
Abstract
Despite extensive research to decipher the immunological basis of coronavirus disease
Introduction
Coronavirus disease (COVID-19
COVID-19 mortality rates at the beginning of the pandemic ranged from 2.84% to 5.5%, which decreased approximately to 0.08% worldwide. Mortality rates peaked among elderly patients whose age was 75 years or older (Depalo, 2021; Velavan and Meyer, 2020). Unlike patients younger than 70 years, the average duration between the onset of symptoms and mortality was shorter than 14 days (11.5 days) in patients older than 70 years (Wang et al., 2020b). This indicates that elderly COVID-19 patients are highly susceptible to complications caused by SARS-CoV-2 variants of concern. Therefore, envisaging precision immunological biomarkers for elderly patients seems crucial for early therapeutic intervention.
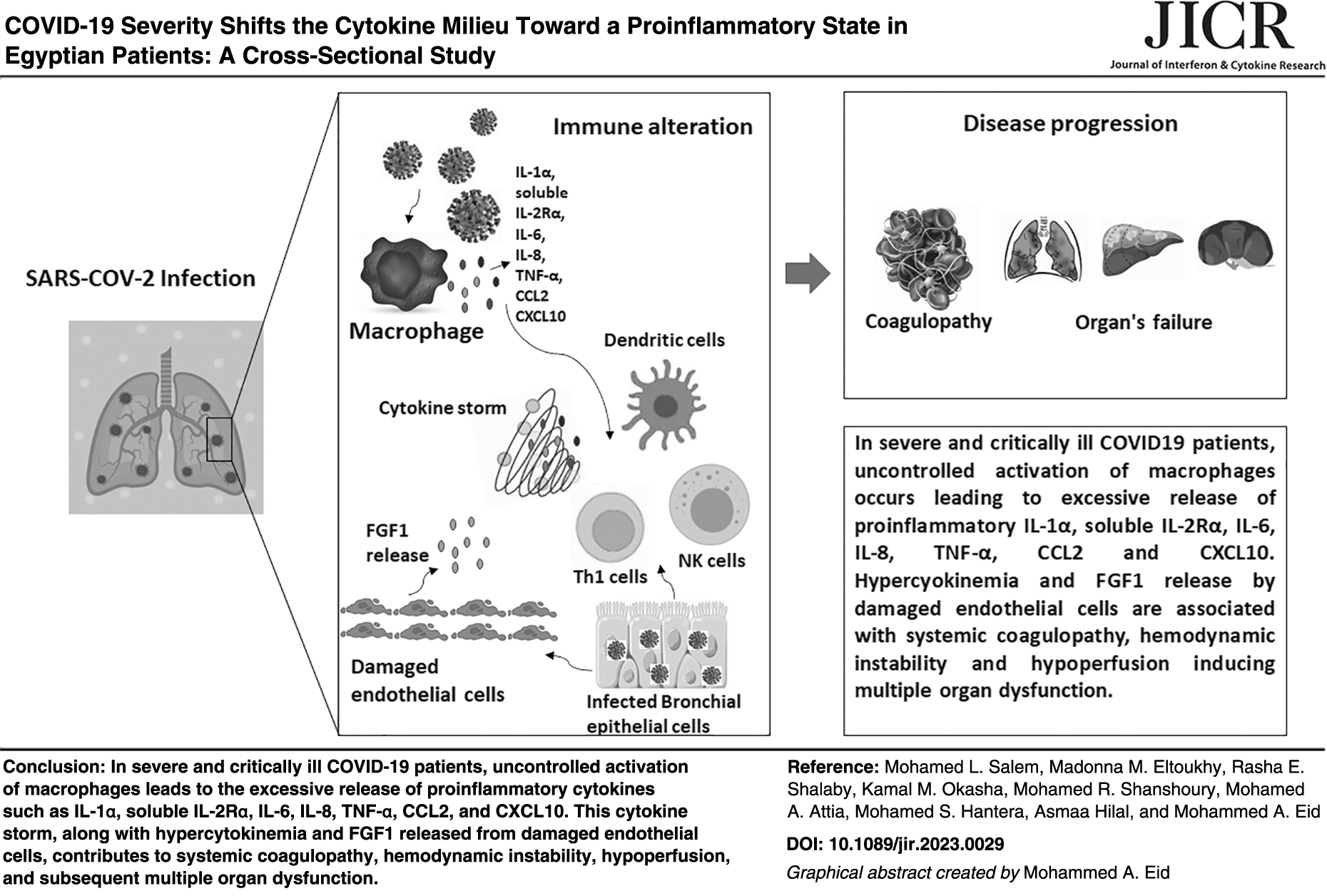
Most COVID-19 patients demonstrate lymphocytopenia and significantly high neutrophils, D-dimer, and C-reactive protein (CRP) levels in the blood; however, the predictive power of these parameters as precision biomarkers of disease outcome is still not fully established (Barrett et al., 2021; Gonçalves et al., 2021; Wang et al., 2020b). COVID-19 may also cause multi-organ dysfunction, presumably due to endotheliitis, loss of vascular integrity, and coagulation pathway activation (Perico et al., 2021). Additionally, a multi-organ hyperinflammatory state, known as cytokine storm or macrophage activation syndrome (MAC), usually ensues in severe and critically ill cases and inflicts tissue damage and fibrosis, particularly in the lungs (Que et al., 2022; Satyam et al., 2021). Varying levels of inflammatory cytokines, including interleukin (IL)-6 and tumor necrosis factor-alpha (TNF-α), have been detected in the plasma of COVID-19 patients, with the highest levels detected in severe cases (Tufa et al., 2022).
