
Abstract
The study of sensitive and specific biomarkers, such as blood inflammatory cytokines, could provide an answer to the challenges faced in the differential diagnosis of patients with systemic inflammation. Limited data exist on the impact of age on serum levels of inflammatory cytokines. We collected serum samples of 42 healthy children and young adults (1 month to 21 years). Serum levels of interleukin 1 receptor antagonist (IL-1Ra), IL-1β, IL-6, IL-18, tumor necrosis factor-alpha (TNF-α), CXCL9, and CXCL10 were measured. Data were analyzed for three different age groups (<6, 6–17, and 18–21 years). IL-18, TNF-α, and CXCL9 values varied significantly according to age group. Median values of IL-18 and TNF-α decline with age, whereas CXCL9 and CXCL10 are lowest at 6–17 years. IL-1Ra is stable among age groups. In the majority of cases, IL-1β and IL-6 are not measurable above the lower limit of quantification. A scoping literature review revealed highly variable data on IL-1Ra, IL-18, TNF-α, and CXCL10. For CXCL9, pediatric reference data are scarce. In conclusion, we report an age-dependent signature of multiple inflammatory cytokines measured in the serum of healthy children and young adults, suggesting the need to use age-specific reference values in future pediatric studies.
Introduction
Several human diseases exhibit features of recurrent, chronic, or severe systemic inflammation. Patients experiencing such symptoms may be labeled with auto-inflammatory, auto-immune, or hyperinflammatory diseases. Despite some clinical similarities and common elevated inflammatory parameters, such as sedimentation rate, C-reactive protein, and leukocytosis, these disorders comprise distinct pathophysiology and management strategies. Distinguishing these diseases is pivotal, as early diagnosis and targeted treatment results in decreased morbidity, mortality, and health care costs.
Identifying biomarkers in blood samples that are sensitive or specific for certain diseases may tackle some of these challenges in diagnostics and categorize patients with systemic inflammatory features within clinical entities and/or differentiate them from patients having infectious or malignant diseases. In this respect, blood cytokine profiling is increasingly used in an attempt to accelerate diagnosis and improve patient management in diseases with systemic inflammation. Limited data reveal correlations of elevated cytokine levels in the blood of patients with specific diseases, such as systemic juvenile idiopathic arthritis or different hereditary fever syndromes (for example, familial Mediterranean fever and cryopyrin-associated periodic syndromes). (Broderick and Hoffman, 2020; Feng et al., 2018; Ibrahim et al., 2017; Koga et al., 2016b).
In order to assess biomarker cutoffs for disease, solid reference values measured in physiological conditions are necessary (Kleiner et al., 2013a). So far, no universal reference values for inflammatory cytokines in healthy controls are available. Especially in the pediatric population, reference values are particularly scarce (Kleiner et al., 2013a; Wu et al., 2017). In addition, this process is hampered because measurements of inflammatory cytokines tend to be nonstandardized and thus often assay dependent. Therefore, the comparability between settings remains an issue (Hennø et al., 2017). To address these challenges, we optimized reference values for a panel of inflammatory cytokines (interleukin 1 receptor antagonist [IL-1Ra], IL-1β, IL-6, IL-18, tumor necrosis factor-alpha [TNF-α], chemokine (C-X-C motif) ligand 9 [CXCL9], and CXCL10) in pediatric healthy controls divided into three age groups, using a multiplex immunoassay.
Materials and Methods
Recruitment of healthy volunteers
Healthy children and young adults (≤21 years) admitted for skin prick tests or surgical procedures (such as minor orthopedic surgery or circumcision) at the Ghent University Hospital were included. Except their reason for admission in the hospital, patients fulfilled all requirements as being healthy. We defined this as follows: no signs of inflammation at the time of, or in the two weeks prior to blood sampling with no signs of acute or chronic infection, no recent vaccination, no ingestion of drugs influencing the immune system, no known underlying disease, or any other clinically significant disorder. Written informed consent for additional blood sampling during routine venipuncture was obtained from patients or the parents of all children, and assent was obtained in children 12 years or older. The research was completed in accordance with the Declaration of Helsinki, and approval of the local ethical committee (Ghent University Hospital Ethics Committee, Ghent, Belgium) was obtained (BC-11141).
