
Abstract
Skin disorders affect ∼40% of the human population. One of the most debilitating cutaneous disorders is Hidradenitis suppurativa (HS), a noncommunicable chronic inflammatory disease with an estimated global prevalence of 0.4% to 2.5%. In January 2011, high levels of IL-17 were discovered in skin lesions of HS patients. In the following years, translational and clinical research led to a better understanding of the pathogenesis of HS. In June 2023, more than 12 years after the initial note, secukinumab, an anti-IL-17A monoclonal antibody, was approved for the treatment of moderate to severe HS. This is the next milestone in improving the treatment of these patients after the approval of the anti-TNF-α monoclonal antibody adalimumab in 2015. In this review article, we present the IL-17 pathway in HS and discuss the use of secukinumab as a therapeutic option for this disease. Our review starts with a description of the epidemiology, clinical features, etiology, and pathogenesis of HS. An overview of the IL-17/IL-17 receptor system in general and a detailed description of the known facts about the expression and action of IL-17 in HS follow. Afterward, we consider the results of clinical trials evaluating the safety and efficacy of IL-17 inhibitors in HS. Finally, a comparison is made between secukinumab and adalimumab and the characteristics of the patients that may be particularly suitable for each of these biologics are described.
Introduction
Skin diseases are among the most common human disorders. A recently published survey of representative 44,689 participants from 27 European countries demonstrated that more than 40% of people aged 18 years or older suffered from at least one dermatological condition or disease in the last 12 months (Richard et al., 2022). Remarkably, the proportion of people with a skin condition seems to increase with age. Nearly 80% of people aged 70 or older are affected (Sinikumpu et al., 2020). The most common skin diseases in the general population are either infections or noncommunicable chronic inflammatory skin diseases (CISDs). The authors of the above-mentioned representative population study in 27 European Union countries calculated the prevalence of the most common CISDs in the population aged 18 and older to be between 0.6% (hidradenitis suppurativa, HS) and 5.5% (atopic dermatitis/eczema) (Richard et al., 2022).
A comparable study with 12,377 patients found the prevalence of the most common CISDs in the population aged 17 to 74 years of 5 European countries (Germany, Italy, the Netherlands, Portugal and Sweden) to be even higher (eg, atopic dermatitis: 7.1%; psoriasis: 4.6%, vitiligo 1.1%) (Svensson et al., 2018). Chronic skin diseases are not only very common; they also significantly reduce the quality of life of those affected (Ujiie et al., 2022). This is often associated with the absence or poor use of effective treatment options.
Notably, the development and persistence of skin alterations in different CISDs appear to be triggered by different immunological mechanisms (Custurone et al., 2021; Diotallevi et al., 2023; Ghoreschi et al., 2021; Sroka-Tomaszewska and Trzeciak, 2021; Trier and Kim, 2023; Wolk et al., 2020; Yanase et al., 2023; Zhou et al., 2022). These mechanisms can be roughly divided into 2 groups, those with dominant involvement of the adaptive immune system and those with dominance of an unspecific inflammation (eg, cryopyrin-associated periodic syndrome, Schnitzler's syndrome). The mechanisms of adaptive immunity involve overactivation of T cells or the humoral immune system (eg, pemphigus vulgaris, bullous pemphigoid, chronic spontaneous urticaria) and are often accompanied by a relative deficiency of regulatory T cells (Treg).
According to the mainly involved effector T cell subpopulation, disorders with an important T cell role may be further subdivided into T1 cell-dominated (eg, vitiligo), T2 cell-dominated (eg, acute atopic dermatitis), T2/T1-dominated (eg, chronic atopic dermatitis), and T17/T22 cell-dominated (eg, psoriasis) responses (Sabat et al., 2019). However, it should be mentioned that professional antigen-presenting cells [eg, macrophages, dendritic cells (DCs), B cells] are necessary for the development of effector T cells, imprinting their phenotype as well as their survival in inflamed tissues (Chatzileontiadou et al., 2020; Loyal et al., 2020; Sabat et al., 2007), making these cells essential players in the pathogenesis of respective diseases.
Furthermore, different immunological mechanisms can coexist and even amplify each other in long-standing lesions. The effector mechanisms of the respective T cell subpopulations, the humoral immune system, or the more unspecific inflammation determine the molecular changes in the local tissue cells, leading to the microscopically and macroscopically specific skin alterations (Eyerich and Eyerich, 2018; Sabat et al., 2019).
For didactic and therapeutic reasons, the classification of CISDs according to their underlying dominant immune mechanism rather than their clinical manifestation or immune response patterns of the skin to immunological processes (eg, lichenoid pattern, fibrogenic pattern, granulomatous pattern) appears to be forward-looking. As more approved drugs targeting the action of certain immune mediators become available and the dominant immune mechanisms are identified in more and more CISDs, the chance that we can eliminate symptoms in more and more CISD patients increases (Eyerich and Eyerich, 2018; Sabat et al., 2019; Yao et al., 2020).
We hope that in the future the treatment decision for patients with CISD will be based on the following: (i) a standardized quantification of the molecules specific to each immunological pathway, (ii) according to the results of this quantification, the identification of the dominant immunological pathway(s) in the patient, and (iii) the consideration of the comorbidities of the patient. The recent approval of the anti-IL-17A antibody secukinumab for the treatment of HS has significantly expanded the treatment options for this disorder.
Hidradenitis Suppurativa
HS is a CISD characterized by the recurrence or persistence of specific skin alterations in usually axillary, inguinal, gluteal, and perianal body sites (Sabat et al., 2020). The HS skin alterations include painful, deep-seated, inflamed nodules, abscesses, and pus-draining tunnels (Sabat et al., 2020). The worldwide prevalence of HS is estimated at 0.4%–2.5% (Anaba et al., 2023; Botvid et al., 2023; Hagan et al., 2022; Prens et al., 2022; Sabat et al., 2020). The first skin changes usually appear in early adulthood and then persist for decades (Sabat et al., 2020; Schneider-Burrus et al., 2021a). HS affects both sexes and is more common in females in some regions of the world such as the United States. While women more frequently suffer from alterations in the inguinal area, the axillary area is more often affected in men (Sabat et al., 2022). Furthermore, skin areas with inflamed nodules are more common in women, and those with fistulas are more often found in men (Sabat et al., 2022).
