
Abstract
Despite the promising results of immunotherapy, further experiments need to be considered because of several factors ranging from physical barriers to off-tumor adverse effects. It is surprising that adoptive cellular immunotherapy, particularly dendritic cell and cytokine-induced killer (DC-CIK) therapy, is far less emphasized in the treatment of cancer diseases. DC-CIK therapy in cancer patients presents auspicious results with low or no side effects, which should not be overlooked. More interestingly, almost all DC-CIK clinical trials are ongoing in China that highlight the limitations of therapeutic strategies and require large-scale research. To date, it is advisable to consider combination therapy with chemotherapy since it has shown promising outcomes with higher efficacy. In this article, the efficacy of DC-CIK therapy in patients with cancer is summarized by underscoring the lack of experiments on soft cancers on an unprecedented scale. In brief, DC-CIK therapy is a safe and effective therapeutic agent for malignant and nonmalignant diseases that enhances short-term and long-term effects.
Introduction
Immunotherapy has gained importance in recent years due to the limited effectiveness of traditional treatments such as chemotherapy (CT), surgery, radiation, and amputation. Adoptive cell therapy, which includes cancer vaccines, chimeric antigen receptor (CAR) therapy, and dendritic cell (DC) vaccines, along with innate immunity and immune checkpoint inhibitors (ICIs), has shown more promising results. However, each therapeutic strategy faces obstacles and limitations that restrict its potential. CAR-T cell therapy has shown positive outcomes in blood cancers but is less effective against solid tumors due to barriers such as physical obstacles, limited T cell infiltration, and tumor cells using immune checkpoint (ICP) to evade immune surveillance and induce apoptosis in CAR cells (Ye et al., 2018).
The targeting of ICIs, such as PD-L1, CTLA-4, LAG-3, and others, which are present in tumor cells, is widely recognized for the potential to revolutionize cancer treatment by creating an environment conducive to tumor growth and invasion (Meftahpour et al., 2022). Therefore, it is not surprising that combination therapy is of primary importance since malignant cancers exhibit various pathways to survive and metastasize.
Cytokine-induced killer (CIK) cells belong to a specific group of non-major histocompatibility complex (MHC) restriction natural killer (NK) T lymphocytes and T cells marked by the presence of CD3+ CD56+. CIK cells' abilities are not limited to quick growth in vitro [through the cocultivation of peripheral blood lymphocytes with the anti-CD3 monoclonal antibody, interleukin (IL)-2, IL-1α, and IFN-γ] and exhibit more potent antitumor effects with lower toxicity, and in comparison, with other targeted therapies, bind with a wider range of tumor cells. Hence, evaluating the effectiveness of CIK cells in cancer patients has shown promising results (Tao et al., 2014). More than 50 trials are currently being conducted to assess the effectiveness of CIK cells in treating various forms of cancer, as stated on
The first clinical trial involving CIK cells in patients was recorded in 1999, where Hoyle et al. (1998) demonstrated that CIK cells have the ability to eliminate both autologous and allogeneic chronic myeloid leukemia (CML) cells, indicating their potential as a curative treatment for CML. In addition, this study revealed that CIK cells can effectively inhibit the growth of CML. Another study conducted by Kornacker reported the suppression of chronic lymphocytic leukemia cells by CIK cells. Meanwhile, other studies have confirmed the cytotoxic properties of CIK cells in patients with alveolar rhabdomyosarcoma, Ewing sarcoma, glioblastoma multiforme, retinoblastoma cell lines, and other types of cancer (Kornacker et al., 2006). Since the exact mechanisms responsible for the cytotoxicity of CIK cells have not been fully understood yet, many experiments are being carried out and, presently, certain factors and signaling approaches have been identified.
Attempts to prevent the cytotoxic activity by using blocking antibodies against CD2, CD3, CD8, CD28, CD56, VLA-4, TCR αβ, and MHC class I and II molecules were unsuccessful, indicating that CIK cells recognize their targets through a method that is independent of MHC. On the contrary, cell-to-cell contact seems essential to CIK when it comes to lysing cell activity by blocking lymphocyte function-associated antigen 1 (LFA-1) and intracellular cell adhesion molecule 1 (ICAM-1). Although the use of immunosuppressive drugs, such as cyclosporine and FK506, inhibits the release of granules by CIK cells when stimulated through the CD3–TCR interaction, the cytotoxicity triggered by interaction with tumor targets remains.
The natural killer group 2-member D (NKG2D) receptor, found within the NK gene complex on human chromosome 12p12-p13, is believed to have a correlation with CIK cell activities. NKG2D is a versatile receptor that can identify at least six counter ligands, including MHC class I chain-related A (MICA), MICB, and members of the UL16-binding proteins (ULBP) family, which are involved in malignant tumors (Introna and Correnti, 2018).
However, it is worth noting that the therapeutic application of autologous and allogeneic CIK has sparked a vast array of topics, as it gives disparate results. For example, one study indicated that CD8+ CIK cells that were expanded from C57BL/6 (H2b) mice showed little to no ability to kill their bone marrow cells, but were highly effective in killing BCL-1 lymphoma tumor cells. When the CD8+ CIK cells from C57BL/6 (H-2b) mice were used in an allogeneic setting, they were able to kill both bone marrow and tumor cells from Balb/c (H2d) mice. However, the killing of bone marrow cells was less compared with the killing of tumor cells, indicating a preference for malignant cells. What is more, Wang et al. (2010) discovered the higher antitumor property of semiallogeneic DC-CIK in patients with renal carcinoma.
Precisely, this experiment showed the enhanced ratios of CD3+CD56+ cells and the remained cytotoxicity impacts of CIK cells by promoting the release of IFN-γ.
