
Abstract
We aimed to examine the relationship between serum midkine levels and placental invasion in pregnant women with placenta previa. The study group consisted of 43 pregnant women diagnosed with placenta previa, whereas the control group consisted of 60 healthy pregnant women. Serum midkine levels were compared between pregnant women with placenta previa and the control group in this study's first part. Thereafter, the utility of midkine in the prediction of the abnormally invasive placenta (AIP) was investigated and optimal cutoff values were calculated. Significantly higher serum midkine level was observed in placenta previa cases than in the controls (1.16 ng/mL vs. 0.18 ng/mL, P < 0.001). Serum midkine level was also significantly higher in the AIP group among the placenta previa cases (P = 0.004). In the receiver operating characteristic analysis, the cutoff value of the midkine level in predicting AIP was 1.19 ng/mL. This study revealed that the serum midkine level is higher in pregnant women with AIP. Maternal serum midkine level may be used as a complementary biomarker to the radiological and clinical findings for the prediction of the AIP in placenta previa cases.
Introduction
Placenta previa, abnormal implantation of placental tissue that covers the endocervical os or ends at a distance of ≤2 cm, is one of the most challenging complications that cause maternal and fetal–neonatal morbidity and mortality (King et al., 2020). Women diagnosed with placenta previa are at high risk of postpartum hemorrhage (PPH), which is the leading cause of maternal morbidity and mortality across the world (Fan et al., 2017).
Therefore, patients with placenta previa have been reported to have a higher requirement of blood transfusion and cesarean hysterectomy (Lal and Hibbard, 2015). Although the exact cause of placenta previa remains unknown, it is considered to be an inflammatory process associated with the abnormal vascularization of the endometrium caused by atrophy or scarring from previous trauma, surgery, or infection (Li et al., 2018).
Placenta previa patients are at high risk for placenta accreta spectrum (PAS), a term used to refer to varying degrees of placental adhesion and invasion. This spectrum includes placenta accreta (adhesion of the placenta to the myometrium), placenta increta (invasion of the myometrium), and placenta percreta (invasion of the myometrium, serosa, and adjacent organs). The main risk factor of PAS is previous cesarean delivery. In women with placenta previa, the risk of placental invasion may increase from 3% to 67% as the number of cesarean sections increases (Silver and Branch, 2018; Silver et al., 2006).
Placenta increta and percreta are called abnormally invasive placenta (AIP) due to placental invasion. As placenta increta and percreta are associated with higher rates of maternal mortality and morbidity, accurate prenatal diagnosis of these mentioned types of AIP is critical (Jauniaux et al., 2021). Owing to the risk of severe bleeding in AIP, the most generally accepted approach is to perform a cesarean hysterectomy after the delivery of the fetus.
Therefore, antenatal diagnosis results in better outcomes and allows referring the patient to a multidisciplinary center before delivery (Cahill et al., 2018). Although the diagnosis of AIP is made at delivery, ultrasonography, magnetic resonance imaging, and some biomarkers have been investigated to be used for antenatal suspicion (Kawashima et al., 2014).
The pathophysiology of AIP is based on abnormal decidualization and postoperative scarring (Jauniaux et al., 2022). Recent studies have associated placental findings such as uteroplacental vascular abnormalities, infarction, and acute and chronic inflammation with etiopathogenesis (Ernst et al., 2017). A better understanding of the molecular basis of placental disorders suggests that inflammation and placental invasion may be closely related (Bartels et al., 2018).
Midkine is a cytokine/growth factor involved in cell recruitment, migration, and chemokine expression in the inflammatory process (Yazihan, 2013). Midkine was also found to modulate the expression of proinflammatory cytokines and the expansion of regulatory T cells (Weckbach et al., 2011). Midkine was first described at the early differentiation stage in embryonal life (Böhlen and Kovesdi, 1991). In addition, midkine expression levels were demonstrated in the extraembryonic membranes and placenta during early pregnancy in the mouse model, and expression was decreased during embryogenesis (Obama et al., 1995).
Although previous studies have suggested that the expression of midkine in adult organisms is limited to a few tissues/organs, it is now known that most organ systems and cell types have the capacity to secrete midkine under normal conditions (Yazihan, 2013). Therefore, midkine has been shown to play a role in a variety of diseases, including cardiovascular, autoimmune, inflammatory diseases, and cancer (Cai et al., 2020). Midkine also has mitogenic, antiapoptotic, migratory, chemotactic, angiogenic, and fibrinolytic functions (Kadomatsu and Muramatsu, 2004; Zhang and Deuel, 1999).