HS is treated according to its severity. Mild cases can be treated with topical antiseptics and antibiotics (Sabat et al., 2020). For painful abscesses, lancing can be used to ease the acute pain. Moderate and severe HS are treated with systemic antibiotics, surgical resection, or anti-TNF-α antibody adalimumab (Sabat et al., 2020). However, more than 40% of treated patients still complain about pain, discomfort, and/or inflammation/redness (Ingram et al., 2022). This leads to the search for new or additional treatment options for HS (Witte et al., 2022).
HS leads to a profound reduction in the quality of life of those affected (Fabbrocini et al., 2022; Krajewski et al., 2021; Schneider-Burrus et al., 2021b). Pain and discharge of pus in the affected areas and limitations in physical mobility, sex life, choice of clothing, and leisure activities have a profound negative effect on self-image and lead to a withdrawal from social contacts (Andersen et al., 2020; Perche et al., 2022; Sabat et al., 2020; Schneider-Burrus et al., 2018). Importantly, classical HS treatments like abscess lancing, surgical resection, and antibiotic therapy do not appear to improve the quality of life of those affected in the long-term (Schneider-Burrus et al., 2021b; Scholl et al., 2023). Instead, multivariable regression analysis demonstrated that previous surgical interventions in HS patients were associated with anxiety and depression (Scholl et al., 2023).
In addition, HS patients often suffer from systemic concomitant disorders such as metabolic syndrome, cardiovascular morbidity, enthesitis, spondyloarthritis, nonalcoholic fatty liver disease, and inflammatory bowel disease (IBD) (Gau et al., 2022; Hanna et al., 2022; Kridin et al., 2023; Sabat et al., 2020; Sabat et al., 2012; van Straalen et al., 2020). The number of comorbidities that an HS patient suffers from positively correlated with the length of time between the onset of symptoms and the diagnosis of HS (diagnostic delay) (Kokolakis et al., 2020). Due to frequent comorbidities, the life expectancy of patients with HS is reduced by about 15 years on average (Tiri et al., 2019). In addition, HS has an enormous socioeconomic importance due to the significant deterioration in work ability and productivity (Schneider-Burrus et al., 2023).
In Germany, HS causes a loss of annual gross value added of around 13 billion Euros due to presenteeism, sick leave, and increased unemployment rate (Schneider-Burrus et al., 2023). Interestingly, the reduced work ability and productivity of HS patients is primarily linked to depressed mood and pain (Schneider-Burrus et al., 2023).
It is generally accepted that, in addition to genetic predisposition, lifestyle and environmental factors contribute to the development of CISDs (Sabat et al., 2019). As triggers of HS, obesity and smoking are probably the most relevant (van Straalen et al., 2021; Wolk et al., 2020). Due to various molecular mechanisms that have not yet been fully elucidated, these triggers lead to perifollicular infiltration of mononuclear cells and a hyperproliferation of keratinocytes in the infundibulum of the terminal hair follicle (Dunstan et al., 2021; Wolk et al., 2020). This induces stasis in the sebaceous gland/hair follicle/apocrine gland unit, with the propagation of bacteria and the damage of host cells. Components of bacteria and damaged host cells stimulate skin-resident macrophages and dendritic cells via their pattern recognition receptors (Moran et al., 2023; Witte-Handel et al., 2019; Wolk et al., 2020).
These stimulated cells secrete cytokines (eg, TNF-α and IL-1β) and chemokines, which lead to activation of endothelial cells, invasion of other immune cells (in particular monocytes/macrophages and T cells) in the skin lesion, and formation of inflamed nodules (Altman and Criswell, 2021; van Straalen et al., 2022; Witte-Handel et al., 2019; Wolk et al., 2020). Due to an inadequate upregulation of antimicrobial proteins (AMPs), the propagation of bacteria, and the mutual activation of immigrated immune cells, a vicious circle develops and leads to severe inflammation, evident by the strong and broad expression of cytokines (eg, IL-17, IL-26, IFN-γ, IL-10, IL-6) (Wolk et al., 2020; Wolk et al., 2011). The ratio between proinflammatory T cells like Th17 cells to Treg cells trends in favor of Th17 cells (Moran et al., 2017).
More and more immune cells migrate into the lesion, with neutrophils and B cells reaching relevant numbers (Altman and Criswell, 2021; Gudjonsson et al., 2020; Sabat et al., 2023). Neutrophils are causally responsible for clinically important abscesses and purulence. Matrix metalloproteinases released by neutrophils and activated fibroblasts lead to remodeling and destruction of the physiological skin appearance with tunnel and scar formation (Tsaousi et al., 2016; Witte-Handel et al., 2019; Wolk et al., 2021). Moreover, structures reminiscent of lymph nodes (tertiary lymphatic structures) appear in the HS skin lesions (Sabat et al., 2023). In the tertiary lymphatic structures, plasma cells can develop, which produce antibodies (partly autoantibodies) that in turn can increase local inflammation and systemically trigger or support the occurrence of concomitant diseases (Carmona-Rivera et al., 2022; Macchiarella et al., 2023; Mulani et al., 2018; Oliveira et al., 2023; Theut Riis et al., 2017).
Besides autoantibodies, the systemically elevated cytokines, adipokines, as well as matrix metalloproteases, the relative deficiency of Treg in the blood, and blood memory T cells able to infiltrate further organs may all play a role in the development of systemic comorbidities in HS patients (Hessam et al., 2020; Krajewski et al., 2023; Tsaousi et al., 2016; Witte et al., 2023; Wolk and Sabat, 2016; Wolk et al., 2017).
The recently published results from a phase 3 clinical trial with the anti-IL-17A monoclonal antibody secukinumab show that IL-17A plays a vital role in HS pathogenesis (Kimball et al., 2023a).
