
Abstract
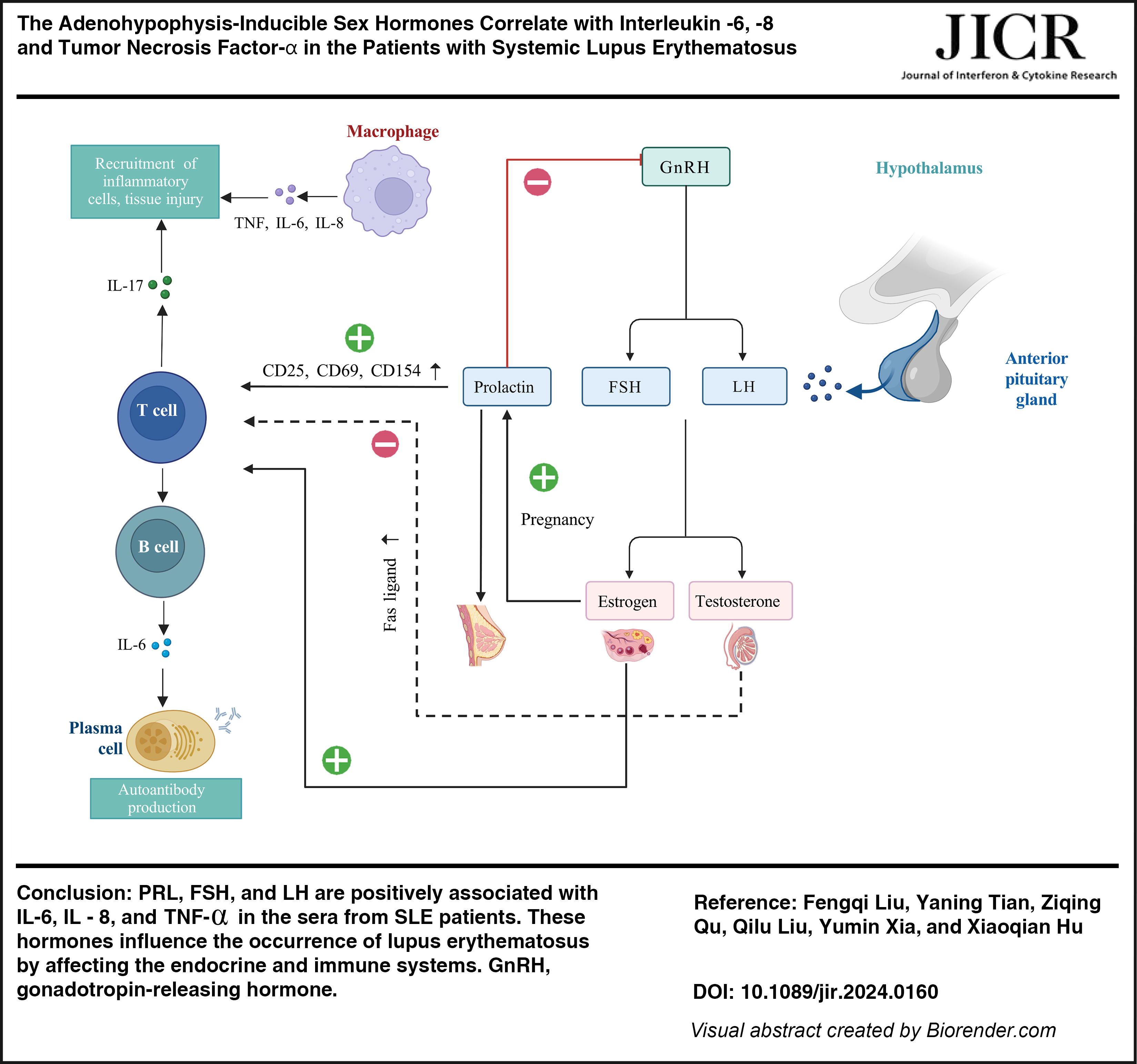
Adenohypophysis-inducible sex hormones include prolactin (PRL), follicle-stimulating hormone (FSH), and luteinizing hormone (LH). These hormones influence the occurrence of lupus erythematosus by affecting the endocrine and immune systems. The present study analyzed the relationship between serum sex hormones and several cytokines in patients with systemic lupus erythematosus (SLE). Compared with the healthy controls, early-onset SLE female patients with menopause had higher PRL levels than the healthy controls and cutaneous lupus erythematosus (CLE) group. FSH levels were higher in male patients with SLE than in the healthy controls or CLE group. In SLE patients, the estradiol levels correlated negatively with interleukin (IL)-8. The levels of FSH versus IL-8, PRL versus IL-6, PRL versus tumor necrosis factor (TNF)-α, and LH versus IL-8 levels were moderately positively correlated. In conclusion, PRL, FSH, and LH are positively associated with IL-6, IL-8, and TNF-α in the sera from SLE patients, which indicates that sex hormone levels can serve as an indicator of disease activity during SLE diagnosis.
