
Abstract
Cytokines are major players in orchestrating inflammation, disease pathogenesis, and severity during COVID-19. Members of the interleukin (IL)-10 family of cytokines play important roles in regulating immune responses to various inflammatory and infectious diseases. However, the role of the IL-10 family of cytokines in COVID-19 remains elusive. Hence, we determined the plasma levels of the IL-10 family of cytokines (IL-10, IL-19, IL-20, IL-22, and IL-24) in 7 groups of COVID-19 individuals, based on days since real-time reverse transcriptase-polymerase chain reaction confirmation of SARS-CoV-2 infection. Our data show that the levels of IL-10, IL-19, IL-20, IL-22, and IL-24 cytokines decreased from days 15–30 to days 61–90 and plateaued thereafter. Severe COVID-19 patients exhibit increased plasma levels of IL-10, IL-19, IL-20, IL-22, and IL-24 compared to mild patients. Thus, our study provides evidence of alterations in the plasma levels of the IL-10 family of cytokines in convalescent COVID-19 individuals.
Introduction
The disease caused by the coronavirus SARS-CoV-2, known as COVID-19, has impacted over 655 million individuals worldwide and led to a staggering death toll of 6.6 million (report, 2023) (
Cytokines that are members of the interleukin (IL)-10 family are potent regulators of the immune system, exhibiting multifaceted roles. The IL-10 cytokine family is composed of IL-10, IL-19, IL-20, IL-22, and IL-24 (Ouyang and O'Garra, 2019). These cytokines signal through receptors on leukocytes and epithelial cells, thus improving natural defense mechanisms and repairing tissues (Ouyang and O'Garra, 2019; Rutz et al., 2014). Research on these proteins has uncovered their significant and essential role in the maintenance of tissue homeostasis and the immune response in various disorders, including inflammatory bowel disease, ulcerative colitis, Crohn's disease, psoriasis, and rheumatoid arthritis (Ouyang and O'Garra, 2019). The rapid increase in IL-10, a cytokine that is traditionally thought of as anti-inflammatory, appears to be a sign of hyperinflammation in people with severe COVID-19 disease (Chen et al., 2020; Huang et al., 2020; Lu et al., 2021; Qin et al., 2020). Some studies suggest that high IL-10 levels can lead to worse outcomes in COVID-19 patients, and the levels were associated with pro-inflammatory markers like CRP and IL-6 (Han et al., 2020; Islam et al., 2021; Zhao et al., 2020). A recent meta-analysis looking at 1,242 nonsevere and 915 severe patients with COVID-19 disease from 18 clinical trials found that IL-6 and IL-10 were covariates that were predictive of disease severity (Dhar et al., 2021; Lu et al., 2021). Recent studies indicated that the elevated levels of IL-10 is associated with critical illness of COVID-19 (Han et al., 2020; Yang et al., 2021; Zhao et al., 2020). IL-22 has been demonstrated to be a pro-inflammatory agent, as it has been shown to stimulate the expression of cytokines, such as IL-1β, IL-17, and tumor necrosis factor-alpha (TNF-alpha), among other cytokines. The protective and pro-inflammatory effects of IL-22 appear to be contingent upon the coproduction of relevant cytokines between the relevant cells at various stages of the disease (Fang et al., 2022; Rutz et al., 2014; Sabat et al., 2014). In comparison to healthy controls, the number of individuals with asymptomatic, mild, and severe pneumonia increased significantly in adult COVID-19 patients, with a significant increase in IL-22+, Tc22, and Th22 cells (Fang et al., 2022). Studies suggest that the pathway of IL-22 (IL-22-R1) plays a role in the pathogenesis of the COVID-19 disease (Albayrak et al., 2022; Fang et al., 2022; Klooster et al., 2021).
However, the impact of COVID-19 disease on the other IL-10 family of cytokine (IL-19, IL-20, and IL-24) levels has not been explored well. Based on the previous literature, we hypothesized that the severity of COVID-19 disease is associated with elevated levels of the IL-10 family of cytokines and that the systemic levels of these cytokines would decrease in convalescent individuals over a period of time. Therefore, we examined the impact of SARS-CoV-2 on the IL-10 family of cytokine responses in different groups of COVID-19-diseased individuals at different time points following real-time reverse transcriptase-polymerase chain reaction (RT-PCR) confirmation for SARS-CoV-2 infection.