Biology of Interleukin-17A and Interleukin-17F
IL-17A and IL-17F are the 2 most extensively studied cytokines of the IL-17 family (which comprises 6 members, named IL-17A, B, C, D, E (IL-25), and F) (Fig. 1) (McGeachy et al., 2019). IL-17A, originally called CTLA-8, was cloned from activated T cells and first described in June 1993 and was found to be largely homologous to the open reading frame of the T cell-tropic gamma herpesvirus Herpesvirus saimiri (Rouvier et al., 1993). IL-17F was discovered a few years later, in 2001, by genome sequencing (Starnes et al., 2001). IL-17A and IL-17F function as disulfide-linked homodimers (IL-17A/A and IL-17F/F) or heterodimers (IL-17A/F). They exhibit ∼50% sequence homology to each other and similar three-dimensional structures, enabling them to signal via common receptors (Brembilla et al., 2018).
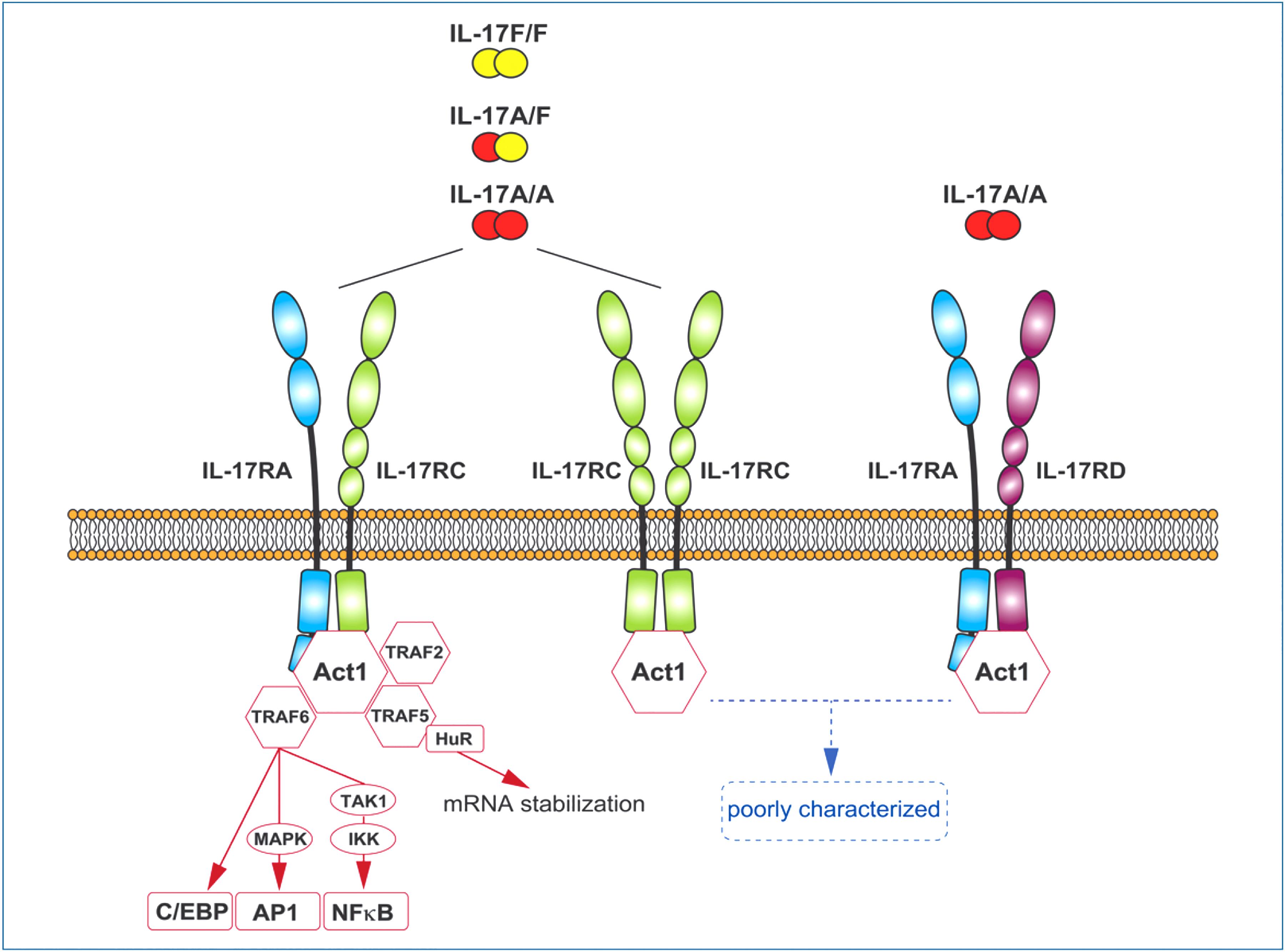
Schematic representation of IL-17A and IL-17F cytokines, their receptors and the main signaling pathways involved.
The best-characterized receptor, used by IL-17A/A, IL-17A/F, and IL-17F/F, is composed of the heterodimeric combination of IL-17RA and IL-17RC subunits (the latter are members of the broader IL-17 receptor family covered 5 structurally related receptor subunits, IL-17RA to IL-17RE). However, a recent data had shown that all 3 cytokines can also bind to a receptor composed of 2 IL-17RC subunits and transduce signals independently of IL-17RA (Goepfert et al., 2020). It should be noted that IL-17RA and IL-17RC exhibit different selectivity toward IL-17A and IL-17F, with IL-17RC binding equally well IL-17A and IL-17F, while IL-17RA has a much weaker affinity for IL-17F (Ho and Gaffen, 2010; Kuestner et al., 2007). Finally, the IL-17RA/RD heterodimer has been identified as an alternative functional receptor for IL-17A/A, but not for IL-17A/F nor IL-17F/F (Su et al., 2019).
IL-17RA and IL-17RC contain a cytoplasmic SEFIR domain, which leads to the recruitment of the Act1 adaptor protein via homotypic domain interaction (Gaffen, 2009). It is this feature that makes the IL-17 signaling pathway unique. Act1 acts as a docking station for TRAF proteins: recruitment of TRAF6 facilitates target gene transcription via activation of the NFκB, MAPK/AP1, and C/EBP pathways; recruitment of TRAF2/5 leads to downstream activation of RNA-binding proteins (such as HuR and Regenase-1), which control post-transcriptional events and regulate mRNA stability.