Some studies have proposed redefining COVID-19 as multiple organ dysfunction syndrome (MODS-CoV-2) because of its complex and systemic pathological sequelae. An essential dimension of MODS-CoV-2 in COVID-19 patients is the connection between deregulated inflammatory response and hypercoagulability state because of inflammatory injury to the microvasculature that activates the coagulation system leading to extensive microthrombosis (Chen et al., 2020a; Dennis et al., 2023; Tian et al., 2020; Wang et al., 2020a; Zhao et al., 2022). According to previous reports, 40% of COVID-19 patients are at risk of venous thromboembolism. Additionally, disseminated intravascular coagulation has been involved in 46% of COVID-19 deaths demonstrating that coagulation dysfunction is one of the primary causes of death in severe COVID-19 patients (Wang et al., 2020a; Wu and McGoogan, 2020).
The regulation of particular cytokines in COVID-19 patients and their potential relationship to immunopathology and coagulopathy have been the subject of numerous reports (Al-Ani et al., 2022; Lax et al., 2020; Plášek et al., 2022; Que et al., 2022; Savla et al., 2021). However, the ability to distinguish a protective COVID-19 immune response from an immunopathologic response across the severity spectrum of COVID-19 in individuals with various ethnic backgrounds has not been thoroughly analyzed (Kopel et al., 2020; Vadgama et al., 2022). Using a highly standardized Luminex xMAP multiplex assay, we comprehensively examined the levels of 25 cytokines previously shown to regulate antiviral immune response and anti-inflammatory and proinflammatory states in Egyptian COVID-19 patients of varying disease severity. Additionally, we have mapped the relatedness between immunological and clinical laboratory parameters using principal component analysis (PCA) for identifying predictive biomarkers of COVID-19 disease progression.
Materials and Methods
Study design and ethical approval statement
In a cross-sectional study, 78 adult COVID-19 patients were enrolled from the inpatient wards and the ICU Department of Tanta University Quarantine Hospital, Tanta, Egypt, between April 2020 and September 2020. Cases were selected to be older than 18 years and meet the COVID-19 virological case definition [positive detection of viral genome in nasopharyngeal swabs by reverse transcription-polymerase chain reaction (RT-PCR)]. Patients with more than one of the following chronic diseases, namely diabetes mellitus, hypertension, cardiac disease, and grade 2 or 3 liver disease, were excluded. Demographic and clinical data were collected as described in Table 1. The enrolled patients were classified into 4 groups according to the World Health Organization (WHO) clinical stage definition for COVID-19 as follows: 10 cases with mild infection, 18 cases with moderate illness, 30 cases with severe illness, and 20 critically ill cases. Twenty-one healthy control volunteers were also enrolled.
Demographic and Clinical Characteristics of COVID-19 Patients and Healthy Controls
Asterisks representa significant difference between the selected group with the healthy controls using 1-way ANOVA at P < 0.01.
ANOVA, analysis of variance; CRP, C-reactive protein; Hb, hemoglobin; M, mean; n, number of human subjects; PLT, platelet counts; SEM, standard error mean; WBC, white blood cells.
The detailed grouping criteria of enrolled participants are listed as follows: (1) healthy controls (CO) including individuals with no COVID-19 infection, no known contact with a confirmed or suspected COVID-19 case in the previous 14 days, no upper or lower respiratory tract infection, and no history of a serious chronic disease; (2) mild illness (MI) including individuals with laboratory-confirmed positive RT-PCR for SARS-CoV-2 who have any of the various signs and symptoms of COVID-19 (eg, fever, cough, sore throat, malaise, headache, muscle pain, nausea, vomiting, diarrhea, loss of taste and smell) but do not have complicated symptoms such as shortness of breath, dyspnea, or abnormal chest imaging;
(3) moderate illness (MO) including individuals with laboratory-confirmed SARS-CoV-2 infection who show evidence of lower respiratory disease during clinical assessment or imaging and have an O2 saturation (SpO2) ≥94% on room air; (4) severe illness (SE) including individuals with laboratory-confirmed SARS-CoV-2 infection and hospitalized with COVID-19 as a primary reason for admission with respiratory support [intubation, continuous positive airway pressure (CPAP), bilevel positive airway pressure (BiPAP)] who have SpO2 <94% on room air, respiratory frequency >30 breaths/min, or lung infiltrates >50% on CT chest; (5) critical illness (CL) including individuals with laboratory-confirmed SARS-CoV-2 infection and hospitalized with COVID-19 as a primary reason for admission and on respiratory support (intubation, CPAP, BiPAP) who have respiratory failure, septic shock, and multiple organ dysfunction.