The researchers found that when autologous DCs were cocultured with CIK cells, the CIK cells showed increased proliferation and enhanced ability to kill tumor cells (Märten et al., 2001). DCs are a specific kind of cells that present tumor antigens to T lymphocytes, resulting in the creation of a cytotoxic T lymphocyte response and an immune reaction against the tumor. In other words, DCs, which play a crucial role in presenting antigens to the immune system, can secrete various cytokines such as Interferon (IFN) and IL-12. This allows them to modulate the immune response against tumors through multiple mechanisms. The utilization of autologous DC-CIK cells as a treatment has demonstrated encouraging outcomes in clinical settings for different solid cancer types, such as liver cancer, colon cancer, kidney cancer, and breast cancer (BC) (Hongeng et al., 2003; Wang et al., 2006).
From a bird's eye view, the potential of CIK therapy in combination with other applications is often overlooked, as there are unprecedentedly fewer ongoing clinical trials compared with other therapies. As a result, we aim to summarize the therapeutic applications of CIK-combination therapy, including DC-CIK, DC-CIK-CAR T cells, DC-CIK-ICP inhibitors, and DC-CIK-chemotherapies for various types of cancers.
DC–CIK Combination Therapies in Malignancies
From the outside looking in, combination therapy has gained scrupulous attention in cancer treatment due to the limited success of monotherapy. Factors such as toxicity and the inability to identify tumor-associated antigens have hindered the effectiveness of single treatments. However, when CIK therapy is combined with other therapeutic applications, it has shown promising results in prolonging the overall survival (OS) and complementing the advantages of each treatment. Studies have shown that when CIK therapy is combined with DCs, there is an increase in the presence of immune-boosting surface molecules and a higher secretion of IL-12 by DCs. In addition, coculturing CIK cells with DCs improves the ability of CIK cells to destroy tumor cells, even those that are resistant to CIK therapy alone.
These promising results from preclinical research have prompted clinical trials to explore the potential of combining DC-CIK therapy with other therapeutic applications such as CAR-T cells, ICI, and CT for treating solid tumors (Zhang and Schmidt-Wolf, 2020). In Fig. 1, we illustrate the ex vivo expansion of CIK combined with DCs.
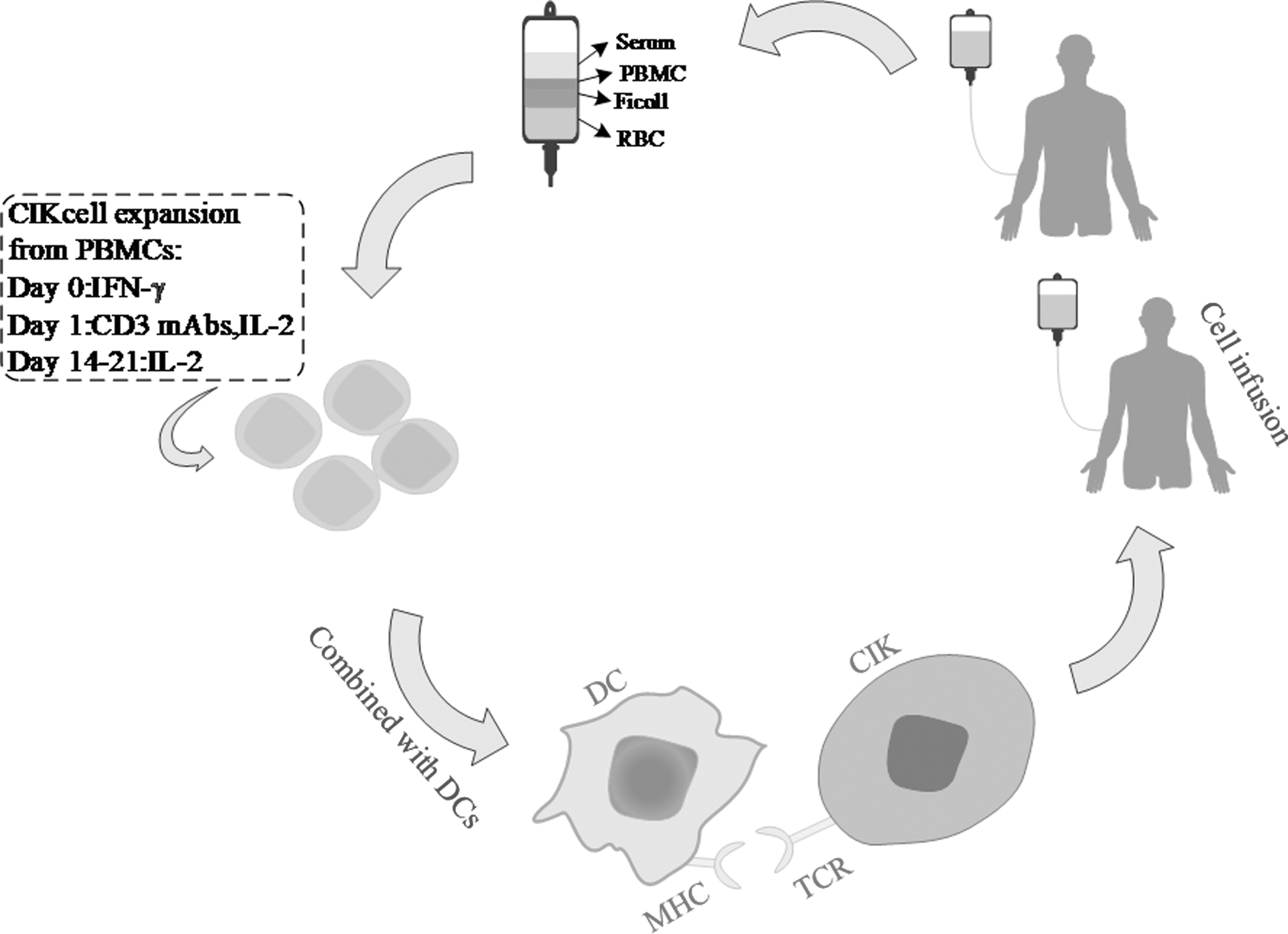
Ex vivo expansion of CIK cells and infusion. Methods for improving the effectiveness of CIK cells in clinical treatment can include isolating PBMCs through density gradient centrifugation and expanding them with IFN-γ, anti-CD3, and IL-2. These expanded CIK cells can then be infused into the patient after a period of 14–21 days. To enhance the antitumor activity of CIK cells, cytokines such as IL-18 can be added during the expansion process. In addition, DCs, which have a strong ability to present tumor antigens, can compensate for the lack of tumor antigen specificity in CIK cells. CIK, cytokine-induced killer; DCs, dendritic cells; PBMCs, peripheral blood mononuclear cells.