In addition to its role as an adaptor protein, Act1 also exhibits direct mRNA-binding activity, which appears to underlie the IL-17 receptor-mediated target specificity (Swaidani et al., 2019). Recent crystallographic analysis revealed the formation of a 2:2:2 hexameric signalosome composed of 2 units of IL-17A/A, IL-17RA, and IL-17RC (Goepfert et al., 2022). At least in vitro, IL-17RA dimerization has been shown to be functionally relevant in potentiating target gene expression (Goepfert et al., 2022).
IL-17A and IL-17F are secreted by immune cells and act primarily on epithelial and mesenchymal cells of barrier tissues such as skin and mucosa, playing a crucial role in protective immune responses against extracellular pathogens and fungi (Sabat et al., 2019). Th17 cells have been described as the main producer of IL-17 (both IL-17A and IL-17F), in a mechanism dependent on TCR signaling and IL-1β/IL-23/IL-6 cytokines (Sabat et al., 2019). IL-17F is believed to be generally coexpressed with IL-17A in these cells, the 2 genes being located at the same locus. However, this concept is challenged by recent data from single-cell analysis of emigrating cells from psoriasis lesional samples, showing that less than 10% of cells coexpress the 2 cytokines (Kim et al., 2021). At least in lesional psoriatic skin, single IL-17F producers appear to outweigh single IL-17A producers (Kim et al., 2021).
To date, it is well established that there are many other cellular sources of IL-17A and IL-17F, including γδ T cells, type 3 innate lymphoid cells (ILC3), NK and NKT cells, MAILTs, neutrophils, and mast cells. Contrary to what was initially thought, many of these cells can produce IL-17 independently of IL-23 (Brembilla et al., 2017; Cole et al., 2020; Lee et al., 2015).
IL-17A and IL-17F induce overlapping effects in target cells, with IL-17A/A considered more potent than IL-17A/F and IL-17F/F (Brembilla and Boehncke, 2023). Under physiological conditions, IL-17A and IL-17F trigger protective responses in bordering tissues by inducing target cells to produce several chemokines (notably CCL20, CXCL1, CXCL8) and cytokines [notably IL-19, IL-20, granulocyte-macrophage colony-stimulating factor (GM-CSF), G-CSF, IL-17C, IL-36 isoforms], resulting in the recruitment of neutrophils and the amplification of a polarized Th17 immune response (Albanesi et al., 2000; Homey et al., 2000; Witte et al., 2014; Wolk et al., 2023; Wolk et al., 2009;Yao et al., 1995). In addition to their proinflammatory effects, IL-17A and IL-17F participate in direct host defense against microbial infections by inducing antimicrobial peptides (AMPs, such as defensins, S100A proteins, and cathelicidins), and participate in tissue remodeling by promoting the release of metalloproteinases (Brembilla and Boehncke, 2023; Brembilla et al., 2018).
Interestingly, besides having an important role in psoriasis pathogenesis, IL-17A does not directly increase proliferation of keratinocytes and only slightly modulates their terminal differentiation (Borowczyk et al., 2020; Wolk et al., 2009). Although the target cells of IL-17A and IL-17F are mainly of nonhematopoietic origin, these cytokines have also been shown to directly affect immune cells and alter regulatory T cell responses (Crawford et al., 2020).
While they exert important physiological functions, IL-17A and IL-17F's notoriety today is mainly linked to their relationship with various inflammatory and autoimmune disorders. Conditions such as psoriasis, psoriatic arthritis, HS, ankylosing spondylitis, rheumatoid arthritis, IBD, multiple sclerosis, and asthma display elevated levels of IL-17A and IL-17F. Recognizing their pathophysiological importance in some of these disorders, therapeutic strategies aimed at blocking their activity have recently been developed and monoclonal antibodies that specifically target IL-17A, IL-17A, and IL-17F or IL-17RA have been approved by regulatory authorities for the treatment of certain conditions, such as psoriasis (Ghoreschi et al., 2021).
Interleukin-17 in HS
The first description that IL-17A is upregulated in cutaneous HS lesions compared to skin from healthy donors dates back to January 2011 (Wolk et al., 2011), notably, more than 12 years before the anti-IL-17A antibody secukinumab was approved for the treatment of the disease. Importantly, the authors showed already then that IL-17A in HS lesions reaches levels comparable to those seen in skin lesions of patients with psoriasis vulgaris (Wolk et al., 2011), a CISD that can be treated very well with IL-17 and IL-17 receptor-targeting antibodies (Ghoreschi et al., 2021). The identified increased presence of IL-17A in HS lesions was subsequently confirmed by other groups (van der Zee et al., 2012; Kelly et al., 2015).
Furthermore, some elevation of IL-17A expression was found in perilesional skin of HS patients (Kelly et al., 2015). The elevation of IL-17F in cutaneous HS lesions was only demonstrated in 2019 (Witte-Handel et al., 2019). As with IL-17A, the levels of IL-17F tended to be higher in HS lesions than in psoriatic lesions (Witte-Handel et al., 2019).
CD4+ cells, found in papillary and reticular dermis of HS lesions, were shown to be able to secrete IL-17 (Hotz et al., 2016; Schlapbach et al., 2011). Almost all of the IL-17A-producing CD4+ cells were also able to produce TNF-α, with many coproducing further cytokines such as IFN-γ, IL-22, and/or GM-CSF (Moran et al., 2017). Interestingly, the relative proportion of such multifunctional T-helper cells was even higher in perilesional compared to lesional HS skin (Moran et al., 2017). Comparing single-cell RNA sequencing data obtained from HS skin tunnels and psoriatic lesions, with the focus on T17 cells (CD161+ CD3+ cells expressing IL-17A and/or IL-17F), a recent study stated a higher mean IL-17F expression and a high proportion of IL-17F-expressing T17 cells (most of them not coexpressing IL-17A) in HS (Kim et al., 2023). However, the authors further demonstrated less coexpression of IL-26, IL-22, and IFN-γ by HS compared to psoriatic T17 cells (with IL-26 and IFN-γ expression mainly assigned to the underrepresented IL-17A+ subset). While psoriatic lesions also contain a considerable proportion of CD8+ T cells able to produce IL-17A, it has been reported that HS lesions do not (Lowe et al., 2020). So far, there is no reliable information about the role of innate IL-17 sources such as innate lymphoid cells in HS lesions.