The study protocol has been approved by the Ethical Committee Review Board, Faculty of Medicine, Tanta University (approval code “34112/9/20”). The sample size for healthy controls and COVID-19 cases was determined based on sample collection feasibility at the time of conducting the study.
Routine hematological parameters
Laboratory tests such as hemoglobin (Hb) level, total and differential white blood cells count, platelet counts (PLT), CRP, and the coagulation parameter, D-dimer, were assessed using standard clinical laboratory methods for all recruited participants.
Cytokine profiling using Luminex xMAP multiplex assay
A volume of 2 mL of peripheral blood samples was drawn from the enrolled participants and centrifuged directly at 13,000 rpm for 10 min to separate plasma (500μL). Plasma samples were then blindly coded and used for analysis. Luminex 200 xMAP Technology (Luminex Corp, Austin, TX) was used to measure plasma levels of a panel of 25 cytokines (kit catalog no. LXSAHM-25, and kit lot no. L137457). Briefly, 50 μL of plasma was diluted 2-folds and then incubated with magnetic beads (Molecular Probes; Life Technologies, Carlsbad, CA) coated with cytokine-specific capture antibodies. After several washes and incubation periods, the beads were detected with the Luminex system (Luminex Corp, Austin, TX). Data were obtained and calculated using a 5-parametric curve fit using xPONENT®, version 4.03, in a blinded manner with measurement performed with the FlexMAP3D system (Luminex Corp) (Datta et al., 2008).
Statistical analysis
Statistical analysis was performed using SPSS 26.0 for Windows (SPSS, Inc., Chicago, IL). The figures and graphs were prepared with GraphPad Prism 9.0. (La Jolla, CA). Pearson's correlation or Fisher's exact test was used as appropriate to compare the frequency of categorical variables. Means and standard error values for each continuous variable were calculated. The comparison of continuous variables between 2 groups was performed using the 1-way analysis of variance (ANOVA), and the correlation analysis was performed using Spearman's correlation analysis. A P-value <0.05 was considered statistically significant.
Results
Demographic and clinical criteria of enrolled study participants
The basic information of enrolled participants is listed in Table 1. We have enrolled 78 COVID-19 cases (59.5% males; mean age 53 years) and 21 healthy controls (58% male; mean age 34 years). No significant differences in gender, age, Hb level, white blood cells, and PLT were found among all patient groups (P > 0.05). The mean age of severe and critically ill patients was 1.2-fold higher than that of mild and moderate cases. Fever was the most prevalent symptom among patients (78.78%); however, higher temperatures were observed in severe and critically ill patients. D-dimer and CRP levels were significantly elevated in severe and critically ill patients (P ≤ 0.0001) compared with other groups, which may reflect active inflammation and hypercoagulable state in severe and critically ill patients. Furthermore, severe and critically ill patients had significant lymphopenia compared with other groups (P ≤ 0.0001). Similar results have been observed for oxygen saturation in severe and critically ill patients requiring assisted ventilation, indicating pulmonary dysfunction.