In this study, we aimed to compare the maternal serum midkine levels of pregnant women with placenta previa and those with uneventful pregnancies. We also evaluated the predictive ability of maternal serum midkine level to detect pregnant women with AIP in women with placenta previa.
Materials and Methods
This prospective case–control study was conducted at the perinatology unit of Ankara City Hospital from June 15, 2021, to June 15, 2022. Written informed consent was obtained from all participants. The study was carried out in accordance with the tenets of the Declaration of Helsinki after receiving approval from the medical research ethics committee of the Ankara City Hospital (E2-21-592).
Study population
The study consisted of 103 participants, of whom 43 were pregnant women with a diagnosis of placenta previa and 60 were healthy women with singleton pregnancies. PAS assessments of all patients were performed and confirmed intraoperatively according to the clinical staging specified in the guidelines published by the International Federation of Gynecology and Obstetrics (FIGO). According to FIGO, PAS classification, Grade 1 was defined as abnormally adherent placenta (placenta accreta), and Grades 2 and 3 as AIP (placenta increta and percreta) (Jauniaux et al., 2019b). According to the invasion status, 14 of the 43 cases had placenta increta and percreta. The remaining 29 cases had placenta accreta or isolated placenta previa.
The control group consisted of healthy pregnant women with normal placental localization according to ultrasonography. The control group was formed by selecting pregnant women who were matched to the placenta previa group in terms of age, gestational week, and body mass index (BMI) to eliminate the possible effect of these factors on the midkine level. Patients with systemic diseases, such as chronic kidney and liver diseases, diabetes mellitus, known lung and heart diseases, history of malignancy, and twin pregnancies, were excluded from the study.
All blood samples were taken between 30–36 weeks of gestation. In order to provide homogeneity, study and control groups were matched at 300–336 and 340–360 weeks of gestation. Serum midkine levels were compared between the placenta previa and control groups in this gestational age groups. Furthermore, pathological examinations of the placentas were performed in available cases in terms of inflammatory changes.
Ultrasonography
The sonographic evaluations of all the participants were performed abdominally and vaginally using the Voluson E8 ultrasound equipment (GE Healthcare, Milwaukee, WI) by obstetricians (B.S., O.K.) with >5 years of experience in obstetric ultrasonography. The diagnosis of placenta previa was confirmed at the time of cesarean section.
According to the guidelines of the Royal College of Obstetricians and Gynaecologists (RCOG), placenta previa was defined as the edge of the placenta being a distance of <20 mm from the internal os after 16 weeks of gestation (Jauniaux et al., 2019a). Our study included patients whose diagnosis of placenta previa was confirmed by ultrasonography after 30 weeks of gestation. Patients diagnosed with placenta previa were evaluated in terms of PAS by ultrasonographic evaluation consisting of 10 parameters.
These parameters are placental lacunae, hypoechoic retroplacental space (“clear zone”), myometrial thinning, hyperechoic uterus–bladder interface (bladder line), focal exophytic mass and/or placental bulge, uterovesical hypervascularity, prior cesarean section, placental relationship with internal cervical os, subplacental hypervascularity, and diffuse or focal turbulent flow in the lacunae (Del Negro et al., 2020).
Operation decision
Type of the abdominal incision and cesarean technique were decided based on ultrasonographic and clinical findings before the delivery. For cases with low clinical suspicion for PAS, Pfannenstiel abdominal incision and low segment transverse uterine incision (Kerr incision) were preferred. However, vertical median abdominal incision and vertical median uterine incision at the fundal area were performed for cases with high clinical suspicion for PAS. All surgical procedures were performed by an experienced obstetric team managed by the same chief surgeon (D.S.). In the presence of obvious clinical findings for AIP such as deep full-thickness myometrial invasion, bladder invasion, or parametrial invasion, the surgical team directly progressed to cesarean hysterectomy.
Furthermore, no traction was applied to the umbilical cord and the surgical team waited for spontaneous separation of the placenta in cases with low invasion suspicion. In cases of the adherent placenta where spontaneous placenta did not separate, the bleeding was controlled by placing sutures on the adherent area.