The production of IL-17 by Th17 cells is known to be supported by the cytokines IL-23, IL-1β, and IL-6 (Ghoreschi et al., 2021), which are all upregulated in HS lesions (Wolk et al., 2011; Schlapbach et al., 2011; Witte-Handel et al., 2019). IL-23, with its essential subunit p19, is expressed by macrophages in the lesional HS skin (Schlapbach et al., 2011), and is well established as the key T17-supporting cytokine in psoriasis (Ghoreschi et al., 2021). Recent clinical trials with risankizumab und guselkumab, however, did not support a crucial role of IL-23 in HS pathogenesis (Kimball et al., 2023b; Kimball et al., 2023c). Instead, a major role of IL-1β in triggering the IL-17 production in HS lesions might be postulated. In line with that, T17 cells in HS skin lesions express limited levels of IL-23 receptor transcripts while showing high levels of IL-1R1 when compared to T17 cells in psoriatic lesions (Kim et al., 2023). Moreover, an inflammasome inhibitor decreased IL-17A levels in parallel with IL-1β levels in HS skin explant cultures (Moran et al., 2023). Finally, IL-1β was able to induce IL-17 production in explant cultures from healthy donor submammary skin (Vossen et al., 2020).
It should be noted that the expression of IL-1β (but not IL-1α) and its target molecules in HS lesions is much higher than in psoriatic lesions and is mainly derived from macrophages/dendritic cells (Kelly et al., 2015; van der Zee et al., 2012; Witte-Handel et al., 2019; Wolk et al., 2011). Importantly, the IL-1β upregulation in HS lesions is not paralleled by an increase in IL-1 receptor antagonist expression as seen in psoriatic lesions (Witte-Handel et al., 2019). Furthermore, RNA sequencing data suggested decreased transcript counts of IL-1 receptor-2, a decoy receptor chain, in nonlesional HS skin compared to healthy donor control skin (Lowe et al., 2020). These data imply both abundancy and unlimited action of IL-1β in HS skin. The concept of IL-1β being a main supporter of lesional IL-17 production in HS also matches the results of a small randomized clinical trial with the IL-1 receptor antagonist anakinra that delivered promising results (Tzanetakou et al., 2016). Further, more detailed investigations are, however, needed to explore the relative contribution of IL-23 versus IL-1β in supporting T17 cell phenotype and function in HS skin lesions.
In the skin, keratinocytes are known to be the main target cells of IL-17, although effects have also been detected on, for example, fibroblasts and endothelial cells (Ghoreschi et al., 2021) (Fig. 2). In the context of HS pathogenesis, the following effects of IL-17 on keratinocytes have been suggested: (i) induction of neutrophil-attracting chemokines such as CXCL1, CXCL6, and CXCL8 (thereby contributing to the clinical symptom of abscesses and pus-secreting skin tunnels) (Witte-Handel et al., 2019), (ii) induction of G-CSF (thereby increasing the viability and activity of these cells and contributing to tissue destruction) (Wolk et al., 2021), (iii) induction of matrix metalloproteases (thereby facilitating the infiltration of immune cells into the skin and long-term tissue destruction) (Witte-Handel et al., 2019), and (iv) induction of LCN2 (thereby contributing to metabolic alterations and inflammatory pain) (Wolk et al., 2017) (Fig. 2).
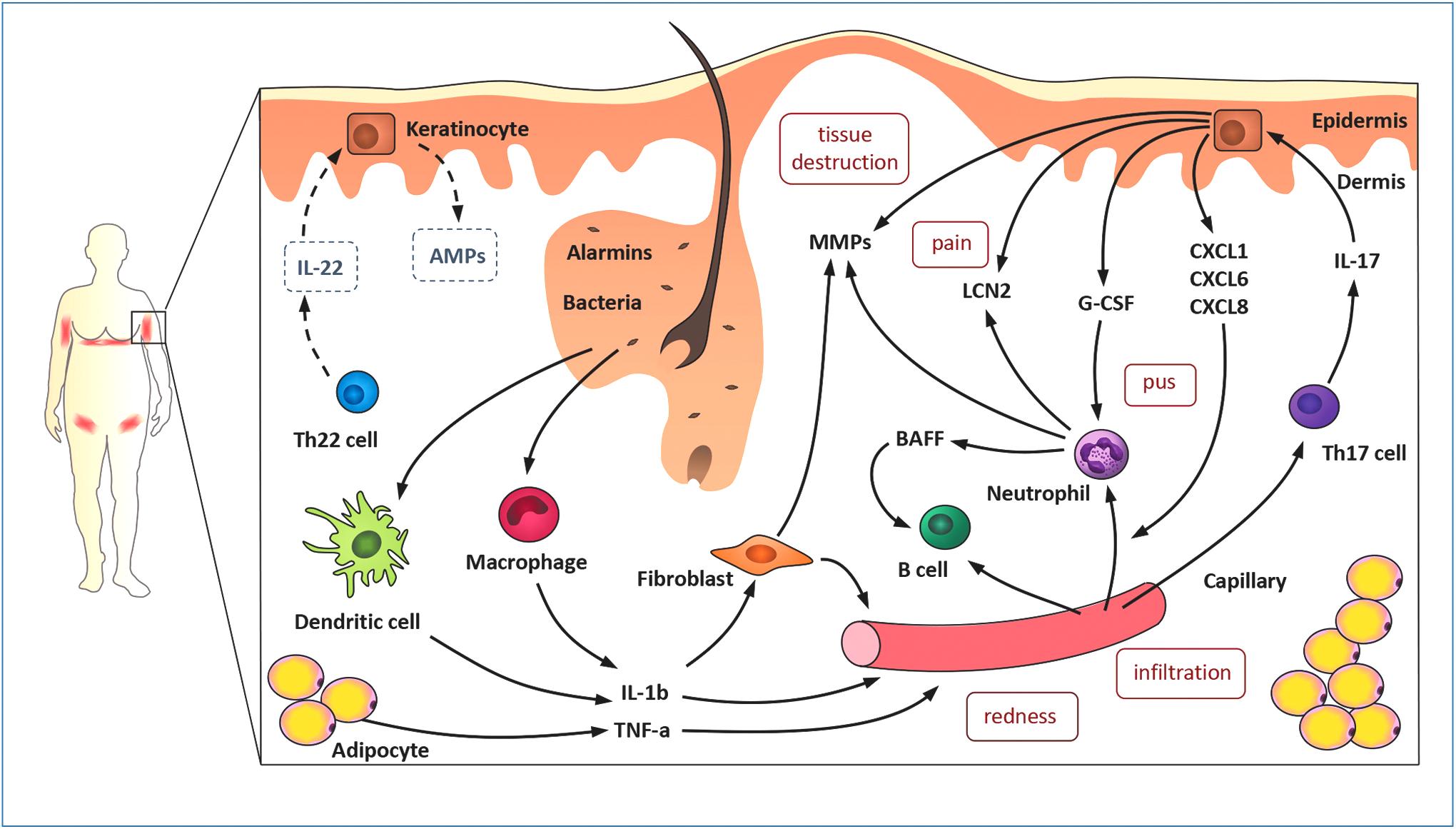
Pathogenesis of HS. HS, Hidradenitis suppurativa.