Blood sampling and sample processing
One serum sample was obtained from each patient. Serum tubes were collected, transported at room temperature, and centrifuged for 10 min at 2000 g at 4°C within 60 min after collection. Supernatant was aliquoted and stored at −80°C in the Primary Immunodeficiency (PID) biobank at the PID Research Lab. A securely stored file contained pseudonymized data and information on the blood sample. Approval from the local ethical committee was obtained (BB190105).
Cytokine measurements
Levels of IL-1Ra, IL-1β, IL-6, IL-18, TNF-α, CXCL9, and CXCL10 were measured on serum samples by Multi-Analyte Profiling (xMAP) Luminex Technology using a magnetic bead-based immunoassay (Bio-Rad consumables) according to manufacturer’s protocol. Undetectable values were quantified as lower limit of quantification (LLOQ) as reported by the software. Data were obtained using a Bio-Plex 200 reader and analyzed using the Bio-Plex Manager Software (v6).
Data analysis
Statistical analysis was performed using SPSS version 29.0. To ensure that cytokine values were within range to be considered healthy, principle component analysis was performed using GraphPad Prism (v8). Reference values of cytokine levels were presented as median and interquartile range according to age groups (<6 years; 6–17 years; 18–21 years) and visualized in boxplots. Kruskal–Wallis testing was performed to identify differences between the different age groups. When significant, post hoc Mann–Whitney U test was performed with Bonferroni correction.
Results
Serum samples from 43 healthy controls, ages ranging from 1 month to 21 years, were analyzed and levels of IL-1Ra, IL-1β, IL-6, IL-18, TNF-α, CXCL9, and CXCL10 were quantified. Principal component analysis (PCA) confirmed minimal heterogeneity among the individual cytokine profiles (Fig. 1). One notable outlier was identified. This concerned a control aged 12 years whose profile was characterized by substantially elevated IL-1b and IL-1Ra. Given its clear differential profile from other individuals, we concluded that this case could not be considered as healthy at the time of sampling and was excluded from further analysis. Apart from some of the youngest individuals, other healthy controls had largely overlapping positions in the first two principal components.
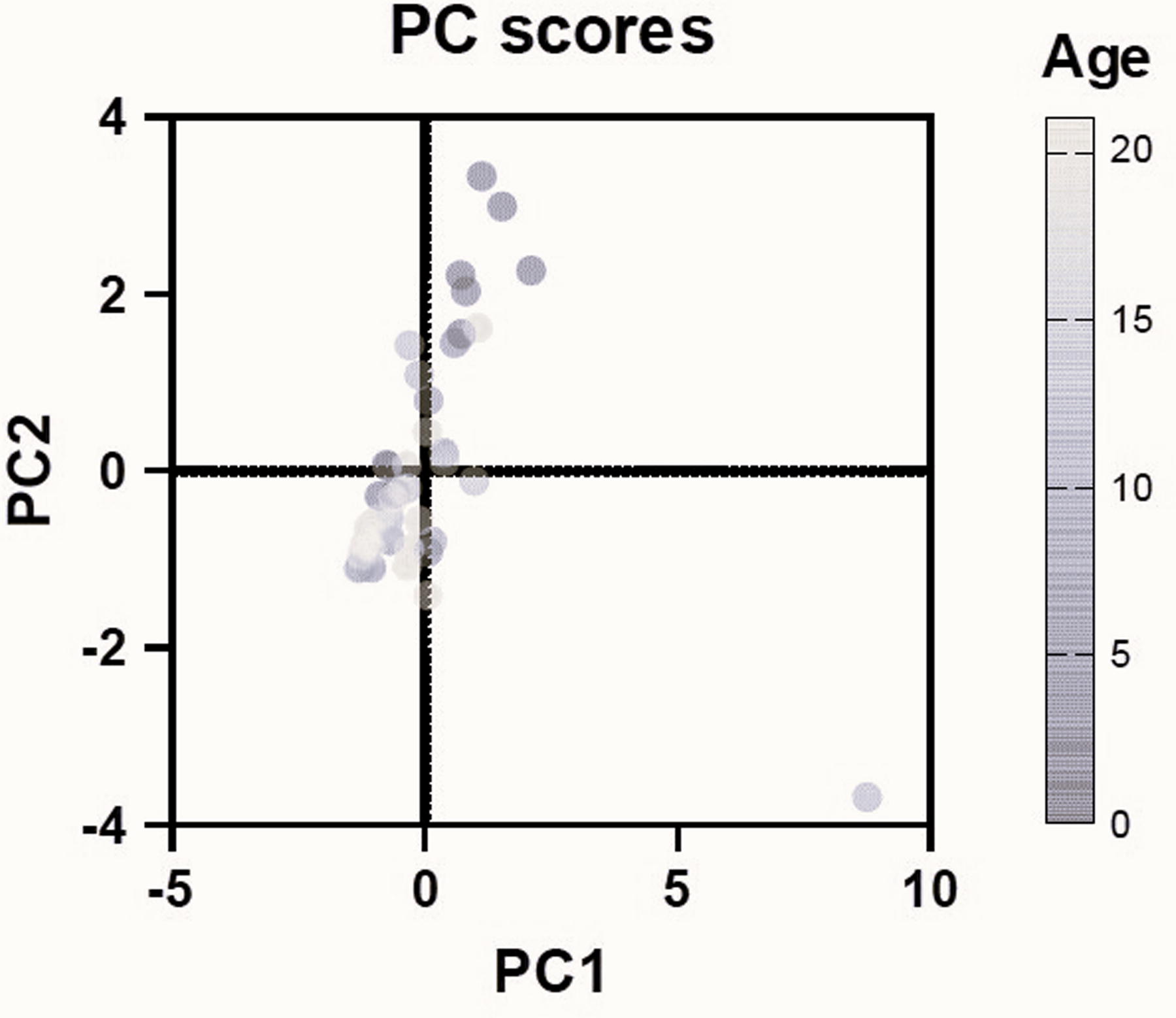