Nonsmall cell lung cancer
Nonsmall cell lung cancer (NSCLC) is a major contributor to global cancer-related fatalities (Jemal et al., 2011). Evidently, the epidermal growth factor receptor (EGFR) gene is responsible for cancer progression (Ota et al., 2015). Although CT can marginally extend the life span of individuals with advanced cases, recent progress in immunotherapy, particularly the targeting of the PD-1/PD-L1 interaction, has resulted in better survival rates when used alone or in conjunction with CT. Nevertheless, numerous patients do not respond to these treatments or eventually encounter disease progression, underscoring the need for supplementary immunotherapies that can be combined with CT (Choudhury et al., 2008; Juergens and Brahmer, 2007; Rizvi et al., 2015; Till et al., 2008). Zhao et al. (2019) investigated a novel approach to clinical trials called a prospective patient preference-based study.
The design of this study involves categorizing patients with similar characteristics into treatment groups based on their personal preferences. This was done after thoroughly discussing and comprehending all the therapeutic options with the researchers. Zhao et al. compared the efficacy of the combination of DC-CIK and CT drugs (either docetaxel or pemetrexed) with DC-CIK alone or CT. This study indicated a noticeable improvement in the 1-year progression-free survival (PFS) and OS among the combination groups than monotherapy groups (either CT or immunotherapy), which underscores the superior effectiveness of the combination of DC-CIK with other applications. PFS is the length of time from the beginning of treatment until the occurrence of the first event, which could be the progression of the disease, death, or the diagnosis of a second cancer, whichever happens first.
Regarding the therapeutic potential of CIK combination with CT, a review conducted by Wang et al. (2014a) discovered that among 1,172 patients with advanced metastatic lung cancer, those who received CIK treatment along with CT had a longer median survival time, better PFS, and a higher rate of disease control compared with those who did not receive CT. In addition, patients with higher levels of CD3+ T cells, CD4+ T cells, NK cells, and CD4+/CD8+ ratio in their peripheral blood showed an improved 3-year OS. These experiments approved the higher efficacy of CIK with CT, but, currently, there is only one clinical trial (NCT01902875) that has examined the effectiveness of combining CIK therapy with paclitaxel + cisplatin in NSCLC patients. The most recent update for this trial was on July 18, 2013, and the current status is unknown.
As previously stated, ICIs have shown promising outcomes by inhibiting the communication between tumors and immune cells. It is evident that researchers have taken a keen interest in ICI therapy, as there are currently more than 600 ongoing clinical trials involving NSCLC patients. With respect to the combination of CIK with ICI, six studies' (with PD-1) status is unknown. In some studies, including those by Hellmann et al. (2019), the response rate to PD-1 blocking antibody alone was 15%–20% in NSCLC. Therefore, combination therapy is required to enhance the curative impacts of ICI. In a retrospective study conducted by Han et al. (2021), the effectiveness of PD-1 blocking antibodies, namely pembrolizumab or nivolumab in combination with CIK, was examined.
The results showed that this treatment approach reversed resistance to the anti-PD-1 pathway by elevating the levels of CD3+CD56+CD16+ T cells. In addition, this therapy was well-tolerated by patients, with no signs of toxicity observed. Another study that approved the efficacy of CIK-PD-L1 combination therapy was conducted by Li et al. The combination of CIK cells with crizotinib and nivolumab can boost the immune response against tumors by activating FasL, which results in higher levels of IFN-γ and granzyme B (Li et al., 2022). Moreover, Wang et al. (2018) found that CIK cells release large quantities of IFN-γ. This not only increases the number of T lymphocytes in the tumor microenvironment but also helps existing T cells infiltrating the tumor to function better. By doing so, it overcomes immune escape mechanisms such as MHC downregulation, ultimately tipping the scales in favor of an antitumor response in the tumor microenvironment.
Further research is needed to determine the effectiveness of CAR-T cells combined with CIK therapy in treating NSCLC as there are currently no data available to evaluate this treatment approach. While studies suggest that CAR-T cells may have potential in NSCLC patients, Hung et al. (2020) found that CIK cells are more effective in fighting tumors and have fewer negative side effects than CAR-T cells in NSCLC. However, additional clinical research is necessary to confirm the clinical efficacy of both types of cellular immunotherapy.
Gastric cancer
Gastric cancer (GC) is a commonly occurring and highly fatal malignancy worldwide, ranking third in fatality rates after lung cancer and liver cancer. Unfortunately, the majority of patients are diagnosed at an advanced stage, missing out on potential treatments such as surgery and CT. However, there is hope in the application of immunotherapy for GC patients, as they have shown great sensitivity to ICIs such as nivolumab and pembrolizumab (Fuchs et al., 2018). Similarly, in the case of clinical curative effects of DC-CIK in patients with GC, a meta-analysis was conducted to evaluate the 1-, 2-, 3-, and 5-year OS rates among 318 patients receiving DC-CIK therapy compared with the 369 patients receiving traditional treatment. Remarkably, the OS rates were significantly higher in the DC-CIK group compared with those receiving conventional treatment (P = 0.03).