Upregulation of both proinflammatory and anti-inflammatory cytokines in severe and critically ill COVID-19 patients
The primary focus of our analysis was to measure the levels of proinflammatory cytokines potentially related to immunopathologic lung injury to monitor disease progression in COVID-19 patients, including IL-1α, soluble IL-2Rα, IL-6, IL-8, IL-18, CCL4, and TNF-α. These cytokines were only significantly upregulated in severe and/or critically ill cases who had very low oxygen saturation and required assisted ventilation compared (Fig. 1 and Table 1).
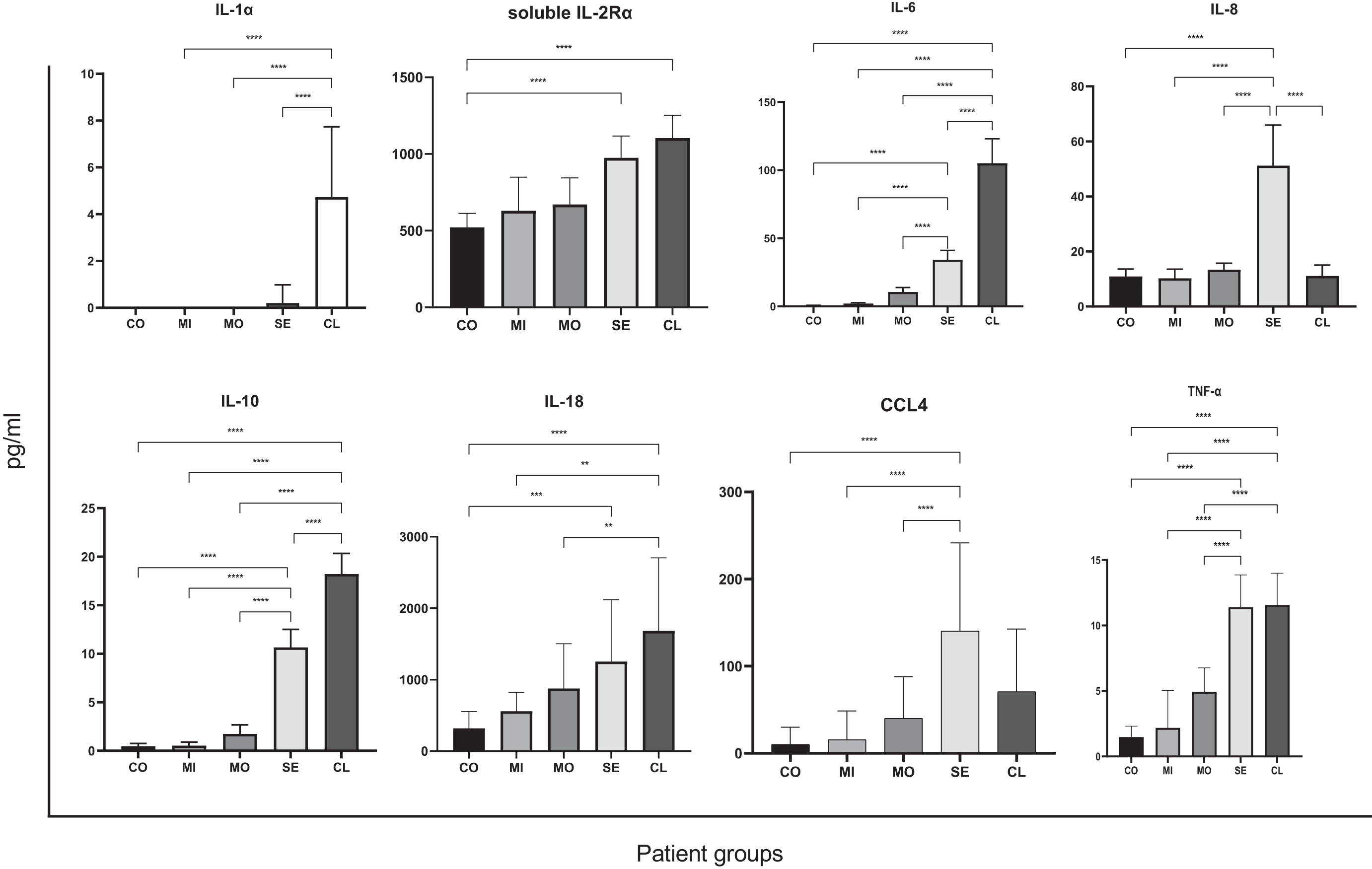
Levels of proinflammatory cytokines potentially related to lung injury and anti-inflammatory cytokines. Concentrations of IL-1α, soluble IL-2Rα, IL-6, IL-8, IL-10, IL-18, CCL4, and TNF-α were measured by Luminex assay 100/200 in plasma of 21 healthy controls (CO), 10 mild COVID-19 (MI), 18 moderate COVID-19 (MO), 30 severe COVID-19 (SE), and 20 critically ill COVID-19 (CL) cases. The mean cytokine levels plus standard errors from 2 independent analyses are shown. Asterisks represent a significant difference between the selected groups using 1-way ANOVA at P < 0.01. ANOVA, analysis of variance; IL, interleukin; TNF-α, tumor necrosis factor-alpha.
However, no significant difference was detected for the proinflammatory IFN-γ and CCL3 between patient groups, and the proinflammatory IL-1β, IL-2, IL-17, and TNF-β were not detected in the plasma of all enrolled patients (data not shown). Interestingly, the anti-inflammatory cytokine IL-10 was markedly upregulated in severe and critically ill patients compared with healthy controls and mild and moderate cases (Fig. 1).
Additionally, the proangiogenic FGF1 was significantly upregulated in severe and critically ill patients compared with healthy controls and/or patients with a milder form of the disease (Fig. 2).

Levels of proangiogenic cytokines and potentially associated cytokines with a hypercoagulable state in COVID patients. Concentrations of FGF1, CCL2, and CXCL10 were measured by Luminex assay 100/200 in plasma of 21 healthy controls (CO), 10 mild COVID-19 (MI), 18 moderate COVID-19 (MO), 30 severe COVID-19 (SE), and 20 critically ill COVID-19 (CL) cases. The mean cytokine levels plus standard errors from 2 independent analyses are shown. Asterisks represent a significant difference between the selected groups using 1-way ANOVA at P < 0.01.
Of note that the following immunomodulatory markers IL-3, IL-4, IL-5, IL-7, IL-13, IL-15, and Granulocyte-Macrophage Colony-Stimulating Factor showed no significant difference between patient groups (Fig. 3 and data not shown).