Materials and Methods
Study population
Individuals with acute COVID-19 symptoms (15–30 days from RT-PCR confirmation, n = 46) and Recovered COVID-19 patients (categorized by days postinfection as 31–60, n = 33; 61–90, n = 38; 91–120, n = 34; 121–150, n = 32; 151–180, n = 37; and >180, n = 40), residing in Chennai and Thiruvallur, were recruited to the study between November 2020 and December 2020, after obtaining their informed consent. Individuals who were actively infected with SARS-CoV-2 within 0–15 days of RT-PCR confirmation were excluded from the study. Healthy control samples collected from the prepandemic period were used as controls (n = 44). The range of ages was 18 to 75 years. The same cohorts were used in earlier studies (Rajamanickam et al., 2022; Rajamanickam et al., 2022a; Rajamanickam et al., 2022b; Rajamanickam et al., 2021a; Rajamanickam et al., 2021b).
The blood samples from COVID-19 and control individuals were drawn into EDTA tubes (BD Biosciences) and transported to NIH-International Center for Excellence in Research (NIH-ICER), Chennai. Upon sample receipt, plasma was obtained by centrifugation and frozen at −80°C until serological and immunological analysis.
RT-PCR testing
RT-PCR testing for SARS-CoV-2 was conducted in laboratories approved by the government. To summarize, health care providers took nasopharyngeal and/or oropharyngeal swabs from suspected SARS-CoV-2 patients. RNA was extracted and purified from the specimens, then reverse transcribed into cDNA, and amplified. The thermocycling process consisted of 30 min at 48°C for reverse transcription, 10 min at 95°C for activation of the DNA polymerase, and 45 cycles of 15 s at 95°C and 1 min at 60°C. The cycle threshold (CT) value for each sample was computed by measuring the fluorescence and identifying the moment at which it eclipsed a limit established at the mean plus 10 standard deviations above the baseline. A positive test result was indicated by 2 or more positive tests (CT <45 cycles) from SARS genomic targets and all control reactions giving the expected range of positive and negative results.
People who did not show any signs during their sickness were categorized as asymptomatic, whereas those who needed oxygen support therapy or were hospitalized in the ICU for oxygen support were categorized as severely ill. The remaining people were placed in the mild illness group. Sample collection occurred between days 15–30 and beyond 180 days. Table 1 displays demographic details and other clinical parameters.
Demographics and Clinical Parameters of the Study Population
Data were shown as median, mean, n (%), or n (%). P values were calculated by χ2 test, or Fisher's exact test, as appropriate.
RT-PCR, real-time reverse transcriptase-polymerase chain reaction.
Institutional ethics committee statement
The study was approved by the Ethics Committees of NIRT (NIRT-INo: 2020047) and NIE (NIE/IHEC/202008-01).
Informed consent statement
Informed written consent was obtained from all participants. All the methods were performed in accordance with the relevant Institutional Ethics Committee guidelines.
Hematology
The Act-5 Diff hematology analyzer (Beckman Coulter) was utilized to conduct hematology assessments on all subjects.
Enzyme-linked immunosorbent assay
The DuoSet ELISA Kit (R&D Systems) was utilized to quantify the levels of IL-10, IL-19, IL-20, IL-22, and IL-24 in circulation through Enzyme-linked immunosorbent assay (ELISA), and 100 μl of plasma samples were utilized in duplicate for each experiment as directed by the manufacturer. The minimum detectable limits were as follows: IL-10 − 31.25 pg/mL, IL-19 − 31.2 pg/mL; IL-20 − 62.5 pg/mL; IL-22 − 31.2 pg/mL; and IL-24 − 62.5 pg/mL.
Statistical analysis
The analysis of data was executed with GraphPad PRISM (GraphPad Software, Inc., San Diego, CA). Cytokine levels were subjected to cross-sectional analysis through Kruskal–Wallis and Dunn's multiple comparison test. For measuring central tendency, geometric means (GM) were used. To compare mild to severe conditions and identify statistically significant differences, the nonparametric Mann–Whitney U test was used.
Results
Study population characteristics
The demographics, clinical, and hematological characteristics of the study population are shown in Tables 1 and 2 as previously described (Rajamanickam et al., 2022; Rajamanickam et al., 2022a; Rajamanickam et al., 2022b; Rajamanickam et al., 2021a; Rajamanickam et al., 2021b). The median age ranges from 36 to 45.5 years among the groups. In all the groups, the female number was slightly higher than the number of male patients. However, they were not statistically different among the groups. Individuals with hypertension were 26% in the acute phase group, and in the remaining groups, that is, 31–60 days to >180 days, the percentage ranged from 18% to 30%. Individuals with diabetes mellitus were 19% in the acute phase, and in the remaining groups, that is, 31–60 days to >180 days, the percentage ranged from 19% to 30%. Individuals with asthma were 5% in the acute phase and in the remaining groups, that is, 31–60 days (6%), 61–90 days (3%), 91–120 days (3%), and 151–180 days (3%).
