, 2013).
Out of the studied inflammatory biomarkers, NF-κB and TNF-α had best sensitivity for the diagnosis of CAD in patients with angina. This study showed that NF-κB can be used for the early diagnosis of CAD. In addition, NF-κB also classified minor, moderate, and critical CAD. This is probably due to the enhanced NF-κB signaling pathway involvement of IL-1, TNF α/β, and reactive oxygen species in the development of atherosclerosis. Oxidative stress, inflammation, hyperglycemia, and ionizing radiations induced production of NF-κB leading to vascular endothelial damage and enhancing further inflammation are responsible to develop atherosclerotic cardiovascular disease (Fan et al, 2018; Robson et al, 2018; Xu et al, 2020).
TNF-α was also revealed significantly elevated and having good diagnostic value in the patients with CAD. In literature, diagnostic accuracy for TNF-α showed odds ratio (OR) 1.011 (1.000–1.021), P = 0.052, and positive correlation (r = 0.51, P < 0.001) with GS in patients with CAD (Wainstein et al, 2017). In another study, CAD severity as assessed by GS was significantly and positively correlated with TNF-α (r = 0.30, P < 0.01), (Jones et al, 2005) similar to our study. TNF-α is secreted by macrophages, lymphocytes, natural killer cells, and vascular smooth muscle cells. TNF-α signaling is mainly mediated by NF-κΒ light-chain-enhancer of the activated B cell pathway, and this affects almost all cells involved in atherogenesis by promoting the expression of cytokines, adhesion molecules, migration, and mitogenesis of vascular smooth muscle and endothelial cells.
This study showed significant elevation of IL-6 in CAD patients with lesser sensitivity and specificity than few other researchers report. ROC curve analysis of plasma IL 6 AUC was 0.62 (0.52–0.71), relatively lower than another study of 0.754 (95% CI: 0.675–0.834, P < 0.01) for assessment of CAD with GS (Min et al, 2017). Diagnostic accuracy of IL-6 showed OR 1.036, (CI 1.017–1.055), P < 0.001, and positive correlation (r = 0.44, P < 0.001) with GS in patients of CAD (Wainstein et al, 2017). In another study, the results revealed that CAD severity as assessed by GS was significantly correlated with IL-6 (r = 0.51, P < 0.01), (Jones et al, 2005). The elevated levels of serum IL-1 and TNF-α stimulate the production of IL-6 from macrophages, lymphocytes, natural killer cells, and vascular smooth muscle cells that further enhance the process of inflammation-induced atherosclerosis.
Our study showed significant elevation of hs-CRP in CAD patients with lesser sensitivity and specificity than other inflammatory biochemical markers. In literature, the diagnostic accuracy of hs-CRP by ROC curve showed higher sensitivity 75% and specificity 69% at cutoff value of 5.77 mg/L and was found independent predictor of high Syntax score in patients with acute coronary syndrome (AUC = 0.775, P < 0.001), (Karadeniz et al, 2015). Various inflammatory mediators involved in the atherosclerosis, such as IL-6 and TNF-α, through transcriptional stimulation of CRP gene promote its release especially by hepatocytes (Del-Giudice and Gangestad, 2018; Sproston and Ashworth, 2018).
This study revealed significant positive correlation between NF-κB, TNF-α, IL-6, and hs-CRP with GS and stenosis of coronary arteries like other studies (Jones et al, 2005; Karadeniz et al, 2015; Wainstein et al, 2017). However, NF-κB and TNF-α independently had better diagnostic accuracy and correlation with stenosis in patients with CAD, than IL-6 and hs-CRP as biomarker of atherosclerosis. NF-κB and TNF-α release is more specific to inflammation and oxidative stress that lead to atherosclerosis in coronary arteries.
Limitations
All biomarkers of atherosclerosis were not analyzed, only selected biomarkers of atherosclerosis were analyzed. This was a single-center study with limited numbers of cases. Multiple centers validation studies may be conducted. Messenger RNA (mRNA) involved in the pathogenesis of NF-κB signaling pathway of atherosclerosis may be analyzed in further studies.
Conclusion
The inflammatory biomarkers of atherosclerosis have diagnostic role in early detection of CAD in patients with angina. NF-κB and TNF-α may be used as noninvasive biomarkers before undergoing angiography for discrimination of healthy individuals from CAD patients. NF-κB and TNF-α can also be used for diagnosis of CAD in medical set ups where Cath lab facilities are not available.
Footnotes
Authors' Contributions
S.T.A.G.: Conceptualization (lead), Data curation (lead), Formal analysis (lead), Investigation (equal), Project administration (equal), and Writing—original draft (lead). D.A.K.: Conceptualization (equal), Formal analysis (lead), and Writing—review and editing (lead). A.R.: Resources (equal), Supervision (lead), and Visualization (equal). Z.H.H.: Investigation (equal) and Validation (supporting). K.A.K.: Methodology (equal) and Software (supporting). F.U.H.: Resources (equal) and Writing—review and editing (supporting).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by National University of Medical Sciences, Rawalpindi.