Introduction
Lupus erythematosus is an autoimmune disease, and based on the disease spectrum, it is categorized as cutaneous lupus erythematosus (CLE) and systemic lupus erythematosus (SLE). According to the onset age, SLE can be classified as childhood SLE, early-onset SLE, and late-onset SLE. Early-onset SLE refers to SLE diagnosed in adulthood, whereas late-onset SLE refers to cases in which the first clinical symptoms of SLE appear in people at ≥50 years. The average onset age for women is 35 years, and the proportion of people with late-onset SLE is very small (Weckerle and Niewold, 2011). The SLE onset peak in male patients is relatively late, and the peak is often observed at the age of 50–80 years (Gergianaki et al., 2018). Obviously, differences in disease onset are observed between male and female individuals.
Although the pathogenesis of lupus erythematosus pathogenesis is not completely elucidated, it may be related to heredity, epigenetics, immunity, environment, sex hormones, and other factors (Sachdeva and Pal, 2022; Zucchi et al., 2022). Lupus erythematosus is common in women. The male-to-female ratios of CLE and SLE are approximately 1:3 (Petersen et al., 2018) and 1:9, respectively (Nusbaum et al., 2020). However, the advantage of this disease for female patients decreases significantly after menopause (Ortona et al., 2016), and the male-to-female ratio of SLE reduces to 1:5 after menopause. The potential mechanism underlying this gender difference is attributable to sex hormone differences. Oral contraceptives, sex hormone replacement therapy, early menarche, early amenorrhea, and other factors increase the SLE risk (Lateef and Petri, 2012). Thus, sex hormones are a crucial reason for gender differences in SLE.
Most current sex hormone-related studies have focused on young patients, and studies investigating changes in sex hormone levels in CLE and elderly SLE patients are few. Some studies have reported that the testosterone (TESTO) level is lower in male patients than in healthy people (Arnaud et al., 2017). Estradiol (E2) and prolactin (PRL) in SLE patients promote disease development, whereas TESTO and progesterone (PROG) inhibit disease progression. No significant changes are observed in sex hormone levels (Jones et al., 2022; Raeisi et al., 2018). However, no unified conclusion exists regarding changes in sex hormone levels in male patients.
Many cytokines are crucial players in SLE and can serve as indicators for evaluating SLE disease activity. Tumor necrosis factor-α (TNF-α), as a pluripotent cytokine, can regulate B cell activity, and increase antibody production and the expression of vascular cell adhesion protein-1 and intercellular adhesion molecule-1 (Wang et al., 2016). IL-6 is a cytokine necessary for B cell differentiation into plasma cells producing antibodies in the germinal center (Bleck et al., 2024). It can promote T cell function in the periphery. IL-6 can trigger Th17 cell differentiation and participate in their pathogenic process in SLE (Kim et al., 2022). In addition, IL-6 inhibits Treg differentiation and activation, thereby promoting SLE progression. IL-6 levels are elevated in SLE patients and are related to disease activity (Tang et al., 2019). Few studies have examined the involvement of IL-8 in SLE pathogenesis. Kondo-Ishikawa S et al. had shown that cerebrospinal fluid IL-8 level correlates positively with anti-U1 ribonucleoprotein (anti-U1RNP) antibody, which is responsible for the development of neuropsychiatric SLE (Kondo-Ishikawa S et al., 2020). A study suggested that IL-8 was associated with adverse pregnancy outcomes caused by SLE (Pitman et al., 2013). However, a clear understanding of the action mechanism is lacking.
Obviously, both sex hormones and these cytokines are pivotal for SLE development. Therefore, this study explored the correlation between sex hormones and cytokines in SLE patients.
Information and Methods
Object
In total, 141 CLE or SLE patients were recruited from June 1, 2021, to January 1, 2023. All patients strictly met the inclusion and exclusion criteria. Based on the difference in the sex and menstrual cycles, the female patients were categorized into the follicular stage group (18 < age < 50) and menopausal group [which was further divided into the SLE late-onset group (whose first clinical symptoms appeared at the age of ≥50 years), SLE early-onset group (who were diagnosed in adulthood), and CLE group (no systemic symptoms)]. The male patients were divided into the adult male group (18 < age < 50) and the elderly male group (age ≥ 50) for comparison with the female patients.