Hematological Parameters of the Study Population
MCH, mean cell hemoglobin; MCHC, mean corpuscular hemoglobin concentration; MCV, mean corpuscular volume; RBC, red blood cells; RDW, red cell distribution width; WBC, white blood cells.
The other clinical symptoms such as fever, cough, chills, sore throat, runny nose, loss of taste and smell, muscle aches, joint pain, abdominal pain, vomiting, and diarrhea were present almost in all the groups. Individuals with seizures were 3% in 31–60 days alone, and neuro-related disorders were 5% in the 61–90 days group alone. Three percent of chronic kidney diseases were in 91–120 days and >180 groups of individuals. Individuals with heart diseases were 6% in 15–30 days group, 3% in 31–60 days group, and 3% in 61–90 days group. Seven percent of the severely diseased were with heart diseases. Individuals with rheumatic fever were 3% in 61–90 days and 3% in 151–180 days. Individuals treated with corticosteroids were 15–30 days (9%), 31–60 days (9%) and 61–90 days (5%), 91–120 days (10%), 121–150 days (3%), and 151–180 days (3%) and severely diseased (20%) groups. Individuals treated with antiviral drugs were 15–30 days (9%), 31–60 days (15%) and 61–90 days (5%), and 91–120 days (13%) and severely diseased (27%) groups. Among the severely infected group, 40% required hospitalization. To this end, we combined all the groups irrespective of their disease status (mild, moderate, severe, and convalescence) based on their time to positive for SARS-CoV-2 by RT-PCR.
Diminished circulating levels of the IL-10 family of cytokines in convalescent COVID-19 individuals over a period of time
To assess the levels of the IL-10 family of cytokines among individuals who have recovered from COVID-19, we assessed the levels of circulating IL-10, IL-19, IL-20, IL-22, and IL-24 in 7 different groups. Our comparative analysis, as shown in Fig. 1, revealed significant variations across the 7-time intervals. Most of the cytokines belonging to the IL-10 family (namely IL-10, IL-19, IL-22, and IL-24) exhibited a gradual and consistent decrease from days 15–30 to 150 days, followed by a plateau. IL-20 levels, on the other hand, showed a steady decline from days 121–150 to beyond 180 days. Finally, all the cytokines belonging to the IL-10 family were found to be significantly lower in the control group compared to both the acute and convalescent groups. Therefore, after COVID-19 recovery in individuals, plasma levels of cytokines from the IL-10 family gradually decline.

Decreasing circulating levels of the IL-10 family of cytokines in convalescent COVID-19 individuals over a period of time. Examination of the IL-10 group of cytokines (IL-10, IL-19, IL-20, IL-22, and IL-124) from COVID-19 diseased patients in the acute and recovery phases was categorized into 7 groups according to the number of days since RT-PCR confirmation 31–60 days, n = 33; 61–90 days, n = 38; 91–120 days, n = 34; 121–150 days, n = 32; 151–180 days, n = 37, more than 180 days, n = 40; and controls n = 44) and juxtaposed with individuals who were in good health. The information is illustrated as box and violin plots with each dot representing an individual. The dark line indicates the median, and the dotted line indicates quartiles. The P values were computed by utilizing the Kruskal–Wallis test with Dunn's post hoc analysis for multiple comparisons. P < 0.05 values were considered statistically significant. IL, interleukin; RT-PCR, real-time reverse transcriptase-polymerase chain reaction.
Severe COVID-19 disease is associated with increased circulating levels of the IL-10 family of cytokines
Subsequently, we aimed to assess the levels of the IL-10 cytokine family in COVID-19 patients with mild and severe symptoms. The results depicted in Fig. 2 revealed that the circulating levels of IL-10 (GM of 30.29 pg/mL in control, 450 pg/mL in mild, 734.8 pg/mL in severe), IL-19 (GM of 74.73 pg/mL in control, 357 pg/mL in mild, 449.6 pg/mL in severe), IL-20 (GM of 160.3 pg/mL in control, 551.8 pg/mL in mild, 762.6 pg/mL in severe), IL-22 (GM of 56.92 pg/mL in control, 293.4 pg/mL in mild, 582.3 pg/mL in severe), and IL-24 (GM of 119.8 pg/mL in control, 275 pg/mL in mild, 362 pg/mL in severe) were significantly elevated in COVID-19 patients with severe symptoms compared to those with mild symptoms. The levels of all the IL-10 family of cytokines (IL-10, IL-19, IL-20, IL-22, and IL-24) were significantly decreased in the control group compared with the mild and severe COVID-19 group of individuals. Hence, it can be inferred that severe COVID-19 cases are linked to elevated levels of the IL-10 cytokine family.