Biological samples and analyses
All blood samples were collected in the late third trimester (between 30th and 36th weeks of gestation) as the comprehensive and final ultrasonographic possible diagnoses of PAS were made in this period in our institution. For the measurement of the midkine level, blood samples taken from the participants were centrifuged at 162 g for 15 min. The obtained plasma was stored at −80°C until the test day. The midkine level was measured with the immuno-based enzyme-linked immunosorbent assay method using a commercial kit (Human Midkine Elisa Kit, Bioassay Technology Laboratory) according to the manufacturer's instructions.
The sensitivity of the kit was 2.49 pg/mL with a detection range of 5–2000 pg/mL. BD Vacutainer™ SST™ II Advance Tube containing acrylic gel was used for blood sample collection. Owing to the nature of the acrylic gel in this tube, a stable barrier was provided between serum and clotted blood.
Statistical analysis
SPSS version 22 (IBM, Chicago, IL) was used for statistical analyses. The Kolmogorov–Smirnov test was conducted to determine whether the data with continuous values conformed to the normal distribution. The Mann–Whitney U test was used for the comparison of non-normally distributed (nonparametric) variables between the 2 groups, and the chi-square test for the comparison of categorical variables. Receiver operating characteristic (ROC) analysis and the Youden index were performed to determine the optimal cutoff values. A binary logistic regression analysis was performed to evaluate independent predictors of abnormal invasion in placenta previa cases. P < 0.05 was accepted as statistically significant.
Results
The study included 103 pregnant women, of whom 60 were healthy women with singleton pregnancies (control group) and 43 were diagnosed with placenta previa (case group). Table 1 presents the demographic characteristics, perinatal outcomes, and maternal serum midkine levels of all the participants. Age, BMI, and gestational week were similar in the placenta previa and control groups. Gravidity, parity, delivery week, fetal birth weight, and Apgar scores at the first minute were significantly different in the placenta previa group compared with the control group (P < 0.050).
Comparison of the Demographic Data, Perinatal Outcomes, and Maternal Serum Midkine Levels of the Groups
Statistically significant values were highlighted with bold.
Data are expressed as median (interquartile range) or count (percentage). Statistically significant at P < 0.05.
Gestational age at which the blood sample was taken.
kg: kilogram; m: meter; ng: nanogram; mL: milliliter.
BMI, body mass index.
When the maternal serum midkine levels were compared, the median midkine value was 0.18 ng/mL in the control group and 1.16 ng/mL in the placenta previa group. The midkine value was statistically significantly higher in the placenta previa group (P < 0.001). All placenta previa cases were delivered by cesarean section and 41 patients in the control group were delivered vaginally (P < 0.001).
Of the 43 patients in the placenta previa group, 29 were noninvasive placenta previa patients (isolated previa and placenta accreta), whereas 14 were invasive placenta previa (placenta increta and percreta) patients. The demographic data, perinatal outcomes, and maternal serum midkine levels of the patients are given in Table 2. The midkine level of patients with invasive placenta previa was 1.31 ng/mL, and the midkine level of those with noninvasive placenta previa was 1.12 ng/mL, revealing a statistically significant difference (P = 0.004).
Comparison of the Demographic Data, Perinatal Outcomes, and Maternal Serum Midkine Values According to the Invasion in the Placenta Previa Subgroup
Statistically significant values were highlighted with bold.
Data are expressed as median (interquartile range) or count (percentage). Statistically significant at P < 0.05.
kg: kilogram; m: meter; ng: nanogram; mL: milliliter.
Gestational age at which placenta previa was diagnosed.
Gestational age at which the blood sample was taken.
AIP, abnormally invasive placenta.
Table 3 gives the comparison of the 2 placenta previa subgroups in terms of clinical characteristics and laboratory values. In the AIP subgroup, operative time, number of patients who required blood transfusion, and length of hospital stay were significantly higher (P < 0.001). The number of patients admitted to the intensive care unit was also significantly higher in the invasive placenta previa subgroup (P = 0.003).
Comparison of the Clinical Characteristics and Laboratory Values According to the Invasion in the Placenta Previa Subgroup
Statistically significant values were highlighted with bold.
Data are expressed as median (interquartile range) or count (percentage). Statistically significant at p < 0.05.
g: gram; dL: deciliter.
ICU, intensive care unit.