First two components of PCA using all measured inflammatory cytokines as inputs and revealing one outlying sample. Individual samples are color-coded depending on the age of the healthy control at the moment of sampling. PCA, principal component analysis.
The PCA suggested that the healthy controls could be divided into three numerically balanced age groups: <6 years (n = 13), 6–17 years (n = 14), and 18–21 years (n = 15) (Table 1). More males than females were recruited in the youngest age group (10/13), whereas the opposite was true for the oldest category (10/15 females). In controls <6 years, there was bias toward patients younger than 1 year of age (1–7 months old).
Demographic Characterization of the Cohort of Healthy Individuals
Based on the principal component analysis one outlier was omitted from the dataset.
IQR, interquartile range.
Serum cytokine data were analyzed for each age group (Table 2). For IL-1Ra, no differences between the different age groups were observed (median values 10.43–10.67 pg/mL). In contrast, IL-18, TNF-α, CXCL9, and CXCL10 values varied according to the age group. Median values of IL-18 were declining with age, going from 3.53 pg/mL to 1.09 pg/mL to 0.030 pg/mL in the respective age groups. The same trend was observed for TNF-α, with 17.37 pg/mL, 5.12 pg/mL, and 5.12 pg/mL, respectively. A trend for a “U-shape,” with higher values in the youngest and oldest categories, was observed in the interferon-induced chemokines CXCL9 and CXCL10, giving median values of 21.26 pg/mL and 42.59 pg/mL, respectively, for the youngest, 9.71 pg/mL and 30.78 pg/mL for the middle, and 13.84 pg/mL and 37.86 pg/mL for the oldest age group. IL-1β and IL-6 were mostly not measurable above the LLOQ in all age groups, except for some outliers.
Age-Dependent Signature of Inflammatory Cytokines in Healthy Children and Young Adults.
aLLOQ, lower limit of quantification.
For IL-18, TNF-α, and CXCL9, statistically significant differences between age groups were found (Fig. 2). Values of CXCL9 and TNF-α differed significantly between the youngest and middle age group (P = 0.021 and P = 0.006, respectively), whereas IL-18 and TNF-α differed significantly between the youngest and oldest age groups (P < 0.001 for both). For IL-18, the difference between the youngest and middle age group was not significant after Bonferroni correction (P = 0.064), although scatterplots indicated an overall inverse linear trend between age and IL-18/TNF-α. For IL-1Ra, IL-1β, IL-6, and CXCL10, no significant differences among age groups were found.