In addition, the study examined the proportions of CD4+ and CD8+ cells and found that patients treated with DC-CIK had a higher proportion of CD4+ cells, while the control group had a higher proportion of CD8+ cells (Liu et al., 2015). Gao et al. (2014) found the levels of IL-2, IL-6, and IL-10 slightly enhanced, with no statistical significance in the sera of GC and colorectal cancer (CRC) patients. However, serum IL-12 and IFN-γ levels were significantly increased in both GC and CRC patients, indicating that DC/CIK therapy may specifically promote a Th1 immune response to mediate the tumor-killing effect of DC/CIK therapy.
CT provides promising results in patients with GC who are diagnosed in an early stage. Otherwise, there is no opportunity for treatment as long as patients receive CT or other strategies alone. Meantime, evaluating the combination therapy of CT with DC-CIK in advanced gastric cancer (AGC) patients conducted by Qiao in March 2019, enhanced PFS and OS with tolerable toxicities were revealed. Precisely, in this experiment, a decrease in the frequency and number of mutations in circulating tumor DNA (ctDNA) in a majority of patients after receiving DC-CIK infusions was observed. The results of this study indicate that a decrease in ctDNA mutational frequency and the restoration of the T cell receptor repertoire are linked to improved PFS and OS in patients with AGC who underwent DC-CIK therapy.
These findings seem reasonable to suggest that changes in ctDNA could potentially be used as an indicator of the effectiveness of DC-CIK therapy in AGC patients (Qiao et al., 2019).
The use of immunotherapy, specifically anti-PD-1 treatment, may offer some improvement in survival rates for patients with AGC. This treatment has shown potential in extending OS at the 12- and 18-month marks, as well as prolonging the duration of response to treatment (Kono et al., 2020). Theoretically, CIK has more cytotoxicity impacts on GC than ICP and CAR-T cells with higher efficacy and lower toxicity, but the combined treatment of DC-CIK with either ICI or CAR-T cells has not been investigated yet.
Hepatocellular carcinoma
Hepatocellular carcinoma (HCC) is a highly prevalent cancer with a high mortality rate worldwide. The occurrence of HCC is influenced by factors, such as gender and geographical location. The development of HCC is primarily attributed to infections caused by hepatitis B or C viruses, as well as liver damage resulting from alcohol consumption. Various potential treatment approaches for HCC exist, such as liver resection or transplantation, as well as radiofrequency ablation. What is more, several reports have found a correlation between HCC with chronic inflammation-induced cancer, invasion, progression, and recurrence (Zhang et al., 2018). Adoptive cell therapy, such as ICI, CAR-T cells, and CIK therapy, has been extensively used to mitigate or cure patients with HCC.
Meantime, in an experiment (Takayama et al., 2000), 150 patients with HCC were randomly assigned to receive DC-CIK or no adjuvant treatment. The patients who received DC-CIK immunotherapy did not experience hazardous adverse effects, had a longer time to first recurrence, and the recurrence rate of HCC was significantly lower compared with the control group (45%–57%, P = 0.01). However, the OS between the two groups was not a considerable difference (P = 0.09). Another study in which the safety and therapeutic feasibility of DC-CIK in patients with HCC was conducted by Cao with a lower recurrence rate in comparison with the control group (Cao et al., 2019).
The interaction between PD-1/PD-L1 in HCC was approved by many reports, in which the high risk of both cancer metastasis and tumor relapse is expected (Gao et al., 2009; Zeng et al., 2011). As already mentioned, the patients who were treated with DC-CIK experienced a longer time to first tumor recurrence than the current treatment-received group; Zhang et al. (2018) found that HCC patients with high levels of PD-L1 expression receiving postoperative transcather arterial chemoembolization (POTACE) treatment experienced shorter periods of relapse-free survival and OS. In this study, in HCC patients with hepatitis B virus (HBV) infection who received POTACE treatment, DC-CIK cell therapy was found to be beneficial in extending OS. Also, the report indicates that using a PD-1 inhibitor to block the PD-1/PD-L1 axis in DC-CIK cells before infusion could be an effective therapeutic approach for treating HCC, potentially improving OS (Zhang et al., 2019).
Hence, it is urgent to consider the combination therapy of ICI, as well as CAR-T cells, with DC-CIK in patients with HCC.
Renal cell carcinoma
Early detection is crucial in the treatment of renal cell carcinoma (RCC), a type of cancer with the highest mortality rate among genitourinary cancers. Although surgical treatment is possible and recurrence is rare in most patients, the prevalence of RCC has increased over time. Interestingly enough, RCC sufferers after receiving DC-CIK had a higher rate of complete and partial remission, as well as 1- and 3-year survival compared with other therapeutic applications (P < 0.0001) (Wang et al., 2014d). In one study where 385 patients with RCC were examined after receiving DC-CIK revealed that a greater number of these patients experienced both complete and partial remission (P < 0.0001). In addition, more patients who underwent DC-CIK treatment achieved 1- and 3-year survival rates compared with those who did not receive this treatment.
DC-CIK therapeutic application enhances the quality of patient's lives and extends disease-free survival (DFS) in a variety of cancer diseases in terms of RCC sufferers, the median OS was longer, 28 months, than the control group, 11 months (Zhao et al., 2015). The use of autologous tumor lysate-pulsed DCs cocultured with CIK (Ag-DC-CIK) immunotherapy significantly reduced the risk of disease progression and relapse after surgery (P = 0.0418) and the 3-year DFS rate was 96.7%, whereas it was only 57.7% in the control group (Wang et al., 2015).