When maternal serum midkine levels were compared according to gestational age subgroups, the placenta previa group had significantly higher values than controls. There were 25 placenta previa and 31 control patients in the 300–336 gestational age group and median serum midkine levels were 1.2 (IQR: 0.3) and 0.17 (IQR: 0.1), respectively, in the study and control groups (P < 0.001). In the 340–360 subgroup, there were 18 and 29 patients in the placenta previa and control groups, respectively. The placenta previa group (median: 1.15, IQR: 0.36) had again higher midkine values than controls (median: 0.18, IQR: 0.1) (P < 0.001).
Among 43 placenta previa cases, pathological examination was performed for 26 specimens and only 1 placenta had findings consistent with active suppurative inflammation.
ROC curve analysis was performed to evaluate the performance of maternal serum midkine level in identifying patients with placenta previa with invasion (Fig. 1). The optimal cutoff value of this parameter for the prediction of abnormal invasion was 1.19 ng/mL (area under the curve: 0.77, P = 0.004, 95% confidence interval [CI]: 0.63–0.91, sensitivity: 71.4%, specificity: 69%).
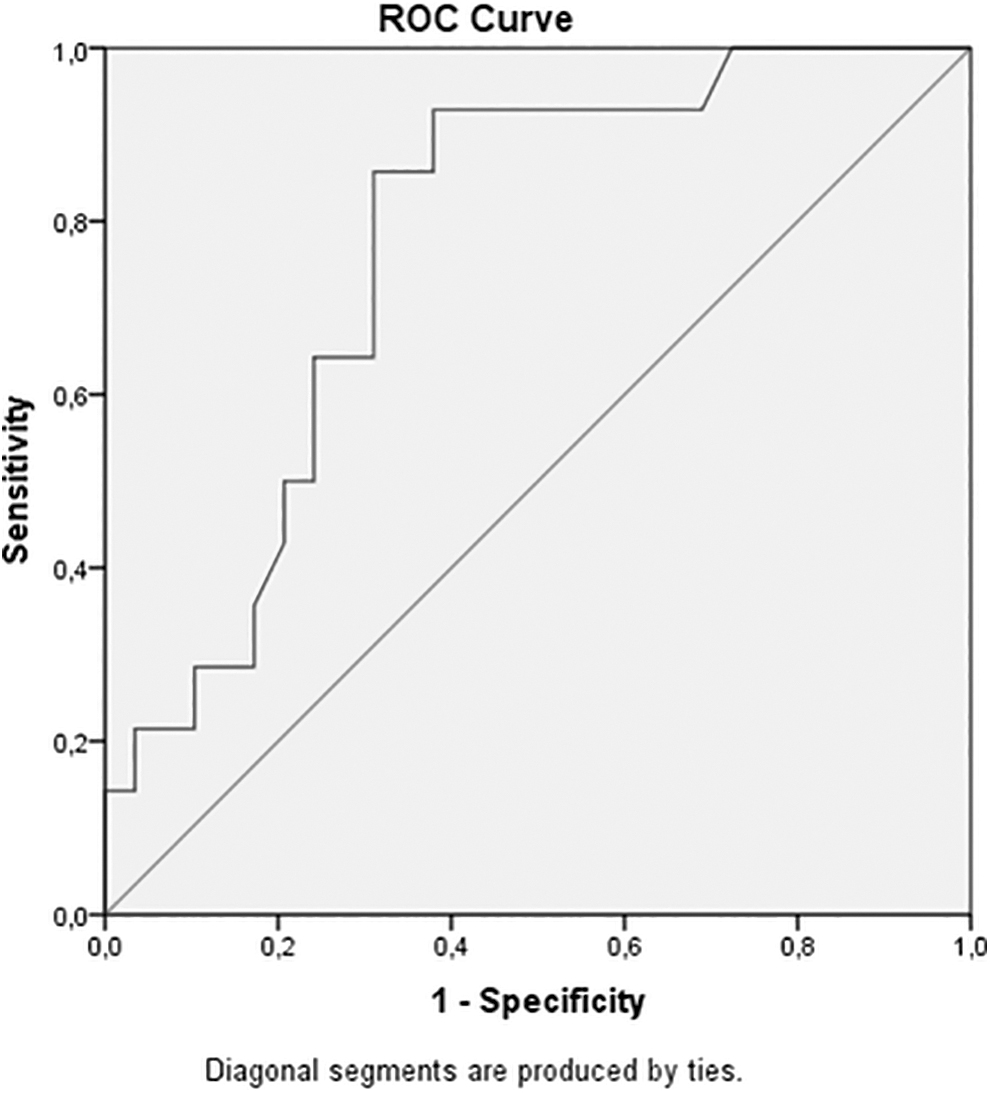
Receiver operating characteristic curve of the serum midkine level in the prediction of the AIP in the placenta previa group (optimal cutoff: 1.19 ng/dL, area under the curve: 0.77, P = 0.004, 95% CI: 0.63–0.91, sensitivity: 71.4%, specificity: 69%). AIP, abnormally invasive placenta; CI, confidence interval.