It is noteworthy that IL-17 does not induce these effects in fibroblasts (Witte-Handel et al., 2019; Wolk et al., 2021; Wolk et al., 2017). While on their own, the effects of IL-17 are moderate, these cytokines synergize with the TNF-α (Witte-Handel et al., 2019; Wolk et al., 2021; Wolk et al., 2017). In contrast to TNF-a, the synergisms between IL-17 and IL-1β are poor (Witte-Handel et al., 2019; Wolk et al., 2021; Wolk et al., 2017). Furthermore, IL-17, especially in the presence of the Th22 cell cytokine IL-22, triggers the expression of epidermal AMPs (such as β-defensin-2 and S100A7) (Liang et al., 2006; Wolk et al., 2011). However, since the expression of the potent AMP-inducer IL-22 (Wolk et al., 2004) is low in HS lesions, the AMP upregulation is nevertheless limited compared to psoriatic lesions and may account for the bacterial propagation in HS skin (Wolk et al., 2011) (Fig. 2).
Interleukin-17-Targeting Drugs as Novel Therapy Options for HS
Based on the evidences of a major role of IL-17 in the pathogenesis of HS, several biologics targeting the IL-17 system have been assessed in moderate to severe HS. Among them, secukinumab was approved very recently (June 2023), and further IL-17 inhibitors (eg, bimekizumab, brodalumab) are well on the way of getting approval (Glatt et al., 2021; Kimball et al., 2023a).
Secukinumab
The highest level of evidence for any anti-IL-17 treatment in HS comes from 2 phase III trials; the SUNSHINE (NCT03713619) and the SUNRISE (NCT03713632), assessing the effectivity of secukinumab, a human monoclonal antibody that selectively binds IL-17A (Kimball et al., 2023a). In both trials, patients with moderate to severe HS (≥5 inflammatory lesion counts, ie, abscesses and/or inflammatory nodules in ≥2 distinct anatomic areas) were randomly assigned (1:1:1) to receive secukinumab 300 mg every 2 weeks (SQ2W; SUNSHINE n = 181, SUNRISE n = 180), secukinumab 300 mg every 4 weeks (SQ4W; SUNSHINE n = 180, SUNRISE n = 180), or placebo (SUNSHINE n = 180, SUNRISE n = 183) for an initial 16 weeks and 36 week maintenance period (Kimball et al., 2023a). After 16 weeks, placebo-treated patients were switched to SQ2W or SQ4W.
Importantly, significantly more patients in the initial SQ2W groups achieved Hidradenitis Suppurativa Clinical Response (HiSCR) compared with placebo at week 16; respectively, 45% versus 34% (P < 0.01, SUNSHINE) and 42% versus 31% (P < 0.05, SUNRISE, Table 1) (Kimball et al., 2023a). HiSCR is defined as a ≥ 50% reduction in inflammatory lesion count (sum of abscesses and inflammatory nodules) and no increase in abscesses or draining fistulas (Kimball et al., 2014). The SQ4W group only showed a significantly higher HiSCR rate than placebo in the SUNRISE trial; 46% versus 31%, P < 0.01 (Kimball et al., 2023a).
Data from Phase III Studies of Approved Anti-TNF and Anti-IL-17 Biologics
Pooled analysis over the trials showed a significant reduction in the percentage of inflammatory nodules (−46.8% vs. −24.3%, P < 0.0001) and abscesses (39.3% vs. −22.4%, P < 0.01) but not in draining tunnel count (−1.4 vs. −0.6) in the SQ2W group versus placebo at week 16 (Poster_EHSF_2023_P144 and Kimball et al., 2023a). Patients (SQ2W) with no previous biologic treatment had similar odds of achieving HiSCR over the placebo group at week 16 (OR 1.64 [95% CI: 1.15–2.33]) as the patients with prior exposure to systemic biologic therapy (OR 1.60 [95% CI: 0.83–3.08]) (Poster_AAD_2023_P42652). Regarding of concomitant antibiotic use, patients (SQ2W) with concomitant antibiotic use showed significantly increased odds of achieving HiSCR over the placebo group at week 16 (OR 4.78 [95% CI: 1.64–13.5]) than patients without concomitant antibiotic use (OR 1.45 [95% CI: 1.05–2.01]) (Poster_AAD_2023_P42981).
