
Abstract
Studying the levels of cytokines in the plasma of patients could be valuable in guiding immunotherapy policies. We assessed the plasma levels of 4 major cytokines [interferon (IFN)-β, interleukin-2 (IL-2), tumor necrosis factor alpha (TNF-α), transforming growth factor beta (TGF-β)] collected from 19 patients with ductal breast cancer (BCa), before surgery (BS) and 5 days after surgery (AS). The ratio AS/BS was also calculated and correlated with histopathological variables and tumor-infiltrating lymphocyte (TIL) density. The IFN-β and TNF-α levels were significantly higher in BCa patients, BS and AS, than healthy controls (P < 0.02). High IL-2 levels BS were linked with node involvement (P = 0.02), and marginally with HER2 expression (P = 0.08), while high TNF-α levels were linked with high PgR expression (P = 0.02). Increasing IFN-β, IL-2, and TNF-α levels were noted AS, which was more evident in patients with larger tumors. The TGF-β levels were significantly lower in BCa patients (P < 0.007). Linear regression analysis showed a direct association of IFN-β levels AS (P = 0.02, r = 0.52) and of TNF-α AS/BS-ratio (P = 0.001, r = 0.72) with TIL-density. It is suggested that although effector immune response is evident in the majority of early stage BCa patients, removal of the primary tumor further unblocks such responses.
Introduction
Tumors are often characterized by an inflammatory microenvironment as a result of chemotaxis of lymphocytes, monocytes, and neutrophils that infiltrate the tumor stroma. Activated immune cells produce inflammatory proteins and cytokines that may block tumor growth or, on the contrary, suppress cytotoxic T cell and macrophage activity (Lan et al., 2021). Studying the levels of cytokines in the plasma of patients may identify distinct immune responses. Such information can be of prognostic relevance and eventually could be valuable in guiding immunotherapy policies (Kartikasari et al., 2021).
Several cytokines have focused attention on translational and clinical research. Interleukin-2 (IL-2) activates antitumor immune responses, and recombinant rIL-2 has been used in the past for treating melanoma and renal cell carcinoma (Abbas et al., 2018). IL-2 promotes T cell and natural killer cells (NK) proliferation and activation, enhancing their cytotoxic activity, although binding to IL-2RA receptors on regulatory T cells can also promote immunosuppression (Buckner, 2010). Tumor necrosis factor alpha (TNF-α) is another cytokine with strong antitumor activity, produced by macrophages, T cells, and NK-cells (van Horssen et al., 2006). Binding of TNF-α to its receptor TNFR-1 induces apoptotic cell death (Ashkenazi and Dixit, 1998).
Type I interferons (IFNs), like IFN-α and -β, exert their activity via binding to heterodimeric receptors IFNAR-1 and 2, followed by phosphorylation of JAK1 and Tyrosine kinase 2, and transcriptional activation of over 100 IFN-stimulated genes (Cheon et al., 2014). These may have various effects, including apoptosis, differentiation, inhibition of metastasis and angiogenesis, and cytotoxic T-cell activation (Cheon et al., 2014; González-Navajas et al., 2012; Parker et al., 2016). Transforming growth factor beta (TGF-β) is a cytokine with strong immunosuppressive properties and direct effects on cancer cells. Although it can block premalignant cell proliferation, it can promote cancer cell growth and epithelial-to-mesenchymal transition. It can also promote angiogenesis and metastasis (Hao et al., 2019; Xie et al., 2018; Yang and Moses, 2008).
In the current pilot study, we assessed the levels of the above 4 critical for the antitumor response cytokines in the plasma of patients with localized breast cancer (BCa) before surgery (BS) and after surgery (AS). Initial levels and changes AS were correlated with the tumor size, node metastasis, steroid receptor, and HER2 expression. Cytokine plasma levels were further examined in parallel with the density of tumor-infiltrating lymphocytes (TILs).