At the same time, volunteers recruited from the health examination center of our hospital were included as a health control group. The age and sex of the volunteers were matched with those of the corresponding groups. The healthy control group was generally in good condition, with women of childbearing age having regular menstruation and all being in the follicular stage, and menopausal women being menopausal for 12 months. All patients had no history of reproductive systemic disease, autoimmune disease, and cardiovascular disease, and no long-term history of medication. According to their menstrual cycle, the female patients were divided into the follicular group and the menopausal group. Based on their age, the male patients were classified into the adult male group and the elderly male group. Finally, the correlation between sex hormone levels and cytokine levels was analyzed.
The clinical medical records of all the patients included in the study, including the patient’s general condition, laboratory test results, and all results of the last visit, were collated and analyzed. General conditions included name, age, sex, diagnosis, course of disease, and history. Menstrual history was recorded for the female patients. Laboratory tests evaluated 7 parameters related to sex hormones and cytokines.
The assays of serum samples
Blood was drawn from the patients who were on an empty stomach from 8:00 AM to 10:00 AM. Two tubes of venous blood were collected from each participant. Each tube containing 3 mL of blood was centrifuged at 3500 r/min for 15 min in a low-temperature high-speed centrifuge, and the supernatant, namely the serum, was separated. The concentrations of the 7 sex hormone-related parameters were detected through radioimmunoassay, and the original matching reagents were automatically detected using a machine. Cytokine concentrations were determined through rate immune scatter turbidimetry. While testing, each index was strictly evaluated according to the instructions of all testing kits.
Ethics statements
This study has been registered with the Chinese Clinical Trial Registry (ChiCTR2200059621).
Studies involving human subjects
Generated Statement: The studies involving humans were approved by the Institutional Research Ethics Committee of the hospital.
The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Inclusion of identifiable human data
Generated Statement: No potentially identifiable images or data are presented in this study.
Statistical methods
SPSS26.0 statistical software was used to analyze the data, and GraphPad Prism 9 was used to draw pictures. The measurement data were examined for normality before the analysis. For the normal distribution data, the independent sample t-test was conducted to compare 2 groups, whereas multiple groups were compared using one-way ANOVA. For the skewed distribution data, the Mann–Whitney nonparametric test was conducted to compare 2 groups, whereas multiple groups were compared using the nonparametric test of multiple samples. The Spearman rank correlation was used for the correlation analysis. All tests were bilateral, and a statistical difference was considered when P < 0.05.
Results
Baselines
Regarding participants’ age, no significant difference was noted among the subgroups, which indicated that the data were comparable between the participants. These data are detailed in Table 1.
The Age of Lupus Patients and Healthy Controls
Age 18–50 years.
Age ≥50 years.
Normal distribution, using mean ± standard deviation.
Female patients at the follicular stage
Significant differences in TESTO, F-T, E2, and follicle-stimulating hormone (FSH) levels were noted among the 3 groups (P < 0.05) (Figs. 1A–C). TESTO and F-T levels were lower in the SLE patients than in the healthy group, whereas the E2 level was higher in the SLE patients than in the healthy control group, respectively. The E2 level was significantly higher in the CLE patients than in the healthy group. No significant difference in PRL, PROG, and luteinizing hormone (LH) levels was noted among the three groups (P > 0.05). However, after the Bonferroni correction was applied, no statistical difference was noted in the FSH level (P = 0.123) (Supplementary Table S1).

Female patients at the menopausal stage
Sex hormone levels among the late-onset SLE, early-onset SLE, and CLE patients, and healthy controls were further compared. Statistical analysis unveiled significant differences in the TESTO and PRL levels among the 4 groups (P < 0.05) (Figs. 1D and E). A pairwise comparison of sex hormone levels revealed that PRL levels were higher in the early-onset SLE group than in the healthy control and CLE groups, whereas TESTO levels were lower in the early-onset SLE group than in the healthy control group, and the difference was statistically significant (P < 0.05). The PRL level was higher in the late-onset SLE group than in the CLE group, and the TESTO level was lower in the late-onset SLE group than in the CLE and healthy control groups, with the difference being statistically significant (P < 0.05). No significant difference was noted in the LH level after the Bonferroni correction was applied (P = 0.097) (Supplementary Table S2).
Adult male patients
Statistical analysis showed a significant difference in the level of FSH among the three groups (P < 0.05) (Fig. 1F). There was no significant difference in the levels of TESTO, F-T, E2, LH, PRL, and PROG among the 3 groups (P > 0.05). Further pairwise comparison showed that the level of FSH in SLE was higher than that in healthy controls and CLE, and the difference was statistically significant. There was no significant difference in CLE sex hormone levels between the 2 groups (P > 0.05) (Supplementary Table S3).
Elderly male patients
Because all patients in the elderly male group had CLE, differences in sex hormone levels between the CLE and healthy control groups were compared. According to statistical analysis, no statistical differences in sex hormone items were observed between the CLE and healthy control groups (Supplementary Table S4).