Of the SQ2W patients who achieved HiSCR at week 16, 75.9% (SUNSHINE) and 83.6% (SUNRISE) maintained clinical response at week 52 (Poster_AAD 2023_P42640). Overall, 49% (SUNSHINE) and 55% (SUNRISE) of HiSCR nonresponders at week 16 achieved HiSCR at week 52 (Poster_AAD_2023_P42640).
Pooled analysis of pain scores revealed that SQ2W-treated patients had greater odds of achieving skin pain Numeric Rating Scale 30 (NRS30; ≥ 30% and ≥2-point reduction from baseline skin pain NRS in patients with a baselines score ≥3) compared with placebo-treated patient at week 16 (OR 1.8 [95% CI: 1.2–2.7], P < 0.01). In both trials, the SQ2W group demonstrated higher Dermatology Life Quality Index (DLQI) response rates (a ≥ 5-points decrease from baseline) than the placebo groups, respectively, 48% versus 37% (SUNSHINE) and 38% versus 32% (SUNRISE), which was maintained at 52 weeks. The DLQI is a 10-item questionnaire used to quantify the negative impact of skin disease on the quality of life of an affected person.
Fungal infections (mainly Tinea and Candida) were reported by 8%–15% of the initial SQ2W and SQ4W patients during the 52 weeks (Kimball et al., 2023a). All fungal infections were localized, mild to moderate infections, which resolved upon treatment and did not lead to study discontinuation. Three new-onset IBD cases were reported in the SUNRISE trial (Kimball et al., 2023a). Following these successful trials, secukinumab was approved by the European Medicines Agency (EMA) in June 2023 for the treatment of HS (
Bimekizumab
Bimekizumab (a humanized monoclonal antibody binding both IL-17A and IL-17F) has been assessed in a phase II, placebo-controlled clinical trial (Glatt et al., 2021). Patients were randomized (2:1:1) to receive bimekizumab (320 mg BQ2W, n = 46), placebo (n = 22), or adalimumab (40 mg weekly, n = 22) for 12 weeks (Glatt et al., 2021). In the BQ2W group, significantly more patients achieved HiSCR (57%, nonresponder imputation [NRI]) than in the placebo group (24%), demonstrating superiority of bimekizumab over placebo (OR 3.95, [95% CI: 1.22–12.79]). HiSCR75 and HiSCR90 were achieved by 46% and 32% of BQ2W-treated patients and 10% and 0% of placebo-treated patients (NRI), respectively. Overall, 35% of BQ2W patients achieved excellent DLQI response (a score of 0/1) compared with 0% of placebo patients at week 12.
In contrast to the placebo group (0%), 64% of the B2QW group achieved a ≥ 30% and ≥1-point reduction in skin pain Visual Analog Scale (VAS) (Glatt et al., 2021). Four cases of oral candidiasis occurred among 3 bimekizumab-treated patients and no instances of new-onset IBD were recorded (Glatt et al., 2021).
Two subsequent phase III studies (BE HEARD I [NCT04242446], n = 505, and BE HEARD II [NCT04242498], n = 509) have been completed but have not been published. These studies compared 2 dosing regimens of bimekizumab (320 mg BQ2W and 320 mg every 4 weeks; BQ4W) with placebo over a 16-week initial and 32-week maintenance period. Preliminary pooled analysis showed that a significantly higher proportion of the BQ2W and BQ4W groups achieved HiSCR at week 16, compared with placebo in both studies: BQ2W 47.8% versus 28.7% (P = < 0.01) and 52.0% versus 32.2% (P < 0.01), and BQ4W 45.3% versus 28.7% (P < 0.05) and 53.8% versus 32.2% (P < 0.01) in, respectively, the BE HEARD I and II (
Other IL-17-targeting biologics
Izokibep, a small (18.6 kDa) protein inhibitor of IL-17A has been assessed in an open-label, randomized phase IIb trial. Izokibep consists of 3 triple helical affinity domains (2 IL-17A-binding domains and one albumin-binding domain) (Klint et al., 2023). Result summary from a clinical trial with 30 HS patients treated with izokibep 160 mg weekly (NCT05355805) is available as an announcement from the company (
Preliminary results from a phase IIa study with sonelokimab, an anti-IL-17 A/F nanobody, have recently been announced (NCT05322473). Sonelokimab (120 mg) showed superiority over placebo for HiSCR75 (primary endpoint), with a 29 percentage points (ppt) delta versus placebo (P = 0.0002) at week 12, and for HiSCR50, with a 38 ppt delta versus placebo (P < 0.0001).
Other IL-17 pathway-targeting biologics such as brodalumab (a human monoclonal antibody blocking IL17RA), ixekizumab (a humanized monoclonal antibody blocking IL-17A) have only been assessed in small cohort studies and case series (Esme et al., 2022; Frew et al., 2021; Frew et al., 2020). In 2 open-label cohort studies (both involving 10 patients) with either biweekly or weekly dosing of 210 mg brodalumab, 100% of patients achieved HiSCR accompanied by significant decreases in VAS Pain and DLQI scores at week 12 (Frew et al., 2021; Frew et al., 2020). However, in a real-world setting among adalimumab refractory patients, clinical response fell short of the 2 open-label trials (Kearney et al., 2023). A case series of ixekizumab (80 mg biweekly) demonstrated that 4/5 treated patients achieved HiSCR, VAS pain reduction and DLQI improvement after 12 weeks (Esme et al., 2022).
With secukinumab already approved for use in Europe and several other ongoing/completed phase III studies, these promising anti-IL-17 therapies should soon reach patients.
Comparison of Secukinumab with Adalimumab in HS
Adalimumab, an anti-TNF-α antibody, was the first biologic to show therapeutic efficacy in HS prospective, randomized, double-blinded, placebo-controlled, clinical trials (Kimball et al., 2012; Miller et al., 2011). In a phase II, placebo-controlled, randomized trial of 154 patients with moderate to severe disease, ∼55% of patients treated weekly with adalimumab reached HiSCR at week 16 compared to 26% in the placebo group (Kimball et al., 2016b). In 2 phase III clinical trials (PIONEER I n = 307 and PIONEER II n = 326) assessing the effectivity of adalimumab in HS, patients were randomly assigned (1:1) to receive adalimumab 40 mg weekly or placebo for 12 weeks (Kimball et al., 2016a).