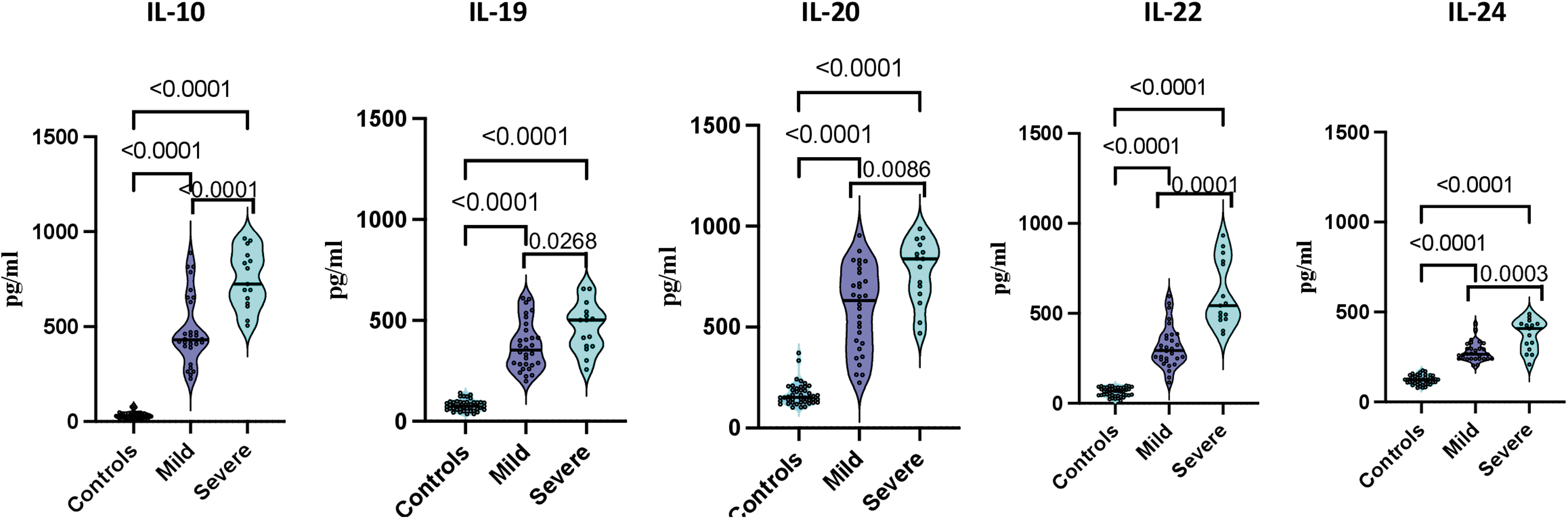
Severe COVID-19 disease is associated with increased circulating levels of the IL-10 family of cytokines. Plasma concentrations of cytokines from the IL-10 family (IL-10, IL-19, IL-20, IL-22, and IL-124) were measured in controls (n = 44), mild (n = 30), and severe (n = 15) COVID-19 cases between days 15 and 60 after RT-PCR confirmation. The information is illustrated as box and violin plots with each dot representing an individual with each circle representing an individual. The dark line indicates the median, and the dotted line indicates quartiles. Statistical significance was determined using the Kruskal–Wallis test with Dunn's post hoc analysis for multiple comparisons. P < 0.05 values considered as statistically significant.
Discussion
The group of cytokines known as IL-10 family encompasses 9 constituents: IL-10, IL-19, IL-20, IL-22, IL-24, IL-26, IL-28, and IL-29. These cytokines promote an array of host protective mechanisms, in response to various diseases and inflammatory conditions, mostly from epithelial cells (Ouyang and O'Garra, 2019). The role of the IL-10 family cytokines is highly varied, encompassing both pro-inflammatory and anti-inflammatory effects, as well as the ability to protect and regenerate tissues. These cytokines can stimulate innate immune responses in epithelial tissues, which can help to mitigate the harm caused by viral and bacterial infections (Ouyang and O'Garra, 2019; Wang et al., 2019). These proteins are not only necessary for protecting the host against different microorganisms but also crucial for returning the host to an immune calm state and maintaining tissue stability following an inflammatory reaction (Moore et al., 2001; Ouyang and O'Garra, 2019; Wang et al., 2019).