Materials and Methods
Patients and disease
We analyzed plasma collected from 19 patients with ductal BCa, BS, and 5 days AS. All patients had been treated at the University Hospital of Alexandroupolis with conservative breast surgery and limited lymph-node dissection or modified radical mastectomy, between 2021 and 2022. Postoperative chemotherapy and radiotherapy was administered according to the 2019 guidelines, as reported for the postoperative management of BCa patients (adjuvant systemic treatment) (Burstein et al., 2019). Although neoadjuvant chemotherapy is gradually accepted as the gold standard for Her2 positive and triple negative patients (Curigliano et al., 2023), none of the recruited herein patients had received any form of chemotherapy or radiotherapy BS. This allowed to assess the cytokine levels in chemotherapy naïve patients immediately BS and AS alone. An additional cohort of plasma collected from 6 healthy control women who were examined in our clinic for benign breast diseases, but did not undergo surgery, was also analyzed. Paraffin-embedded tissue material was available for the assessment of TILs.
Enzyme linked immunosorbent assay
Ten milliliters blood from each patient, before and after the operation, were collected in EDTA tubes. Samples were immediately centrifuged at 1.500g for 10 min, and plasma samples were stored at −80°C. ELISA assays were used for the detection of TGF-β, TNF-α, IL-2, and IFN-β, respectively, following the instructions of the technical manual for each assay. First, standard curves were prepared using different dilution series for each protein. Plasma samples, before and after the operation, were tested in duplicates.
Briefly, the Assay Genie Sandwich ELISA kit (Cat. No. HUFI00262; Assay Genie, Dublin, Ireland) was used for TNF-α. A standard curve was generated in a range of 0–1,000 pg/mL. Each sample was tested in duplicates adding 100 μL of sample in each well. TGF-β1 levels were detected in plasma samples using the ELISA Genie TGFB1 (Cat. No. HUEB0149; Assay Genie). Its standard curve ranges from 0 to 5,000 pg/mL, while 100 μL of each sample in duplicates are used, as well. Human IL-2 levels were detected using SimpleStep ELISA® Kit (ab270883; Cambridge, UK) with a standard curve ranging between 0 and 4,000 pg/mL. IFN-β levels were detected with Human Interferon beta SimpleStep ELISA Kit (ab278127; Cambridge, UK) with a standard curve ranging between 0 and 1,200 pg/mL. For these latter kits, 50 μL per sample was used in duplicates for standard and test samples.
The optical density (O.D.) absorbance at 450 nm was read using OMEGA Microplate reader for all ELISA assays. The relative O.D. 450 nm was calculated using the following equation:
Assessment of TIL-density
TIL quantification was performed on hematoxylin and eosin-stained slides. The number of TILs was assessed in all high-power × 40 fields in the stroma of 2 distinct tumor areas: (1) the invading front, thus the stroma in the optical field that comprises tumor and adjacent normal breast tissue, and (2) inner tumor areas, thus the stroma surrounding the BCa foci while moving the optical fields away from the tumor front and toward the center of the tumor. The mean values were obtained to score the TIL-density (or TIL-score) in the invading tumor front (TILinv) and in inner tumor areas (TILinn) separately.
Statistical analysis
Statistical analysis was performed with the GraphPad Prism 7.0 package. Categorical variables were compared with the chi-square t-test. Groups of continuous variables were compared with the nonparametric Wilcoxon matched-pairs signed rank test or the unpaired nonparametric Mann–Whitney test, as appropriate. Linear regression analysis was applied to assess correlations between continuous variables. A P value <0.05 was considered for significance.
Results
IFN-β plasma levels
The plasma levels of IFN-β ranged from 20 to 73 pg/mL in healthy controls (median 33), 12.2 to 1,459 pg/mL (median 104) in BCa patients BS, and 21.5 to 946 pg/mL (median 94) in BCa patients AS. The IFN-β levels were significantly higher in BCa patients, whether BS or AS, compared to healthy controls (P = 0.02 and 0.01, respectively) (Fig. 1a). There was no difference between the concentrations recorded BS and AS (P = 0.29).