A significantly higher proportion of patients in the adalimumab group compared to the placebo group reached the HiSCR: 41.8% versus 26.0% in PIONEER I (P = 0.003) and 58.9% versus 27.6% in PIONEER II (P < 0.001) (Kimball et al., 2016a) (Table 1). Serious adverse events occurred in 1.3% of patients receiving adalimumab and 1.3% of those receiving placebo in PIONEER I and in 1.8% and 3.7% of patients, respectively, in PIONEER II (Kimball et al., 2016a).
Our current understanding of the role of TNF-α (Wolk et al., 2020) and IL-17 (see chapter ‘Interleukin-17 in HS’) in HS pathogenesis suggests that both cytokines have partially distinct functions, although they might strongly enhance each other's HS-related effects in keratinocytes. However, we do not yet have biomarkers that can be quantified in skin or blood to indicate whether the TNF-α or the IL-17 pathway dominates in a given patient. There are only preliminary data indicating that lesions with a strengthened inflammatory molecular signature, particularly those associated with immune cell recruitment and B cell signature, are less likely to linearly respond to adalimumab (Lowe et al., 2020).
It is our lack of knowledge that prevents us from developing routine tests to select the patients who should receive secukinumab instead of adalimumab. At the moment, a recommendation can only be based on the experiences from other indications, in which both antibodies are already approved, that is, from psoriasis. In doing so, IL-17 inhibitors should be the first choice in patients with risk for Mycobacterium tuberculosis infection, demyelinating disease, or lupus. Patients with cardiovascular comorbidities, spondyloarthritis, or psoriatic arthritis might also benefit from IL-17 inhibition (Fig. 3). TNF inhibitors are recommended for HS patients with concomitant IBD and rheumatoid arthritis. Patients with child-bearing intentions, spondyloarthritis, or psoriatic arthritis might also benefit from particular TNF inhibitors (Fig. 3).

Algorithm for treating HS with distinct biologics. *A classification into mild, moderate, and severe HS can also be made according to the International Hidradenitis Suppurativa Severity Score System (IHS4) (Zouboulis et al., 2017).
Conclusions
The recent approval of secukinumab for the therapy of HS sets a clear expectation for the treatment options for these patients. However, further efforts are needed to permanently improve the care of HS patients. The authors consider the following aspects to be particularly relevant and in need of improvement: The time between the onset of symptoms and HS diagnosis must definitely be reduced. In Germany, for example, this time is 10 years (Kokolakis et al., 2020). Delayed diagnosis is associated not only with a higher number of physicians consulted, resulting in higher health care costs, but also with more severe HS disease and a higher number of concomitant disorders at the time of diagnosis (Kokolakis et al., 2020). Early systemic immunomodulating therapy is indicated to prevent irreversible destruction of the skin architecture in the affected body regions (Sabat et al., 2020). Therefore, future studies should aim to determine the best time to start therapy with secukinumab or adalimumab (definition of the window of opportunity). HS is a disease with a strong systemic component (Sabat et al., 2020). Exploring the potential impact of secukinumab and adalimumab treatment on HS inflammatory comorbidities would increase acceptance for early and widespread use of these drugs. Moreover, we need to identify parameters (preferably clearly quantifiable biomarkers) that make it possible to determine patients who will benefit most from the available treatment options (eg, anti-TNF-α vs. anti-IL-17). Numerous clinical trials are ongoing that address the role of cytokines and inflammatory pathways other than TNF-α and IL-17 in HS pathogenesis (Gamell et al., 2023; Liu et al., 2023; Molinelli et al., 2023; Tsai et al., 2023). As long as the treatment responses remain highly heterogenic, it is highly desirable that appropriate programs to identify and validate therapy response-predicting biomarkers should be integrated into clinical development programs and be specified at the time of approval.
Footnotes
Acknowledgment
The authors acknowledge Anna-Sophia Wolk for her support with the illustrations.
Author Disclosure Statement
R.S. has received research grants, scientific awards, or honoraria for participation in advisory boards, clinical trials, or as speaker for one or more of the following: AbbVie, Inc., AbbVie Deutschland GmbH & Co. KG, Almirall Hermal GmbH, Amgen GmbH, Bayer Schering Pharma AG, Boehringer Ingelheim Pharma GmbH & Co. KG, Celgene GmbH, Celgene International II Sàrl, Charité Research Organisation GmbH, CSL Behring, Dr. Willmar Schwabe GmbH & Co. KG, Flexopharm GmbH & Co. KG, ICON plc, Incyte Corporation, Janssen-Cilag GmbH, La Roche-Posay Laboratoire Dermatologique, MoonLake Immunotherapeutics AG, Novartis Pharma GmbH, Parexel International GmbH, Rheinischen Friedrich-Wilhelms-Universität Bonn, Sanofi–Aventis Deutschland GmbH, TFS GmbH, and UCB Biopharma SPRL.
JG has received research grants, or honorary for participating in advisory boards for one or more of the following: AbbVie, Novartis, UCB, Almirall, Eli Lilly, Janssen, Kyowa Kirin, Boehringer Ingelheim, Sanofi. KRvS has received honoraria for participation in advisory boards or as speaker for Novartis Pharma GmbH, UCB Biopharma SPRL, and Boehringer Ingelheim Pharma GmbH & Co. KG. KW has received research grants, travel grants, consulting honoraria or lecturer's honoraria from AbbVie Inc., AbbVie Deutschland GmbH & Co., Celgene/BMS, Charité Research Organisation GmbH, Dr. Willmar Schwabe GmbH & Co. KG, Flexopharm GmbH & Co. KG, JanssenCilag GmbH, Novartis Pharma GmbH, Pfizer Deutschland GmbH, Sanofi–Aventis Deutschland GmbH, TFS GmbH, and UCB Biopharma SPRL.
Funding Information
The preparation of this review was neither funded nor financially supported.