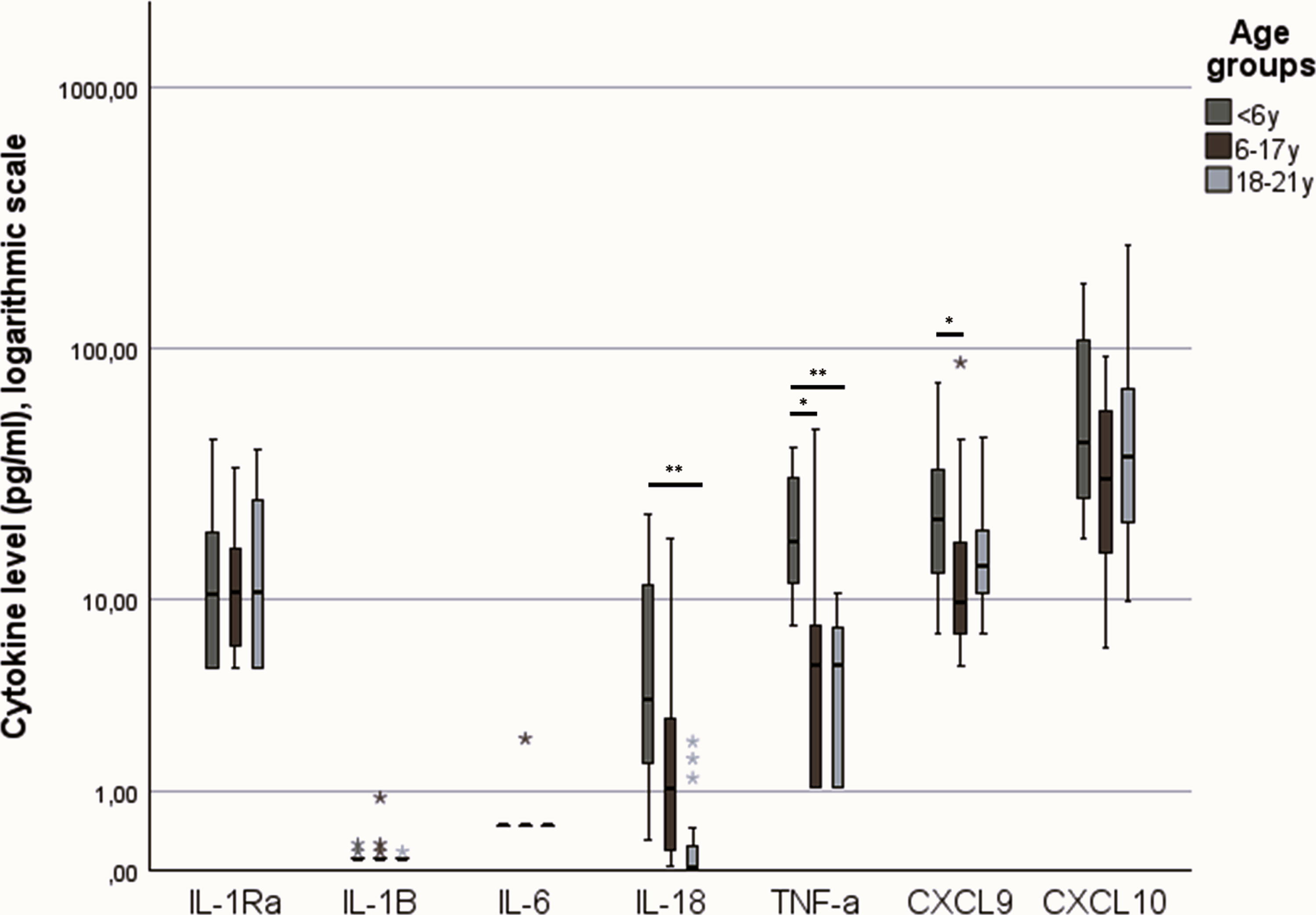
Boxplot displaying cytokine values (on a logarithmic scale) for the different age groups. Outliers were defined as >+2SD.