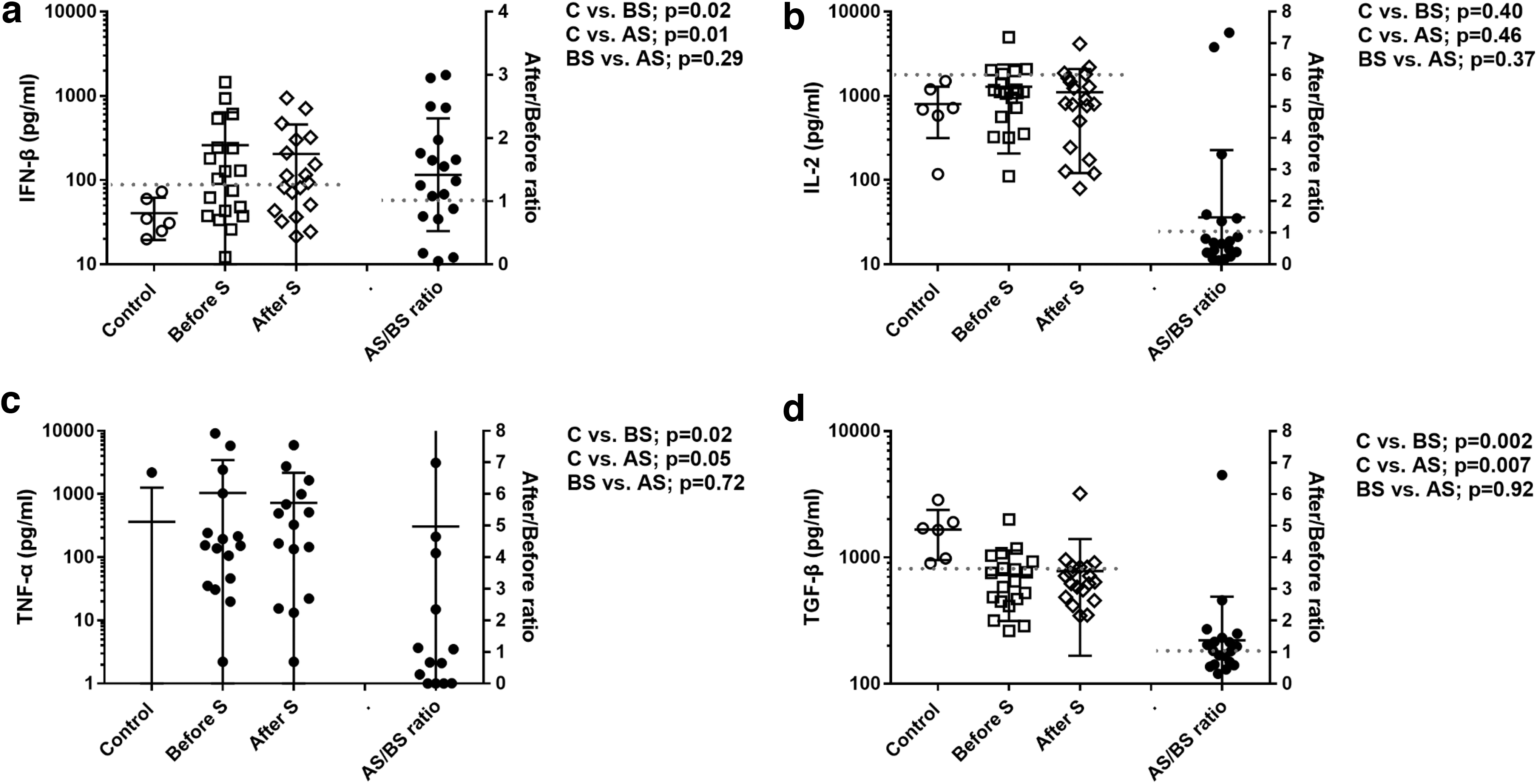
Cytokine levels in healthy controls, BCa patients BS and AS, and the AS/BS ratio:
Eleven out of 19 patients (57.8%) had IFN-β plasma levels BS higher than the controls. Twelve out of 19 patients (63.1%) had IFN-β plasma levels AS higher than the controls. Patients were split into 2 categories of normal versus high IFN-β levels BS. Analysis according to the histopathological variables showed no significant differences (Table 1). However, a marginal association of tumors with lack of PgR expression with high IFN-β levels was noted (P = 0.06, respectively) (Table 1). Analysis according to the BCa subtype did not reveal any significant association (Table 1).
Association of Interferon-β Levels Before and After Surgery, and of the After Surgery/Before Surgery-Ratio with Histopathological and Molecular Variables
T1 versus T2,3.