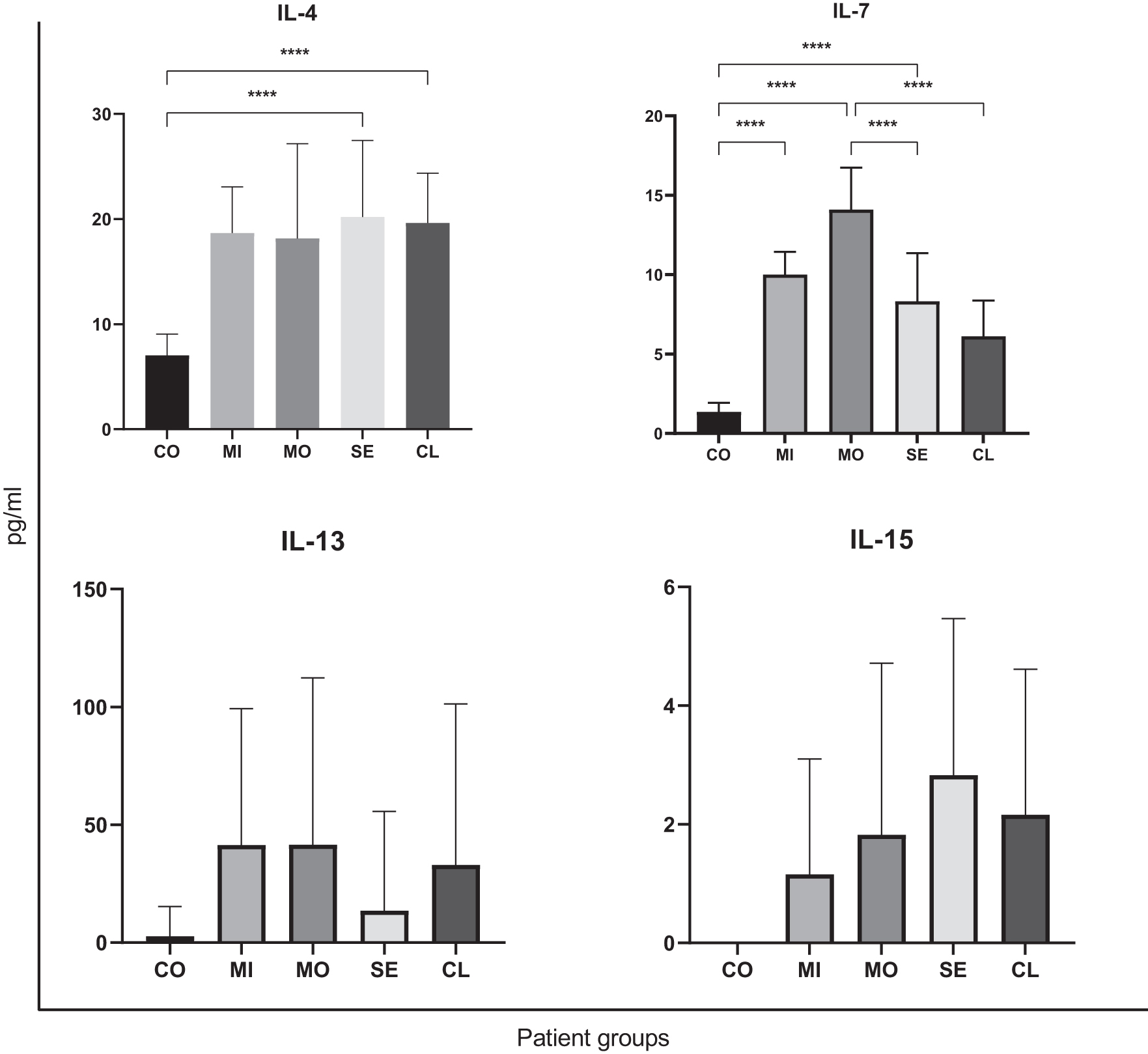
Levels of immunomodulatory cytokines in COVID-19 patients. Concentrations of IL-4, IL-7, IL-13, and IL-15 were measured by Luminex assay 100/200 in plasma of 21 healthy controls (CO), 10 mild COVID-19 (MI), 18 moderate COVID-19 (MO), 30 severe COVID-19 (SE), and 20 critically ill COVID-19 (CL) cases. The mean cytokine levels plus standard errors from 2 independent analyses are shown. Asterisks represent a significant difference between the selected groups using 1-way ANOVA at P < 0.01.
Upregulation of CCL2 and CXCL10 as potential hypercoagulability markers in critically ill cases
CCL2 and CXCL10 levels were significantly increased in the critically ill group compared with mild, moderate, and severe cases with extremely high levels of D-dimer (Fig. 2 and Table 1). Additionally, CXCL10 levels showed a strong positive correlation with D-dimer levels in COVID-19 patients (Fig. 4).