To assess the clinical validity of our cohort, a scoping literature review was performed to benchmark our findings (Table 3). Few data in literature were available on pediatric inflammatory cytokines reference values. For IL-1Ra, conflicting reference values were reported. Some studies reported higher reference values for IL-1Ra (>100 pg/mL) (Biancotto et al., 2013; Decker et al., 2017; Kleiner et al.), whereas others reported a median value in the same range as our analysis (31.51–42.59 pg/mL) (Hennø et al., 2017; Koga et al., 2016a). For CXCL10, in the majority of papers, higher median values were reported (Biancotto et al., 2013; Decker et al., 2017; Hennø et al., 2017; Kleiner et al., 2013a; Koga et al., 2016a). In other cohorts, higher reference values for IL-18 were found, although there was great variation between studies (Almeida de Jesus and Goldbach-Mansky, 2013; Federici and Gattorno, 2014; Ibrahim et al., 2017). For IL-1β, IL-6, and TNF-α, reference values found in the literature are in the same order as our reference values (Almeida de Jesus and Goldbach-Mansky, 2013; Federici and Gattorno, 2014; Hennø et al., 2017; Ibrahim et al., 2017; Koga et al., 2016a). Only limited data were found that specifically reported on pediatric reference values for CXCL9 (Kleiner et al., 2013a). In addition to comparing cytokine profiles with age-specific reference values, it is important to obtain follow-up samples from the same individual because of the potential high variation between individuals (Biancotto et al., 2013).
Reference Values of Inflammatory Cytokines in Healthy Controls—Scoping Literature Review
The authors declare that samples have been stored for 24 h at 37°C.
CBA, cytometric bead array; IQR, interquartile range; LLOD, lower limit of detection; LLOQ, lower limit of quantification; SD, standard deviation; SEM, standard error of the mean.
Discussion
Literature on reference values of cytokines is scarce, especially in the pediatric population. In this work, seven inflammatory cytokines were assessed in a pediatric cohort of healthy controls (n = 42). The number of healthy volunteers and their age distribution allowed for an in-depth analysis and provided insights into maturational differences in cytokine profiles, demonstrating the importance of age-specific references.
By comparing findings with previous reports, we could confirm some of the cytokine signatures that were found in our cohort, including age-dependent differences for IL-18 and TNF-α. Regarding the age-dependent signature for CXCL9 and CXCL10, we hypothesize that young, healthy children have a higher interferon steady state and that there could be hormonal influences during puberty. Of note, the difference is only statistically significant for CXCL9 between the youngest and middle age group in this cohort. First, mounting evidence during the COVID-19 pandemic has shown that there is a higher innate interferon response and steady state in young, healthy children (Yoshida et al., 2022). It has furthermore been observed that these higher type II interferon levels are downregulated during viral infection in early childhood (Savino et al., 2024). This could explain the higher values of CXCL9 and CXCL10 in the youngest age group, as these are interferon-related. Second, there are pubertal influences on systemic inflammation, as shown with CRP, IL-8, and TNF-α (Stumper et al., 2020). We suggest that these maturational effects and hormonal influences also affect CXCL9 and CXCL10 values in the middle age group. Lastly, interferon aging could also contribute to the rising values in (early) adulthood (Cao, 2022). This age-dependent signature of CXCL9 and CXCL10 is also echoed in the cohort of Kleiner et al. and Decker et al., although additional data are scarce (Decker et al., 2017; Kleiner et al., 2013a). Further research to elucidate this age-dependent signature is needed.
Recruitment of pediatric healthy controls remains challenging. There is an ethical objection to perform venipunctures in young children without diagnostic or therapeutical need. Although we had strict inclusion criteria and used a specific questionnaire to avoid children with recent or current inflammation to be included, we identified one outlier with unexpectedly high IL-1β and IL-1Ra. In addition, recruiting very young children is challenging because these children seldom undergo blood sampling which might give some bias toward those that were recruited in the study. As present in our study population, male children younger than one year were recruited more frequently, mainly because of recruitment among children in day clinics undergoing circumcision. As in this age group, a trend for higher levels of IL-18 and TNF-α was found, and further research is necessary to confirm these findings in independent cohorts of infants and toddlers. However, one of the strengths of our study is the inclusion of individuals who are notoriously understudied, in particular infants and young children, and that we were able to draft specific reference values for these age groups.