Moreover, in patients with metastatic RCC (mRCC), the efficacy of antiangiogenic drugs, such as axitinib, has been approved, but the survival rate of patients has reached a stable level and is not improving further. The curative impacts of a combination of axitinib with DC-CIK, as well as the ICI drug, pembrolizumab, in metastatic patients was reported in 2021 by Song et al. (2021). The effectiveness of ICIs in treating mRCC has been established, particularly when used in conjunction with DC-CIK therapy. However, previous study has been limited by the absence of a control group for comparison. Despite this limitation, the combination of axitinib, pembrolizumab, and DC-CIK has shown promising results in advanced RCC, prompting researchers to pursue further investigation and experimentation.
Also, another report discussing the combining of adoptive cell therapy with immunotherapy was conducted by Yuan et al. (2019) to assess the therapeutic effects of DC-CIK, anti-CTLA-4, and anti-PD-1 in advanced RCC. Yuan et al. demonstrated that the use of CAR-T cells and ICIs effectively inhibits the immune evasion mechanisms used by tumor cells, thereby augmenting the therapeutic property of DC-D-CIK therapy in killing tumor cells. Consequently, similar to other types of tumors, further studies are required to prolong the survival of patients with RCC. Zhang et al. (2020) carried out another study, which examined the effectiveness of CIK cell treatment in RCC patients.
Breast cancer
BC continues to be a major contributor to women's mortality from cancer, primarily due to its diverse nature, ability to spread, and resistance to treatment. To date, with respect to clinical trials, four out of seven studies' status has been completed: NCT02418481, NCT02450357, NCT01395056, and NCT01232062. In a 2014 study, it was found that patients who received DC-CIK had a significantly higher 1-year OS rate compared with those who received CIK alone or DC alone. Furthermore, various immune cells and cytokines in the peripheral blood, such as CD3+ T cells, CD4+ T cells, CD8+ T cells, NK T cells (CD56+ CD16+ cells), IL-2, IL-12, TNF-α, and IFN-γ, were much higher in the DC-CIK group compared with the other groups (Wang et al., 2014c).
In this article, there is a correlation between CT drugs and the level of T helper cells, as it was observed that receiving CT decreased the presence of these cells. Nevertheless, the combination of DC-CIK therapy with CT resulted in a notable rise in T helper1 cells within the treatment group. This increase in T helper1 cells played a crucial role in enhancing the immune response against cancer cells and ultimately improving the effectiveness of tumor suppression (Lin et al., 2017). In the advanced BC patients, the use of DC-CIK treatment showed a potential improvement in the 3- and 5-year OS rate compared with the non-DC-CIK group. Although the improvement did not reach statistical significance (P = 0.051), the 5-year OS rate still increased from 22.72% to 41.56% (Xie et al., 2019).
In terms of clinical aggression, triple-negative breast cancer (TNBC), which lacks overexpression of the human EGFR2 and the estrogen, progesterone, and hormone receptors, is the most common form of BC, accounting for 10%–17% of all cases. DC-CIK combined with CT drugs may have synergistic effects on tumor cells and Wang et al. (2016) approved the therapeutic application of cyclophosphamide, thiotepa, and carboplatin with DC-CIK in younger than 45 years of metastatic TNBC patients. The limited use of ICIs in treating BC has primarily been focused on TNBC, possibly due to the higher infiltration of T cells in TNBC tumors.
However, it is important to note that there have been no studies conducted on the combination of ICI or CAR-T cells and DC-D-CIK in patients with BC. This is a significant gap in research that should not be overlooked, and further studies should be conducted as it has shown promising results in other types of cancer.
Ovarian cancer
Ovarian cancer stem cells (OCSCs) are a type of cancer cells that have shown resistance to current cancer treatments. These cells have been found to be associated with metastasis and recurrence in ovarian cancer (OC), a highly malignant gynecological cancer that poses a significant threat to women's health. In recent years, there has been an increase in the incidence of OC in younger patients, along with an increase in its malignancy. Several studies have identified a subpopulation of cells in OC tissue samples that resemble embryonic stem cells and express high levels of CD44, CD133, and c-Kit (CD117) markers. These cells possess stem cell-like characteristics, such as self-renewal ability, but also exhibit the aggressive features of cancer cells, including high proliferation, invasiveness, and tumorigenicity. Hence, they are referred to as OCSCs (Ffrench et al., 2014).
Qin made an unexpected finding that OCSCs obtained from OC patients exhibited extremely high levels of TNFR1 on their cell surface. This discovery provided a clear explanation for how DC-CIK cells were able to effectively eliminate OCSCs. When TNFR1 expression was eliminated in OCSCs, the effectiveness of DC-CIK cell therapy in killing OCSCs significantly decreased, and the OCSCs displayed increased abilities in proliferation, invasion, and tumor formation. As a result, this study concluded that TNFR1 expression plays a crucial role in determining the efficacy of DC-CIK immunotherapy in eliminating OCSCs (Qin et al., 2018). Surprisingly, previous reports on the effectiveness of combining CT with DC-CIK cell therapy in OC patients have been limited. However, Gao et al. (2021) conducted a study and found that this treatment approach significantly improved OS in advanced OC cases.