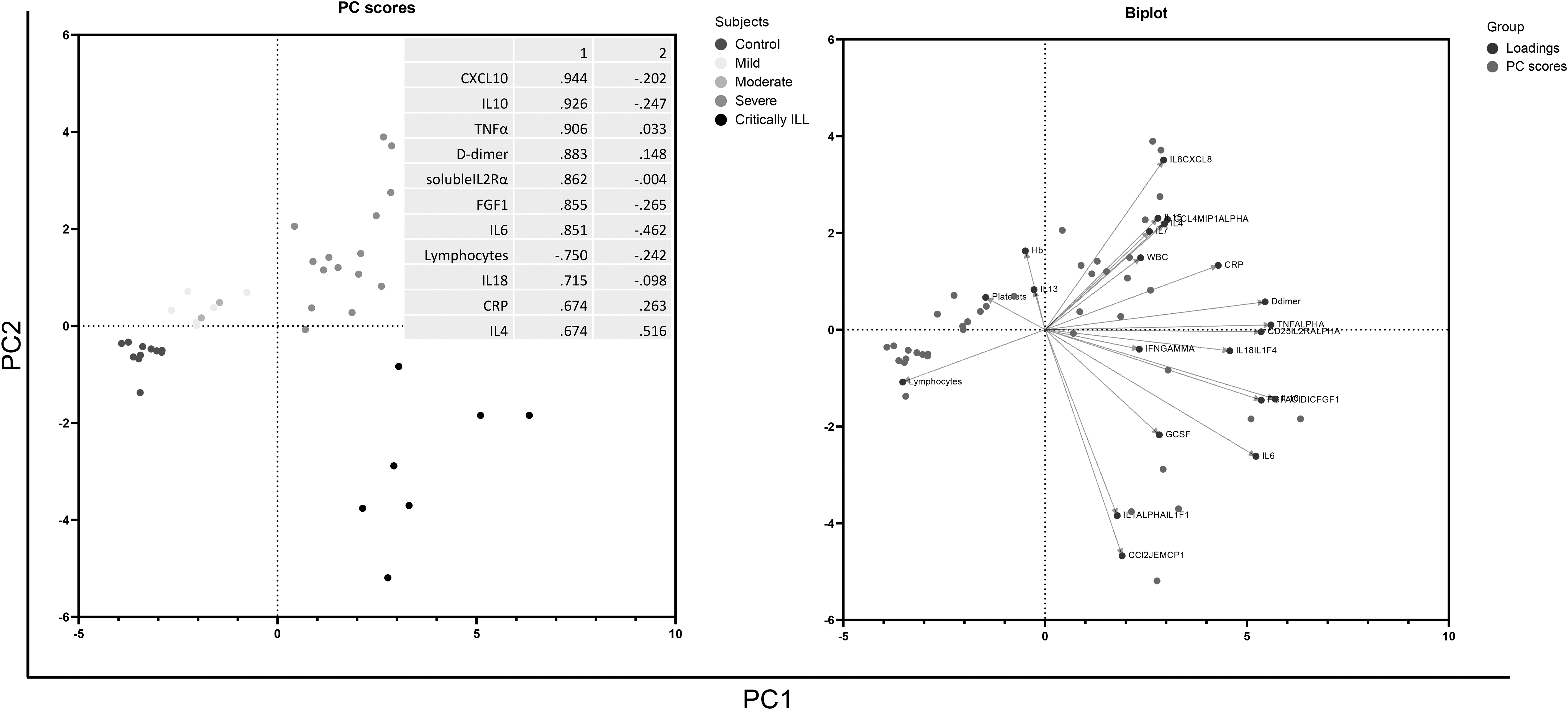
Distinct cytokine profiles related to COVID-19 severity. PCA of tested cytokines and different clinical parameters. The analysis identified 8 cytokines and 3 clinical parameters (CRP, D-dimer, and lymphocyte counts) that were important in explaining the observed variations between patient groups. PC1 and PC2 scores for the tested variables in the table rank the variables based on their influence on the observed variations between patient groups and determine the clustering of patient groups along PC1 and PC2. CRP, C-reactive protein; PCA, principal component analysis.
PCA identifies potentially predictive biomarkers of COVID-19 severity
To map the relationship between plasma cytokine levels, clinical parameters, and COVID-19 severity, we performed PCA for COVID-19 patients of various severity levels (Fig. 4). Proinflammatory markers, including CRP, soluble IL-2Rα, IL-6, IL-18, CXCL10, and hypercoagulability marker D-dimer mainly contributed to the first principal component and exhibited differential association with severe and critically ill patients. Likewise, the proangiogenic FGF1 clustered with severe and critically ill patients (Fig. 4).
Correlation analysis for the detected cytokines and clinical laboratory parameters showed variable relationships
To examine the potential interplay between the detected cytokines and clinical laboratory parameters, we have performed a correlation analysis between the levels of cytokines and clinical laboratory parameters throughout the COVD-19 clinical continuum (Fig. 5). The data showed a significant positive correlation between CCL2 and IL-6, CCL4, TNFα, CXCL10, D-dimer and CRP, IL-10, IL-15, IL-18, and soluble IL-2Rα, respectively (P ≤ 0.001). However, a significant negative correlation was observed between CCL2, TNF-α and Hb concentration, IL-2Rα, TNF-α, IL-10 and PLT, IL-2Rα and lymphocyte percentage, respectively (P ≤ 0.001). These findings reveal a potential interplay between hematological and inflammatory parameters in COVID-19 patients.

Correlation heat map for the measured cytokines and clinical parameters in various COVID-19 severity groups. Positive numbers represent a positive correlation, and negative numbers represent a negative correlation between the tested parameters. Color intensity determines the strength of the correlation.