Luminal-A-like = ER+, PgR+ and her2 negative; Luminal-B-like = ER+, PgR negative and Her2 negative; Luminal-Her2 = ER+/Her2+; Her2 (enriched) = ER and PgR negative/Her2+; Triple negative = ER/PgR/Her2 negative.
AS, after surgery; BCa, breast cancer; BS, before surgery; IFN, interferon.
The ratio AS/BS of plasma IFN-β (<1: reducing versus >1: increasing levels AS) ranged from 0.05 to 3.0. Thirteen out of 19 patients had increasing IFN-β plasma levels AS (range 1.08–3.0-fold). Six out of 19 patients had decreasing IFN-β plasma levels AS (range 0.05–0.88-fold). Larger T2,3-staged tumors had significantly higher IFN-β AS/BS-ratio than small tumors (P = 0.02) (Table 1).
IL-2 plasma levels
The plasma levels of IL-2 ranged from 118 to 1,499 pg/mL in healthy controls (median 705), 111 to 4,979 pg/mL in BCa patients BS (median 1,115), and 79 to 4,149 pg/mL AS (median 815). There was no significant difference between controls and BCa patients (P > 0.40). There was no significant difference between the BS and AS IL-2 levels (P = 0.37) (Fig. 1b).
Five out of 19 patients had higher than the control IL-2 plasma levels BS (range 1,812–4,978 pg/mL). Five out of 19 patients had higher than the control IL-2 plasma levels AS (range 1,627–4,148 pg/mL). Patients were split into 2 categories of normal versus high IL-2 levels according to the BS levels. Analysis according to the histopathological variables showed that high IL-2 levels BS were linked with node involvement (P = 0.02) and were marginally related to HER2 expression (P = 0.08) (Table 2). Analysis according to the BCa subtype showed significantly higher levels of IL-2 in patients with Lumina-A/B-type compared to Luminal-Her-2 type (P = 0.01) (Table 2).
Association of Interleukin-2 Levels Before and After) Surgery, and of the After Surgery/Before Surgery-Ratio with Histopathological and Molecular Variables
T1 versus T2,3.
Luminal-A-like = ER+, PgR+ and her2 negative; Luminal-B-like = ER+, PgR negative and Her2 negative; Luminal-Her2 = ER+/Her2+; Her2 (enriched) = ER and PgR negative/Her2+; Triple negative = ER/PgR/Her2 negative.
Luminal-A and B-like versus Luminal-Her 2: P = 0.01.
IL-2, interleukin-2.
The AS/BS-ratio of plasma IL-2 ranged from 0.12 to 17.5. Seven out of 19 patients had increasing IL-2 plasma levels AS (range 1.36–17.5-fold). Twelve out of 19 patients had decreasing IL-2 plasma levels AS (range 0.12–0.87-fold) (Fig. 1b). Larger T2,3-stage tumors had a significantly higher AS/BS ratio (0.02).
TNF-α plasma levels
The plasma levels of TNF-α ranged from 0 to 2,195 pg/mL in healthy controls (median 0). In fact, 5/6 controls had no detectable levels, while 1 had very high. BS TNF-α levels ranged from 0 to 9,157 pg/mL (median 139), while AS these ranged from 0 to 5,942 pg/mL (median 145). Three BCa patients BS and 4 AS had no detectable TNF-α levels. The TNF-α levels were significantly higher in BCa patients compared to healthy controls (P = 0.02 and 0.05 for TNF-α levels measured BS and AS, respectively) (Fig. 1d).
As TNF-α levels were undetectable primarily in controls, still detectable in 16/19 BC patients, BC cases were split into 2 categories of low versus high TNF-α taking as a cut-off point the median BS value recorded (139 ng/mL). Ten patients had low levels and 9 high BS levels. Analysis according to the histopathological variables showed a significant association of high TNF-α levels with positive PgR expression (P = 0.02) and marginally with high ER expression (P = 0.06) (Table 3). Analysis according to the BCa subtype did not reveal any significant association (Table 3).
Association of Tumor Necrosis Factor Alpha Levels Before and After Surgery, and of the After Surgery/Before Surgery-Ratio with Histopathological and Molecular Variables
T1 versus T2,3.