As far as we know, this investigation is the first to conduct an exact analysis of plasma concentrations of the IL-10 cytokine family in acute COVID-19 disease and various classes of recovered COVID-19 patients (7 categories distinguished by the time elapsed since diagnosis). We have categorized convalescent COVID-19 subjects into distinct groups according to the length of time since the RT-PCR detection (the most accurate sign of infection), which spans from 31–60 days to over 180 days.
This investigation demonstrates that the plasma concentrations of the cytokines belonging to the IL-10 family, namely IL-10, IL-19, IL-20, IL-22, and IL-24, exhibited a declining trend from days 15–30 to days 151–180. In addition, heightened plasma levels of IL-10, IL-19, IL-20, IL-22, and IL-24 were observed in severe COVID-19 patients, suggesting the involvement of the IL-10 family of cytokines in the pathogenesis of COVID-19 disease. Our results demonstrate that the kinetics of the IL-10 family of cytokines over a period of time in convalescence is similar to the levels of pro-inflammatory cytokines such as TNF-alpha, IL-1β, and IL-6 levels, which also decreased over the period of time (Queiroz et al., 2022; Shuwa et al., 2021; Silva-Junior et al., 2023; Yang et al., 2021).
Numerous studies have shown that people with COVID-19 disease who experience severe symptoms have high levels of the cytokine IL-10, which has anti-inflammatory properties. The immune characteristics observed in COVID-19-diseased patients who are critically ill and have considerably elevated levels of IL-10 in the circulation have resulted in the proposition that IL-10 could potentially contribute to the pathological advancement of the COVID-19 disease (Chen et al., 2020; Huang et al., 2020; Lu et al., 2021; Qin et al., 2020). According to the findings of a recent meta-analysis, IL-6 and IL-10 levels in patients can be used to predict the severity of COVID-19 disease (Dhar et al., 2021).
Following the symptom onset (Liu et al., 2020; Lucas et al., 2020) or hospitalization (Hue et al., 2020), the concentrations of IL-10 in the blood were observed to gradually decrease within a period of 2–3 weeks or upon the improvement of symptoms (Diao et al., 2020). Consistent with previous reports, we also observed that the levels of IL-10 significantly decreased over the period of infection, and increased levels of IL-10 were associated with severe COVID-19 disease. These alterations could be because IL-10 is widely recognized to aid in the alleviation of inflammation and tissue restoration, as well as in shielding against tissue harm in autoimmune illnesses (Ouyang and O'Garra, 2019; Saraiva et al., 2020).
IL-19, IL-20, and IL-24 are cytokines that share the common IL-20RA/IL-20RB and IL-22RA/IL-20RB receptors (Logsdon et al., 2012). Saheb Sharif-Askari et al. (2022) determined that the expression of IL-19 and its receptor, IL-20RB/IL-20R2, increased in both plasma and saliva after SARS-CoV-2 infection, and this upregulation was linked to the severity of the disease. The IL-19 concentration remained consistently high during the initial infection with SARS-CoV-2 and during the acute or hyperinflammatory stage (Liao et al., 2004; Matsuyama et al., 2020; Saheb Sharif-Askari et al., 2022). In accordance with previous reports, we observed that the levels of IL-19 significantly decreased over the period of infection and increased levels of IL-19 associated with severe COVID-19, suggesting that IL-19 plays an active role in the inflammatory reaction to an infection.
The pathogenesis of COVID-19 is known to involve IL-19 signaling through IL-20R1 and IL-20R2, which leads to the activation of STAT3. This process has been found to contribute to the viral spread by inhibiting the antiviral interferon response during the early phases of SARS-CoV-2 infection (Dumoutier et al., 2001; Jafarzadeh et al., 2021; Matsuyama et al., 2020; Wruck and Adjaye, 2020) and, additionally, later by causing a cytokine storm (Musiu et al., 2022). We observed that the levels of IL-20 were similar till 120 days and started decreasing till 180 days and were associated with elevated levels of disease severity, which implies that IL-20 might be having a role in the pathogenesis of COVID-19. Recent research has indicated that IL-22 possesses strong abilities to enhance immunity, combat viruses, and fight bacteria. These properties may also be applicable in treating SARS-CoV-2 infection (Das et al., 2020). Another study reported that IL-22+Tc22 and IL-22+Th22 numbers were significantly increased in COVID-19 patients with pneumonia compared with healthy control individuals (Cagan et al., 2022; Fang et al., 2022). We observed that the levels of IL-22 significantly decreased from 120 days till >180 days following infection and were associated with elevated levels of disease severity, which indicates that IL-22 might be having a role in the pathogenesis of COVID-19.