Discussion
Cytokine-induced modulation of host immune response has been shown to play a critical role in governing the outcome of many potentially serious viral infections, including influenza, SARS-CoV, and MERS (Alhetheel et al., 2020; Cheung et al., 2005; Page et al., 2012; Zhou et al., 2014). A growing body of evidence suggests that the severity of COVID-19 is driven by disordered immunoregulation, which often results in ARDS, a leading cause of death in affected patients (Quan et al., 2021). However, there is a limited consensus on specific cytokine signatures that predict the clinical outcome and guide precision therapy of COVID-19 (Pereira et al., 2021; Wang et al., 2021). Moreover, high-throughput cytokine profiling is particularly understudied among Egyptian COVID-19 patients (Gharib et al., 2021; Shafiek et al., 2021). The present study aims to address the current gap by clustering hospitalized Egyptian COVID-19 patients of varying disease severity based on their cytokine profile.
Luminex xMAP technology was utilized to analyze 25 cytokines in plasma samples isolated from patients with varying degrees of COVID-19 severity, including proinflammatory cytokines potentially associated with lung damage in COVID-19 patients, such as IL-1α, IL-1β, IL-2, soluble IL-2Rα, IL-6, IL-17, IL-8, CCL3, CCL4, IFN-γ, TNF-α, and TNF-β. Additionally, we have examined cytokines potentially related to a hypercoagulable state such as CCL2, CCL3, and CXCL10. Finally, we have examined cytokines known to be essential for immune modulation, namely IL-1α, IL-3, IL-4, IL-5, IL-10, IL-13, IL-15, IL-17, IL-18, and TNF-β (Chen et al., 2021; Chen et al., 2020b; Chen et al., 2018; Huang et al., 2005; Jakobs et al., 2022; Julian et al., 2021; Robba et al., 2020; Zhang and An, 2007). Our comprehensive analysis identified distinct cytokine profiles throughout the COVID-19 severity spectrum, suggesting dysregulated adaptive immune responses with a proinflammatory cytokine shift that is exacerbated in higher COVID-19 severity levels.
Our profiling of cytokines demonstrated that the proinflammatory cytokines IL-2Rα, IL-8, IL-18, TNF-α, and CXCL10 were significantly upregulated in severe and/or critically ill COVID-19 patients compared with healthy controls or cases with milder forms of the disease (Figs. 1–3). Likewise, IL-4 and IL-15 levels demonstrated a similar, although nonsignificant, surging trend toward severe forms of COVID-19. Notably, IL-1α, IL-6, and CCL2 were exclusively upregulated in critically ill patients who had respiratory failure and required mechanical ventilation (Figs. 1 and 2).
However, IL-13 was downregulated in severe and critically ill COVID-19 patients, whereas no change was observed in IFN-γ level across all severity levels of COVID-19, suggesting compromised T-helper (Th)1 responses (Fig. 3 and data not shown). This profile is consistent with the development of hyperinflammatory status and MAC in severe and critical COVID-19 cases implying a potentially significant role of the host's innate immune responses in the immunopathology of COVID-19 (Cabaro et al., 2021; Dorgham et al., 2021; Gómez-Escobar et al., 2021; Gustine and Jones, 2021; Russick et al., 2021; Zhou et al., 2020).
The concurrent rise in the levels of macrophage inflammatory cytokines, including IL-1α, IL-18, IL-6, IL-8, TNF-α, CXCL10, and CCL2 in severe or critically ill patients (Figs. 1–3), has also been reported by other research groups (Abers et al., 2021; Cabaro et al., 2021; Dorgham et al., 2021; Gómez-Escobar et al., 2021; Russick et al., 2021; Satış et al., 2021; Zhou et al., 2020). Multiple studies have suggested that high levels of the proinflammatory cytokines IL-1 and IL-6 in COVID-19 patients may predict poor disease outcomes, including MAC and ARDS (Han et al., 2020; Russick et al., 2021; Shafiek et al., 2021).
However, clinical trials incorporating IL-1 and IL-6 inhibitors in the treatment protocols of COVID-19 patients demonstrated variable results without a significant improvement in disease outcomes (Mariette et al., 2021; Stone et al., 2020). These data imply that the concerted action of macrophage cytokines potentially governs the outcome of COVID-19. Therefore, it has also been proposed that a combination of these cytokines may be used as prognostic markers to predict COVID-19 severity (Bhaskar et al., 2020). In agreement with our results, other research groups have demonstrated that CCL2 and CXCL10 levels were significantly elevated in severe COVID-19 cases. Specifically, a high CXCL10 level has been associated with ARDS development and respiratory failure (Cabaro et al., 2021).
The immune modulator IL-18, a vital member of the IL-1 cytokine family, has been demonstrated to play a crucial role in promoting the development of MAC and cytokine release syndrome in various autoinflammatory conditions (Weiss et al., 2018). Our data show a significant increase in IL-18 levels in severe and critically ill cases compared with healthy controls and patients with milder forms of the disease (Fig. 3). In congruence with our findings, other studies have detected high levels of IL-18 among COVID-19 patients with severe pneumonia, which also correlated with mortality and poor disease outcomes (Gómez-Escobar et al., 2021; Satış et al., 2021).
However, contradictory evidence from a different study showed that mortality in critically ill COVID-19 patients who required extracorporeal membrane oxygenation correlated with low levels of IL-18 (Dorgham et al., 2021). These data suggest that unraveling the ultimate role of this cytokine in COVID-19 pathogenesis requires further elucidation of the molecular mechanisms and the immunological contexts regulating its function.