Binary logistic regression analysis for the determination of independent predictors for AIP among placenta previa cases is given in Table 4. According to the results of the regression analysis, BMI (odds ratio [OR]: 0.6, 95% CI: 0.5–0.9, P = 0.006), number of previous cesarean section deliveries (OR: 2.1, 95% CI: 1.1–3.5, P = 0.016), anterior placental location (OR: 5.5, 95% CI: 1.3–22.5, P = 0.016), ultrasonographic evaluation (OR: 2.1, 95% CI: 1.3–3.2, P = 0.001), and serum midkine level (OR: 27.8, 95% CI: 1.7–46.2, P = 0.010) were found to be the independent predictors of abnormal invasion in placenta previa.
Binary Logistic Regression Analysis for the Determination of Independent Predictors for Abnormally Invasive Placenta Among Placenta Previa Cases
Statistically significant values were highlighted with bold.
Statistically significant at p < 0.05.
CI, confidence interval; OR, odds ratio.
Discussion
This study evaluated whether the maternal serum midkine level could predict disease severity in patients with placenta previa. To the best of our knowledge, this is the first study on this subject. Our results showed that the serum midkine level was higher in the patients with placenta previa than in the healthy pregnant women. In addition, we found that the serum midkine level was higher in AIP cases than in placenta accreta and isolated placenta previa cases. Similar midkine levels were observed in the subgroups formed according to gestational age, and inflammatory findings were present only in 1 placenta specimen.
Placenta previa is a risk factor of PPH, with approximately half of patients with placenta previa experiencing PPH. If placenta previa patients are complicated with PAS, the rate of PPH increases further (Rosenberg et al., 2011). PAS can lead to PPH, resulting in blood transfusion, hysterectomy, surgical morbidity and mortality, multiple organ failure, and death (Allen et al., 2018).
Some studies have shown that preoperative evaluation and a multidisciplinary surgical approach are necessary to reduce the rate of complications related to PAS (Licon et al., 2020). It was previously stated that placenta increta/percreta from PAS patients represent more serious conditions and require life-saving surgical interventions due to PPH (Sumigama et al., 2007). In another study, it was concluded that placenta accreta does not put patients in a high-risk situation, and this risk is high in cases of placenta increta or percreta, which form the AIP group (Chalubinski et al., 2013).
Therefore, preoperative evaluation of placenta increta or percreta is crucial for predicting peripartum outcomes (Silver, 2015). In a recent consensus statement, patients with AIPs appear to require more intensive treatment, including planned preterm cesarean section hysterectomy (Committee, 2010). A meta-analysis reported that the rate of hysterectomy in patients diagnosed with prenatally AIP was 83.7% (Buca et al., 2018). In our study, all patients with AIP underwent hysterectomy. In addition, we did not have patients who underwent hysterectomy in isolated placenta previa and placenta accreta patients.
It is now crucial to develop prenatal screening protocols to further improve the outcome of this major obstetric complication, which has become increasingly common in recent years. Therefore, preoperative diagnosis of the AIP, especially in patients with placenta previa, is clinically important as it increases the risk of intraoperative bleeding and may change surgical management.
Midkine becomes involved in inflammatory processes through expression from damaged tissues. Furthermore, midkine can be considered an important cytokine associated with endothelial cell proliferation, vasodilation, and arteriogenesis (Yazihan et al., 2022). In addition to being derived from multiple embryonic tissues, midkine is expressed in the placenta (Obama et al., 1995). Studies have reported that inflammatory markers increase in patients with placenta previa (Keles et al., 2022). Since midkine is also an inflammatory marker, we hypothesized that midkine expression would be increased in patients with placenta previa.