Interleukin (IL)-24 is secreted by different cell types like CD4+ T cells and bronchial epithelial cells and has a role in the pathogenesis of allergic lung (Mitamura et al., 2020). A very recent study described that COVID-19-recovered patients exhibited increased levels of IL-24 compared to healthy controls (Abeer Ghazi Nazzal, 2022). We observed that IL-24 levels significantly decreased from 15–30 days till >180 days following SARS-CoV-2 infection and were associated with elevated levels of disease severity, which indicates that IL-24 might be having a role in the pathogenesis of COVID-19.
Our investigation has certain limitations in that we did not evaluate the practical implication of these modifications in cellular subsets. Furthermore, we did not investigate the evolution of antigen-specific cytokine responses in this study. We have not excluded the other respiratory viral coinfections among the recruited individuals. We were not able to compare the asymptomatic group with the control group due to insufficient sample size in the asymptomatic group. However, our study does encourage further examination of the function of the IL-10 family of cytokines in the acute and convalescent stages of COVID-19. Moreover, our research accentuates the significance and the role of cytokines from the IL-10 family in COVID-19 infection. Our study has the benefit of substantial sample size and illustrates the fluctuations of the IL-10 family of cytokines from the initial stages of infection to >6 months post-COVID-19 disease.
To the best of our knowledge, our study provides the first comprehensive analysis of the levels of the IL-10 family of cytokines in COVID-19 at early time points following infection (from days 15–30) to >180 days. In addition, we compared the levels of the IL-10 family of cytokines between severe and mild COVID-19. These results would help us to understand the dynamics of the IL-10 family of cytokines and their role in pathogenesis. Our finding shows that the levels of the IL-10 family of cytokines slowly revert to normal levels over the period of time as the infection resolves. In addition, our results imply that the elevated levels of IL-10 family of cytokines might be a characteristic feature of COVID-19 and provide a basis for combined therapeutic approaches.
Conclusions
The cytokine family known as IL-10 is a group of cytokines that have not been extensively studied but possess distinct members that exhibit significant biological activities in relation to COVID-19. The IL-10 cytokine family could potentially serve as a common link between various COVID-19 diseases. Due to the intricate nature of this cytokine group, with multiple receptors and pleiotropic properties, gaining a more comprehensive understanding of its complex regulatory functions and individual family members could aid in the development of novel treatment strategies for respiratory viral infections, including COVID-19.
Footnotes
Acknowledgments
The authors are grateful to the Director of the NIRT for ongoing assistance. We appreciate the prompt assistance from the data entry operators Mr. Jaiganesh and Mr. Vigneshwaran, as well as the entire ICER department employees. The authors acknowledge D. Sudha Rani, Scientist B, M. Beula Margarete, Staff Nurse, Technical Officers B.P. Ashok Kumar, C.K. Sathish Kumar, Annamma Jose, D. Augustine, and T. Mahesh, Laboratory Technician, S. Kalaivani, M. Sheeba Mary, C. Kanagasivam, Technical Assistant R. Sivakumar, Project Assistants Y. Radhakrishnaiah, and R. Swapna Shinde.
Authors' Contributions
Designed the study (S.B., A.R, N.P.K.); conducted experiments (A.R., N.P.K., N.S.); acquired data (A.R, N.P.K.); analyzed data (A.R., N.P.K.); contributed reagents (S.B., M.M.); responsible for the enrolment of the participants and also contributed to acquisition and interpretation of clinical data (M.M., J.W.V.T., G.K.C.P.); coordinated field operations (J.W.V.T., M.S.K., T.B., M.P.), coordinated the laboratory processing of samples (G.K.C.P.), coordinated data management (S.R., S.V.); wrote the article (A.R.); revised subsequent drafts of the article (S.B., M.M). All authors read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Division of Intramural Research, the National Institute of Allergy and Infectious Diseases (NIAID), National Institutes of Health (NIH) and ICMR-NIE.