The observation that the proinflammatory TNF-α, IL-8, and IL-2Rα were significantly upregulated in severe COVID-19 patients has been corroborated by other studies (Fig. 1) (Dorgham et al., 2021; Kaya et al., 2021; Ma et al., 2021; Zhang et al., 2020). Notably, one study has shown that high levels of soluble IL-2Rα in blood from severe COVID-19 patients are inversely correlated with T cell numbers. The same study has also shown that the in vitro addition of recombinant IL-2Rα could inhibit the proliferation and function of activated T cells derived from peripheral blood mononuclear cells. These data signify that high IL-2Rα levels may play a role in compromising adaptive immune responses and COVID-19 prognosis (Zhang et al., 2020).
Additional studies have associated high levels of IL-8 and IL-2Rα in severe COVID-19 cases with prolonged illness, respiratory failure, and higher mortality rates (Dorgham et al., 2021; Kaya et al., 2021; Ma et al., 2021). These data suggest a complex interplay between distinct cytokines in governing COVID-19 outcomes. The data may also suggest a potential protective role of IL-2 signaling in restoring T cell responses or delaying the onset of compromised T cell responses (Zhang et al., 2020).
T-helper (Th) polarization is well known as a critical determinant of the outcome of various viral infections (Calarota and Weiner, 2004; Kamperschroer and Quinn, 2002; Neidleman et al., 2020; Roncati et al., 2020). By profiling Th2-related cytokines, namely IL-4, IL-6, and IL-10, their levels were modestly upregulated among patients with more severe forms of COVID-19 (Figs. 1 and 3), whereas IL-15 displayed a modest increase across all COVID-19 severity levels (Fig. 3), and these data are consistent with other similar studies (Gil-Etayo et al., 2021; Kandikattu et al., 2020; Petrey et al., 2021; Vaz de Paula et al., 2020). Conversely, the anti-inflammatory cytokine IL-13, secreted by activated Th2 cells, was differentially downregulated in severe COVID-19 cases (Fig. 3).
Contradictory evidence from various studies demonstrated high IL-13 levels in severe COVID-19 patients who developed ARDS, lung damage, and acute renal failure (Donlan et al., 2021; Petrey et al., 2021; Vaz de Paula et al., 2020). On the contrary, other studies suggested that higher expression levels of IL-4 and IL-13 in asthmatic patients may lower the risk of developing severe COVID-19 due to the downregulation of angiotensin-converting enzyme-2 receptors (Song et al., 2021).
Interestingly, our PCA revealed that severe and critically ill patients with high mortality rates exhibited distinguishing cytokine signatures from mild and moderate COVID-19 patients. Specifically, the observed variations between early and late stages of COVID-19 disease can be primarily attributed to the levels of IL-2Rα, IL-6, IL-10, IL-18, TNF-, FGF1, and CXCL10. Our PCA also demonstrated that the described immunological markers positively correlate with high D-dimer and CRP levels and inversely correlate with lymphocyte counts in severe and critically ill patients (Fig. 4). In addition, a significant positive correlation was detected between IL-2Rα and IL-10, IL-15, IL-18, and TNF-α (Fig. 5). These data raise the hypothesis that SARS-CoV2 might dysregulate the adaptive immune response by disturbing the balance between the Th1 and Th2 responses. Further characterization of individual cytokine functions and cytokine cross talk in future studies may define stage-specific roles of cytokine signaling in governing COVID-19 disease outcomes.
To the best of our knowledge, this is the first study to perform a high-throughput cytokine analysis spanning the whole COVID-19 severity spectrum and show an apparent proinflammatory cytokine surge among severe and critically ill COVID-19 patients from Egypt. Despite that, the reported variability for some of the data points could be attributed to the small sample size and to receiving dexamethasone therapy by COVID-19 patients. Further molecular characterization of cell-type-specific responses to individual cytokines using systems biology approaches may explain the reported interpatient variability and allow envisaging novel precision diagnostic, prognostic, and therapeutic modalities for COVID-19.
Footnotes
Authors' Contributions
Conceptualization: M.A.E. Methodology: M.L.S., M.M.E., R.E.S., K.M.O., M.R.S., M.A.A., M.S.H., A.H., and M.A.E. Formal analysis: M.L.S., R.E.S., and M.A.E. Software: M.A.E. Investigation: M.L.S., R.E.S., and M.A.E. Data curation: M.L.S., R.E.S., and M.A.E. Supervision: M.L.S., R.E.S., and M.A.E. Writing—original draft preparation: R.E.S. and M.A.E. Writing—review and editing: all authors read and approved the final article.
Ethical Approval and Consent to Participate
This study complies with all relevant ethical regulations. The experimental protocol was established according to the International Ethical Guidelines for Biomedical Research Involving Human Subjects and were approved by the Ethical Committee Review Board, Faculty of Medicine, Tanta University, Tanta, Egypt, granted this cross-sectional study (approval code “34112/9/20”).
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was funded entirely by Tanta University, Tanta, Egypt, through a project (TU:20-03-04).