For this analysis, we used the xMAP Luminex Technology. This technology has advantages compared with enzyme-linked immune sorbent assay (ELISA) as it can quantify multiple analytes simultaneously from small volume samples and at relatively low concentrations. There might be additional advantages as Luminex assays can be time- and cost efficient. However, in some instances, accuracy and sensitivity might be lost when comparing with high-sensitive ELISAs.
Investigators should be aware that preanalytical conditions and sample storage conditions can induce important variability in cytokine research. Previous research has shown that cytokine levels might differ depending on the sample type (serum versus plasma), the time needed to store samples after collection (Friebe and Volk, 2008; Hennø et al., 2017; Skogstrand et al., 2008; Sugden et al., 2015), the number of freeze-thaw cycles (Hennø et al., 2017), the technology used to measure biomarkers (Chowdhury et al., 2009), and that baseline differences exist between individuals (Wu et al., 2017). Cytokines suggested to be most sensitive to those influences are IL-1β, IL-6, and TNF-α, although conflicting evidence exists (Friebe and Volk, 2008; Hennø et al., 2017; Skogstrand et al., 2008; Sugden et al., 2015). Therefore, it is suggested to analyze cytokines only if the sample has been immediately cooled on crushed ice and rapidly centrifuged within 4 h and that no more than three freeze-thaw cycles occur after storage at −80°C.
These observations show that absolute concentrations of blood inflammatory cytokines are not always comparable between cohorts or assays. Additional research will be needed to assess similarities and differences between technologies and experimental settings. This implies that a limitation of our study is that findings might be center- and assay specific.
Commercial multiplex kits use synthetic diluents as surrogate matrix. Although the same diluents are used to generate calibration curves, these do not mirror the complexity of biological matrices. This underlines the importance of in-house controls within the test matrix and that additional data on cytokine levels in the healthy population are highly needed.
Conclusions
In conclusion, we report on an age-dependent signature of multiple inflammatory cytokines measured in the serum of healthy children and young adults, and a cohort of individuals who are frequently understudied. Some reflections are formulated on the validity and comparability of cytokine analysis, aiming to guide future analysis strategies. Future research should always incorporate pediatric-specific reference values when studying children, and—when relevant—use specific age group data, as presented herein.
Footnotes
Acknowledgments
This work was performed in the context of the “Honours Program in Life Sciences, Breaking Frontiers” at Ghent University. The authors are very grateful for this opportunity and thank all the organizers and staff involved.
The authors want to thank the Allergy Network of the Ghent University Hospital (in particular Ms. L. De Groote) and the pediatric day clinic (in particular Ms. E. Tytgat) for welcoming them with a big smile for sample collection on healthy controls. They also thank the Dept. of Urologic Pediatric Surgery, led by Prof. Dr. E. Van Laecke, and Prof. Dr. F. Plasschaert from the Dept. of Orthopedic Pediatric Surgery for helping them collect blood samples of healthy children who underwent surgery.
This work was not possible without the enthusiastic staff of the PID Research Laboratory helping them to coordinate the sample collection and for the practical lab work.
Lastly, the authors also thank all the parents and participants for their contribution to this research.
Authors’ Contributions
M.B. contributed to data curation, formal analysis, investigation, and writing—original draft. R.E.K. contributed to data curation, formal analysis, investigation and writing—original draft. L.H. contributed to formal analysis, investigation and writing—review and editing. B.M. contributed to investigation and writing—review and editing. S.T. contributed to investigation and writing—review and editing. K.C. contributed to investigation, project administration, and resources. V.D.B. contributed to investigation, project administration, and resources. J.D. contributed to conceptualization, supervision and writing—review and editing. F.H. contributed to conceptualization, funding acquisition, supervision and writing—review and editing.
Author Disclosure Statement
The authors do not report any conflicts of interest.
Funding Information
FWO TBM project (T004721N) “FEBRIS: Flemish joint Effort for Biomarker pRofiling in Inflammatory Systemic diseases.”