Luminal-A-like = ER+, PgR+ and Her2 negative; Luminal-B-like = ER+, PgR negative and Her2 negative; Luminal-her2 = ER+/Her2+; Her2 (enriched) = ER and PgR negative/Her2+; Triple negative = ER/PgR/Her2 negative.
TNF-α, tumor necrosis factor alpha.
In 11/19 patients, the TNF-α levels increased in AS samples (AS/BS-ratio >1), in 7 decreased (AS/BS-ratio <1), while 1 patient had undetectable levels BS and AS. Analysis of patients according to the TNF-α levels showed no significant association (Table 3).
TGF-β plasma levels
The plasma levels of TGF-β ranged from 901 to 2,856 pg/mL in healthy controls (median 1,676), 262 to 1,998 pg/mL (median 646) in BCa patients BS, and 346 to 3,205 pg/mL (median 638) in BCa patients AS. The TGF-β levels were significantly lower in BCa patients compared to healthy controls (P = 0.002 and 0.007 for TGF-β levels measured BS and AS, respectively) (Fig. 1c).
Fourteen out of 19 patients had TGF-β BS plasma levels lower than the controls. Sixteen out of 19 patients had TGF-β AS plasma levels lower than the controls. Cases were split into 2 categories of normal versus low TGF-β BS-levels. Analysis according to the histopathological variables showed no significant associations (Table 4). Analysis according to the BCa subtype did not reveal any significant association (Table 4).
Association of Transforming Growth Factor Beta Levels Before and After Surgery, and of the After Surgery/Before Surgery-Ratio with Histopathological and Molecular Variables
T1 versus T2,3.
Luminal-A-like = ER+, PgR+ and Her2 negative; Luminal-B-like = ER+, PgR negative and Her2 negative; Luminal-her2 = ER+/Her2+; Her2 (enriched) = ER and PgR negative/Her2+; Triple negative = ER/PgR/Her2 negative.
TGF-β, transforming growth factor beta.
The AS/BS-ratio of plasma TGF-β ranged from 0.31 to 6.61. Eleven out of 19 patients had increasing TGF-β plasma levels AS (range 1.04–6.61-fold). Eight out of 19 patients had decreasing TGF-β plasma levels AS (range 0.32–0.90-fold). There was no significant association with histopathological variable, although an increasing AS/BS-ratio was noted in ER-negative patients (Table 4).
TILs and plasma cytokine levels
The TIL-density was significantly higher in the invading tumor front compared to inner tumor areas (P < 0.0001) (Fig. 2a). This ranged from 4 to 165 (median 52, 33rd percentile 42, 67th percentile 75) in the invading tumor front versus 1 to 73 (median 9, 33rd percentile 4, 67th percentile 26) in inner tumor areas. Figure 2b shows a typical immunohistochemical image of a BCa tumor with high TIL-density in the inner tumor areas.

TIL-density and association with cytokine levels:
Linear regression analysis between the TIL-densities in the invading front or inner areas with the cytokine levels BS did not show any significant association. A direct association of IFN-β levels AS (P = 0.02, r = 0.52) and of high TNF-α A/B-ratio (P = 0.001, r = 0.72) with high TIL-density in inner tumor areas was noted (Fig. 2c and d).
Discussion
Assessment of the cytokine levels BS and monitoring their changes AS may provide a patient-specific profile of interactions between the tumor and host. In the current pilot study, we assessed the levels of 4 important cytokines, IFN-β, IL-2, TNF-α, and TGF-β in the plasma of BCa patients, BS and AS.
IFN-β is a member of the IFN-type I cellular response cascade, a key pathway regulator of antiviral and antineoplastic immune response. The IFN type I pathway starts with the exposure of immune cells to viral and bacterial antigens, or DNA and RNA fragments released by cancer cells, which are followed by activation of stimulated interferon gene (STING) and transcription of IFN-β that is secreted in the tumor environment. This binds to specific receptors on immune and cancer cells and triggers the downstream expression of a large number of IFN-stimulated genes (Mazewski et al., 2020). Cancer cell damage by radiation and chemotherapy may also trigger the IFN-type-I response in the cancer cell itself so that the cancer cell becomes the source of IFNs and IFN-stimulated proteins that induce antitumor immunity (Zhang et al., 2020). High preoperative levels of IFN-β in the plasma of patients with BCa may, therefore, be a result of an intensified activation of lymphocytes and monocytes by cancer cell DNA fragments or of interactions with activated tumor-recognizing dendritic cells.