Furthermore, the DC-CIK group showed significantly higher percentages of CD3+ T lymphocytes, CD3+ CD4+ T lymphocytes, and NK cells, as well as a higher CD4/CD8 ratio, compared with the CT group. Conversely, the proportion of CD4+ CD25+ T lymphocytes was significantly lower in the DC-CIK group compared with the CT group. Overall, these findings highlight the potential of combining DC-CIK cell therapy with CT as a promising treatment option for advanced OC patients. Further research is needed to validate these results and explore the underlying mechanisms of this treatment approach.
CRC and colon cancer
CRC ranks as the third-most frequently detected cancer in people. In recent times, there has been a noticeable rise in colon cancer cases, particularly in the Eastern world, due to changes in dietary patterns. While surgical removal is the primary treatment option globally, CT, radiation therapy, or a combination of both can also effectively treat CRC and enhance patient survival rates. Nevertheless, it is disheartening to note that 25% of individuals diagnosed with advanced-stage cancer have a mere 10% chance of surviving for 5 years. Researchers worldwide have shown great interest in immunotherapy for CRC, as it has demonstrated the ability to effectively eliminate tumors and improve long-term survival rates. In the context of DC-CIK therapy for colorectal patients, although there is limited research assessing its clinical effectiveness, the available reports have shown promising outcomes.
Several clinical trials have investigated the use of DC-CIK therapy in colon cancer patients, and the results indicate that combining this immunotherapy with CT significantly enhances OS rates. For example, one study revealed a 1-year OS rate of 93% for colon cancer patients who underwent DC-CIK immunotherapy alongside CT, compared with only 84% for those who did not receive DC-CIK treatment. Similarly, the 2-year OS rate was 76% for the DC-CIK and CT group, while it was 69% for the control group. In addition, the 3-year OS rate was 80% for the combination therapy group, whereas it was only 61% for the CT-only group.
These consistent findings from multiple trials demonstrate that patients who receive DC-CIK immunotherapy combined with CT experience improved survival outcomes. Moreover, the combination therapy also resulted in an 86% DFS rate at 1 year for colon cancer patients, compared with only 63% for those who received CT alone. Figure 2 shows the possible pathways to enhance the therapeutic potential of CIK to eradicate tumor cells. Trials in Table 1 also showed a longer DFS period in the DC-CIK and CT group compared with the CT-only group within the first year (Cai et al., 2010; Li et al., 2012; Wei et al., 2009; Ying et al., 2010; Zhang et al., 2011; Zhu et al., 2011). A comprehensive analysis conducted by Wang et al. (2014b) confirmed that DC-CIK treatment resulted in improved clinical responses among colon patients. Furthermore, combining DC-CIK therapy with CT drugs has been found to enhance patients' quality of life
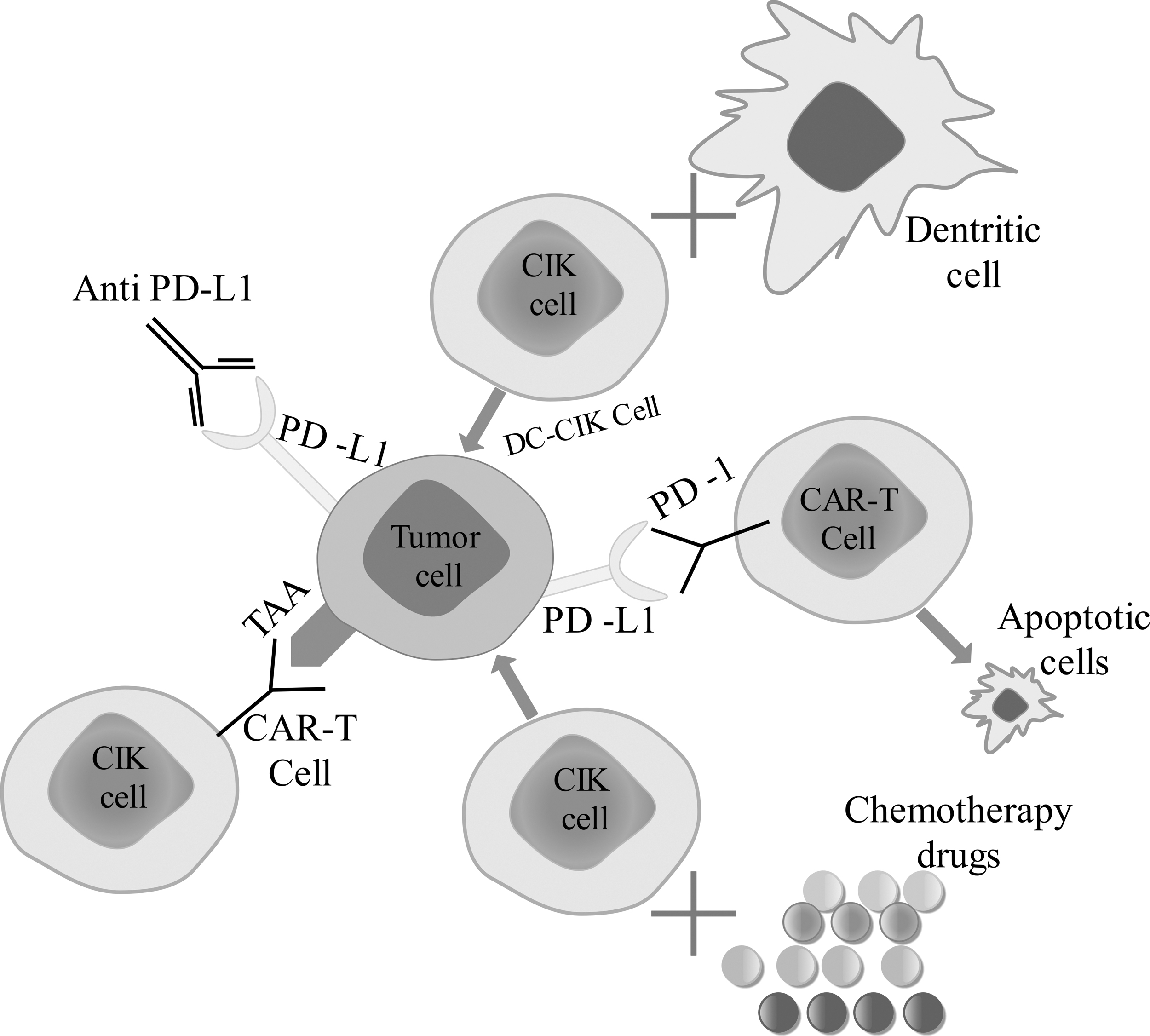
A diagram depicted the enhanced CIK treatment approach. The enhanced CIK treatment approach involves combining CIK with other therapeutic applications to increase their effectiveness while minimizing toxicity. For instance, CAR-T cells, which express ICP on their surface, can bind with ligands such as PD-L1 on tumor cells, leading to CAR-T cell apoptosis. By binding with ICIs, the chances of connecting with TAA are increased; therefore, CAR-T cells in combination with anti-immune checkpoint monoclonal antibody are able to kill tumor cells. This means that combination therapy, such as DC-CIK-CAR-T cells, may have a greater antitumor activity compared with individual treatments. In addition, combining CIK with CT and immune checkpoints is recommended for various types of cancer. CAR, chimeric antigen receptor; CT, chemotherapy; ICIs, immune checkpoint inhibitors; TAA, tumor-associated antigens.