Moreover, impaired placentation in PAS cases may be associated with tissue hypoxia, abnormal cell growth, excessive inflammation, and altered immune processes. It has been reported that midkine takes part in apoptosis, cell growth, and tissue reorganization (Filippou et al., 2020). Thus, midkine may have the potential to be used as a biomarker for placenta previa cases. In our study, when we compared the maternal serum midkine level between the placenta previa and control groups, the maternal serum midkine level was significantly higher in the former. We also presumed that the serum midkine level could change in patients with placenta previa at higher risk in terms of AIP.
Therefore, we compared serum midkine levels between pregnant women with AIP and those with placenta accreta and isolated placenta previa. As a result, we determined that the level of midkine was significantly higher in the abnormally invasive subgroup.
In a study based on biomarkers to predict the degree of placental invasion in patients with placenta previa, they concluded that serum VEGF levels were significantly negatively correlated with the clinical degree of AIP (Schwickert et al., 2021). To investigate the predictive value of biomarkers, a study of 54 pregnant women with placenta previa found that pro-B-type natriuretic peptide predicted placental invasion anomalies (Ersoy et al., 2016). In another study, placental growth factor was found at a higher level in patients with PAS than in those with placenta previa (Zhang et al., 2022).
Cai et al. found that soluble fms-like tyrosine kinase (sFlt) was lower in placenta increta/percreta than in placenta previa and placenta accreta and reported that it could be used to show the severity of PAS (Cai et al., 2022). Thus, biomarkers may be used in the prediction of placental invasion abnormalities. Similarly, the results of this study indicated that serum midkine level might be used in the prediction of AIP with appropriate sensitivity and specificity.
When we reviewed studies based on ultrasonographic findings to predict placental invasion in patients with placenta previa, a study of 106 women with placenta previa showed that loss of clear zone, abnormal placental lacunae, placental bulge, and bladder wall interruption reliably predicted abnormal invasive placenta (Sargent et al., 2023). Intermittent hypoechogenic spaces and lacunae may be present even in women with placenta previa without myometrial invasion, although they are associated with an increased likelihood of invasive placentation (Hamada et al., 2011).
In a study in which the degree of invasion was desired to be measured based on ultrasonography, it was found that placenta increta/percreta cases could be distinguished from placenta accreta and normal placentation with 100% sensitivity and specificity (Chalubinski et al., 2013). In a meta-analysis, it was concluded that the sensitivity of uterovesical hypervascularity was low (12.3%) for the detection of placenta accreta, and high for placenta increta (94.4%) and percreta (86.2%) (Pagani et al., 2018). In our ultrasonographic evaluation, we were able to correctly predict 12 (85.7%) of the 14 AIP patients.
Furthermore, the definitive diagnosis of the AIP is the histological evaluation of the uterus and the placenta. Ultrasonographic screening, clinical findings, obstetric history of the patients, and biomarkers may be used to help physicians detect high-risk cases for PAS. Therefore, it should be kept in mind that biomarkers such as midkine must be used in combination with ultrasonographic parameters to achieve favorable outcomes.
Strengths and limitations
This study has certain limitations. First, it had a single-center design and relatively low participants. Therefore, there is a need for multicenter studies with larger patient populations. Second, only 1 blood sample was taken from each participant. Future studies should examine the blood samples of all participants at regular intervals during all 3 trimesters of pregnancy. In contrast, the high number of study parameters, the presence of ultrasonographic evaluation, and the prospective design were the main strengths of this study.
Conclusion
This study showed that the serum midkine level was higher in the patients with placenta previa than in the healthy pregnant women. In addition, we found that the serum midkine level was higher in placenta previa cases with invasive placenta. In light of these results, the maternal serum midkine level may be a complementary biomarker for ultrasonography in the prediction of AIP in patients with placenta previa.
Footnotes
Authors' Contributions
All authors have read and approved the final article. All authors contributed to the following sections of the article and fulfilled the conditions for being an article writer.
R.D. contributed to formal analysis, software, review, and editing. N.F. contributed to writing—original draft, data curation, review, and editing. Ö.K. carried out conceptualization, writing—original draft, review, and editing.
O.O.Ö. was involved in methodology, data curation, review, and editing. B.S. was involved in formal analysis, data curation, review, and editing. D.Ş. took charge of methodology, supervision, review, and editing. A.T. took charge of conceptualization, original draft, review, and editing. E.T. was in charge of software, resources, review, and editing. N.Y. took charge of methodology, supervision, review, and editing.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.