Indeed, in the current study, significantly high levels of plasma IFN-β were recorded in BCa patients compared to healthy controls in 57% of patients. Frequently, tumors from these patients had a more lack of PgR expression and intense tumor infiltration by lymphocytes. However, this latter finding reached statistical significance only for the postoperative IFN-β levels. The reason for increasing IFN-β levels 5 days AS in 13/19 patients is compatible with an intensification of the antitumor immune response. This effect was more prominent in patients with larger tumors. It can be hypothesized that the removal of the primary tumor may have removed immunological obstacles suppressing the IFN-type-I response. Primary tumors suppress the immune response in tumor-draining lymph nodes (TDLNs) due to acidic lymph and immunosuppressive cytokine drainage into the lymph nodes (Koukourakis and Giatromanolaki, 2022). Thus, removal of the primary tumor may unleash dendritic cell function in the TDLNs and enhance IFN-Type-I response. This hypothesis may also explain why the prominent immune response as assessed with a high tumor TIL-density was linked with increasing IFN-β plasma levels only AS.
IL-2 is another important cytokine involved in antitumor immune response. IL-2; however, may promote proliferation of cytotoxic, memory, and regulatory T cells, exerting a dual effect on the immune system (Abbas et al., 2018). In our study, about one-fourth of BCa patients had IL-2 levels higher than controls. A higher incidence of lymph node involvement was noted in these patients, together with a marginal prevalence of a HER2+ tumor phenotype. This finding is in accordance with a study by Saglam et al. (2009) where IL-2 levels in 50 BCa patients were significantly related to HER2 expression by cancer cells, which made the authors speculate an activation of T cells by HER2 peptides. Such an activation appears, however, inefficient, as in our study high IL-2 levels were linked with metastasis to the lymph nodes.
Another interesting finding was that similar to IFN-β levels, increasing IL-2 levels were noted in 7/19 patients AS, and this was related with larger tumors. Again, unblocking TDLN antitumor immune function after removal of the primary tumor may account for this finding. This effect could have been more robust in larger tumors that may have had a stronger immunosuppressive effect before their removal. A study by Zhang et al. (2018) in 43 BCa patients suggested that basal levels of IL-2 are higher in patients with high levels of circulating tumor cells, thus aggressive tumors, compatible with our finding of a direct association of IL-2 with node metastasis. However, IL-2 levels decreased in patients with persistent circulating cancer cells after therapy, which may be a result of tumor-induced suppression of IL-2 released by immune cells.
The levels of TNF-α, a potent cytokine secreted by activated macrophages, T-cells, and NK-cells that induce cell cancer cell death after binding to specific TNF-receptors (Ashkenazi and Dixit, 1998; van Horssen et al., 2006) were, overall, undetectable in healthy individuals, at least using the herein applied ELISA test. In contrast, TNF-α levels were significantly increased in BCa patients at baseline and AS. Tesarová et al. (2000) also found significantly increased TNF-α levels in BCa patients compared to controls.
In our study, using the median levels as a cut-off point, patients with high TNF-α levels BS had tumors with a frequent expression of PgR and ER expression. This finding was inverse to the one noted with IFN-β levels. In 11/19 patients, TNF-α was increased AS, following the same pattern noted for IL-2 and IFN-β. Although this finding contrasts a study by Tesarová et al., where TNF-α levels decreased after therapy, TNF-α levels were measured 3 months after therapy verus 5 days in the current study. Berberoglu et al. also found decreased TNF-α levels in patients with locally advanced BCa treated with neoadjuvant chemotherapy who showed partial or complete response. However, this is again a long-term outcome and not an immediate postsurgery effect (Berberoglu et al., 2004).