A Summary of Clinical Study Details in Cancer Diseases
BC, breast cancer; CC, colon cancer; CIK, cytokine-induced killer; CRC, colorectal cancer; DC, dendritic cell; FCM, flow cytometry; GC, gastric cancer; HCC, hepatocellular carcinoma; NSCLC, nonsmall cell lung cancer; OC, ovarian cancer; PC, pancreatic cancer; RC, renal carcinoma; RT-PCR, real-time polymerase chain reaction.
Others
Contrary to other commonly used clinical treatments such as ICI, CAR-T cell therapy, vaccines, and CT, there is a surprisingly limited amount of research and reports on the use of DC-CIK therapy in cancer treatment. Furthermore, aside from the tumors previously mentioned, DC-CIK treatment has also been investigated in the context of glioblastoma, pancreatic cancer (PC), and prostate cancer. However, clinical trials of combination therapy with other applications, including CAR-T cells or ICIs, are still present in these patients.
Glioblastoma is a highly aggressive and prevalent primary malignant brain tumor in adults, with uncertain risk factors and a typically fatal clinical outcome. A phase III clinical trial conducted by Kong et al. (2017) found that combining DC-CIK immunotherapy with temozolomide led to a notable increase in the median PFS for patients with glioblastoma. The CIK immunotherapy group had a median PFS of 8.1 months, whereas the control group had a median PFS of 5.4 months. The CIK immunotherapy group also had higher PFS rates at 1 and 2 years compared with the control group. Furthermore, the CIK immunotherapy group had a longer median OS of 22.5 months, while the control group had a median OS of 16.9 months. The disease control rate between the two groups was significantly different, even though there was no significant difference in the total response rate between the groups.
PC is a difficult disease to treat, with a rising incidence and limited improvement in mortality rates. It is anticipated that by 2030, it will rank as the second-most common reason for cancer-related death. While surgery and adjuvant CT can lead to long-term survival, this is only possible for a small percentage of patients with PC that can be surgically removed. Chen and Zhang (2016) reviewed eleven clinical studies that examined the effects of DC-CIK therapy on patients with PC at different time points (1, 1.5, and 2 years). The results showed that this form of immunotherapy significantly prolonged the OS of patients compared with those who did not receive immunotherapy.
A prospective study (Clinical Trial No.: NCT01781520) was carried out to evaluate the effectiveness of combining DC-CIK therapy with the CT drug S-1 in individuals older than 18 years who were diagnosed with advanced PC (Jiang et al., 2017). To evaluate the prognosis and response to treatment in gastrointestinal cancers, clinical trials commonly use CA199, CA125, CA153, and CEA as indicators. Among these, CA199 is widely recognized as a prominent marker for PC (Wang and Tian, 2014). Meantime, Jiang et al. (2017) observed that the DC-CIK plus S1 group exhibited the highest percentage of patients with decreased levels of CEA and CA-199, which correlated with improved outcomes compared with the other groups. The addition of DC-CIK therapy to S-1 significantly extended OS and PFS compared with either treatment alone, without causing additional toxicity compared with CT alone.
Notably, the greatest benefits in terms of OS and PFS were seen in patients who received two or more cycles of DC-CIK treatment.
Prostate cancer is a type of cancer that affects men and is a major cause of death among males worldwide. Patients with prostate cancer can have either a localized or advanced form of the disease. Despite a 40% decrease in mortality over the past two decades, prostate cancer continues to be the most commonly diagnosed cancer and the sixth leading cause of cancer-related deaths in men globally. In a study published in 2020, Wang et al. (2020) assessed the safety and effectiveness of DC-CIK treatment in four immortalized prostatic epithelial cell lines (BPH-1) and four human prostate cancer cell lines, namely LNCaP, 22Rv1, VCaP, and DU145. This work validated the immunogenic peptide-sensitized DC-CIK cell's antiprostate cancer actions in vitro.