In contrast to the above-discussed cytokines that are rather related to antitumor response, TGF-β is a potent immunosuppressive cytokine with direct effects on cancer cell growth, epithelial-to-mesenchymal transition, and also effects on intratumoral angiogenesis and metastasis (Hao et al., 2019; Xie et al., 2018; Yang and Moses, 2008). TGF-β promotes differentiation of CD4+ T cells to regulatory Tcells, promotes monocyte differentiation to M2-type, and blocks cytotoxic T-cell activity by binding to specific TGF-receptors (Fu et al., 2004; Zhang et al., 2016).
In our study, these immunosuppressive cytokine levels were lower overall in BCa patients compared to healthy controls. This was noted in 73% of patients, but no relation to histopathological variables was noted. Sminia et al. (1998) found elevated TGF-β levels in 25% of BCa patients versus 5% of controls, while Wakefield et al. (1995) reported that most BCa patients have TGF-β levels within the normal levels. Ivanović et al. (2003) also reported that TGF-β levels are high in advanced BCa disease (stage IIIb/IV), while Panis et al. (2013) found that TGF-β levels were lower in patients with metastasis and triple-negative tumors. Grau et al. (2008) found no association of TGF-β levels with stage of disease. Following surgery, TGF-β levels increased in 11/19 patients, which was more frequent in patients with ER-negative tumors. Kong et al. (1995) found that in node-negative BCa patients, TGF-β dropped to normal levels AS, while these were increased in node-positive patients.
We further examined the hypothesis that the above cytokines may be involved in the regulation of infiltration of tumors with lymphocytes. The TIL-density was assessed in the surgical samples of our patients. Indeed, high IFN-β and increasing TNF-α levels AS were linked with high TIL-density in inner tumor areas. The pre-operative levels were not linked with TIL-density, however, and none of the cytokines was linked with TIL-density in the invading tumor front. As the TIL-density dropped significantly in inner tumor areas compared to the tumor periphery, it is suggested that microenvironmental conditions may inhibit survival and proliferation in inner tumor areas. Hypoxia and acidity may underlie the phenomenon, as previously shown (Giatromanolaki et al., 2022).
The overall patterns of findings are difficult to interpret. The complexity of the interactions between cytokines, lymphocytes, and microenvironment conditions should better be studied separately in the specific BCa subtype, which is not feasible within the context of the current study that recruited limited number of patients. Triple negative and HER2+ enriched BCa are more immunogenic. In an analysis of 3,771 patients treated with NAC, high TIL density was noted in 13%, 19%, and 30% of luminal HER2−, HER2+, and Triple Negative Breast Cancer, respectively (Denkert et al., 2018). Whether cytokines are involved in the differential immunologic response demand further investigation.
Conclusions
This pilot study suggests that cytokines supporting cytotoxic antitumor activity, that is, IFN-β, IL-2, and TNF-α are increased in the plasma of BCa patients, and these levels are further increased AS. This latter effect was stronger in patients with larger tumors. TGF-β levels were low in most patients analyzed. It is speculated that although effector immune response is evident in the majority of early stage BCa patients, removal of the primary tumor further unblocks such responses in the TDLNs in a subgroup of patients that were partially suppressed eventually by the lymph arriving at the TDLNs.
Availability of Data and Material
All data reported in the study are available in our departments.
Ethics Approval
The study has been approved by the local ethics and research committee (ΕΣ6/Θ1/6-4-2023, Protocol No. 7017/09.02.2023), and informed consent was obtained from all individual participants included in the study. All procedures performed in the study were in accordance with the ethical standards of the institutional and the national research committee and with the 1964 Helsinki Declaration and its later amendments.
Consent for Publication
There are no individual person's data included in the article.
Footnotes
Authors' Contributions
E.K.: conception and design, analysis, and interpretation of data, writing of the article. C.T.: conception and design, analysis, and interpretation of data, writing of the article. A.M.: ELISA assessment, analysis, writing of the article. A.G.G.: immunohistochemistry assessment, analysis, writing of the article. E.E.: acquisition of data, surgery, blood sampling, writing of the article. D.K.: acquisition of data, surgery, blood sampling, writing of the article. K.N.: interpretation of data, writing of the article. N.N.: ELISA assessment, analysis, writing of the article. A.G.: immunohistochemistry assessment, analysis, writing of the article. M.I.K.: conception and design, analysis, and interpretation of data, writing of the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study has been financially supported by the Democritus University Special Account, project number 81006.