According to Wang's research, primary and metastatic prostate cancer has a markedly higher prevalence of the glycoprotein EpCAM than normal and benign hyperplastic prostates. This suggests that using CIK-based immunotherapy to target EpCAM+ and CD44+ prostate cancer stem cells, or PCSCs, may be a promising treatment strategy. In addition, another study suggests that DC-CIK-based immunotherapy is effective in inhibiting the advancement of prostate cancer (Xu et al., 2015). However, further research and experimentation are needed to evaluate the therapeutic effects of DC-CIK alone and in combination with other treatments in prostate cancer patients. For instance, Deng et al. (2015) demonstrated the cytotoxic effects of CAR-T-based therapy targeting EpCAM in their study. Nevertheless, clinical trials involving DC-CIK and CAR-T cells have not been conducted thus far.
Hematological malignancies
Despite the significant benefits observed in patients with hematological malignancies treated with CIK cells, such as prolonged survival and improved quality of life, there is still a need to determine the most effective application schedule for their clinical use. Studies have shown that in many cases, CIK cell therapy can improve immunological parameters (such as immune function), decrease tumor markers (substances produced by cancer cells), and reduce inflammation in cancer patients. However, some studies have suggested that CIK cell therapy may not be as effective in treating hematological neoplasms, such as acute myeloid leukemia (AML). AML patients were shown to benefit least from this type of therapy (Schmeel et al., 2014).
Several clinical trials have been conducted to evaluate the efficacy of CIK cell therapy in different cancer types. One study evaluated the effectiveness of CIK cell therapy followed by CT in 41 patients with acute leukemia (Jiang et al., 2005). The results showed that CIK cell treatment before CT did not significantly improve the overall response rate or survival compared with CT alone. Another study enrolled six patients suffering from advanced lymphomas in a pilot phase I trial (Olioso et al., 2009). Only one patient achieved and sustained complete remission, while the remaining patients did not respond to CIK cells at all. However, no severe adverse effects were observed. In a phase I trial involving 20 patients with various types of cancer, including AML, positive immunologic effects were observed after CIK cell infusions combined with subcutaneous injections of IL-2. However, three patients developed mild symptoms that disappeared after symptomatic treatment.
The researchers have developed a new method to modify CIK cells by introducing CD33.CAR and CXCR4, enhancing their ability to migrate toward cancer cells and to kill them (Biondi et al., 2023). The CXCR4 protein is overexpressed in these modified CIK cells, which makes them more responsive to the chemokine CXCL12, a molecule that attracts immune cells to the tumor site. The CD33.CAR protein is a chimeric antigen receptor that recognizes a protein called CD33, which is present on the surface of many leukemia cells, including leukemia stem cells (LSCs). This approach is particularly relevant for AML, a type of blood cancer in which CAR-T cell therapy has shown limited efficacy due to difficulties in targeting LSCs that reside in the bone marrow.
By modifying CIK cells with CD33.CAR and CXCR4, the researchers aim to improve their homing to the bone marrow and increase their contact with leukemia cells, including LSCs, leading to a more effective elimination of the cancer cells. The study also tested the modified CIK cells on CD33+ cell lines and primary AML cells, demonstrating their potential as a treatment option for this challenging cancer. The clinical trials of CIK therapy in hematological malignancies are given in Table 2.
Clinical Trials of CIK in Hematological Malignancies
Conclusion
As we summarized the therapeutic potential of DC-CIK in cancer diseases, it is urgent to conduct more study and experiment to assess its safety and impacts. However, we need to consider various aspects of using DC-CIK therapy to enhance tumor response, such as the treatment cycle and combination therapy. DC-CIK therapy not only has beneficial effects that lead to longer OS, but it also has the ability to modulate the proportions of T cell subpopulations. Specifically, it can regulate Treg cells, which contribute to tumor recurrence and immune suppression by releasing inhibitory cytokines such as IL-10 and transforming growth factor-β1. Several studies have shown an increased presence of CD4+ CD25+ regulatory T cells in patients with NSCLC, HCC, and GC, which supports these findings (Yu et al., 2017).
Furthermore, Song et al. (2017) demonstrated a direct relationship between the administration of multiple cycles (specifically three cycles) of DC/CIK cell immunotherapy and a decrease in Treg cell count, resulting in enhanced tumor cytotoxicity in individuals with NSCLC. Patients who underwent three or more cycles of DC-CIK therapy exhibited a lower recurrence rate compared with the control group (Song et al., 2017).
In recent years, significant advancements in tumor immunology and molecular biology have led to the emergence of more promising treatment options for cancer. These new approaches show great potential in enhancing patient outcomes and prognosis. In other words, the combination of DC-CIK therapy with other treatments, such as CT, CAR-T cells, and ICIs, has been shown to have synergistic effects. However, each approach has its limitations, such as T cell infiltration issues with CAR-T cells and off-tumor side effects with ICIs. Therefore, combining these therapies appears to be the most effective strategy for maximizing their therapeutic benefits. However, there is a lack of experiments evaluating combination therapy in different types of cancer and studying its limitations. At the moment, clinical trials of DC-CIK therapy in certain cancer types, such as osteosarcoma, melanoma, and soft tumors, are currently lacking and should not be overlooked.
In summary, the ability of CIK cells to effectively target various types of tumors without being limited by MHC molecules is a significant attribute. In addition, CIK cells are known for their manageable and comparatively lower levels of toxicity. While DC-CIK therapy has shown improved quality of life and increased OS in cancer patients, as well as reduced tumor recurrence, there is limited research on its effectiveness when used alone or in combination with other treatments. Therefore, further studies are needed to investigate its antitumor potential.
Footnotes
Acknowledgment
The authors apologize that because of space constraints they were unable to cite many studies.
Authors' Contributions
S.Z.: Conceptualization and software.
Y.Z.: Methodology and writing—original draft preparation.
X.L.: Supervision, validation, revision, and project administration.
V.M.: writing—original draft preparation and language review.
Availability of Data and Materials
The data sets used in this study are available upon reasonable request.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.