Correlation between sex hormones and cytokines
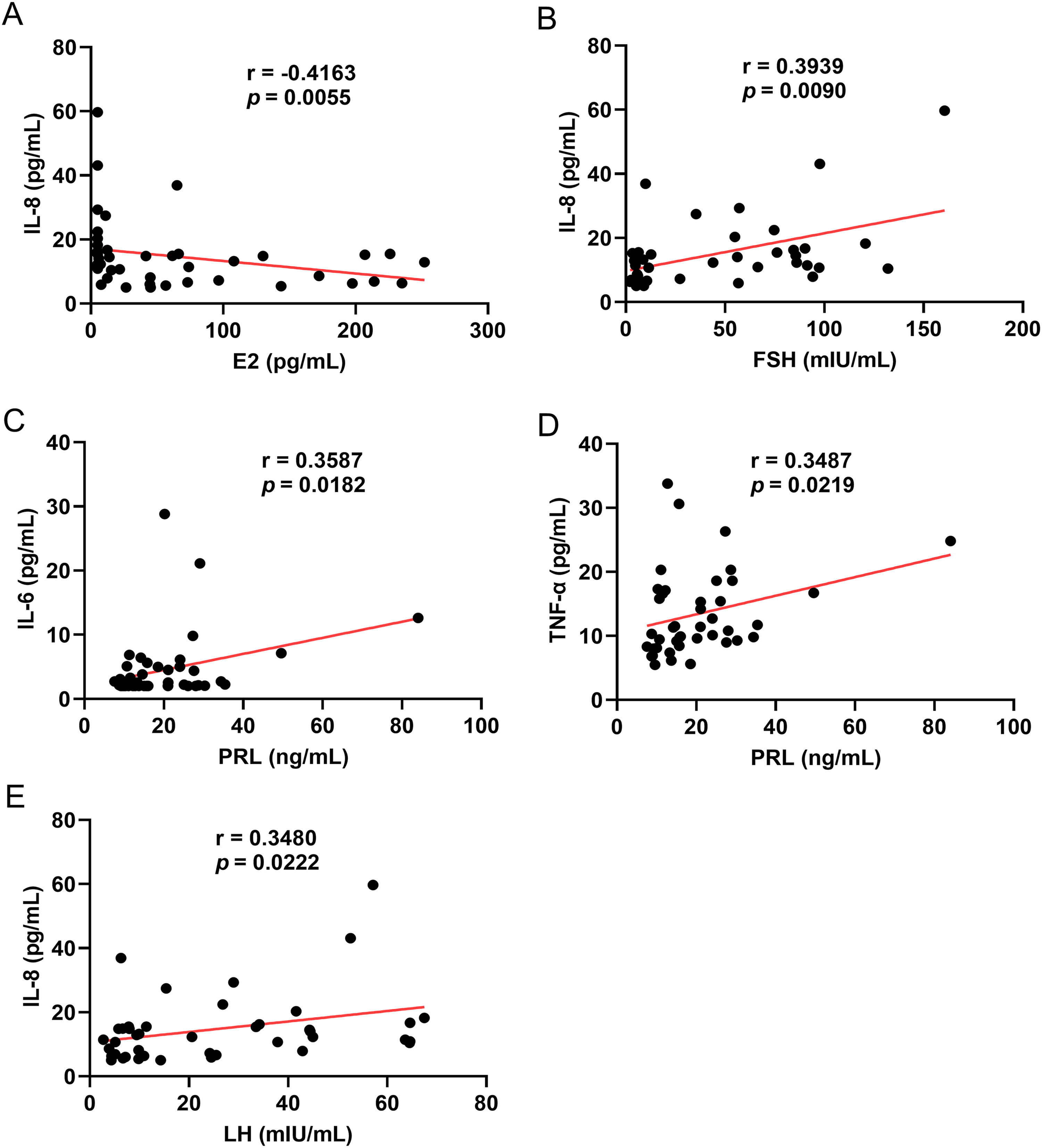
Correlations of the adenohypophysis-inducible sex hormones PRL, FSH, and LH with IL-6, IL-8, and TNF-α were analyzed (Supplementary Table S5). In SLE patients, E2 and IL-8 levels exhibited a weak negative correlation (r = −0.416, P = 0.005). The levels of FSH versus IL-8 (r = 0.394, P = 0.009), PRL versus IL-6 (r = 0.359, P = 0.018), PRL versus TNF-α (r = 0.349, P = 0.022), and LH versus IL-8 levels (r = 0.348, P = 0.022) were moderately positively correlated (Fig. 2).
Discussion
Studies investigating hormone changes in patients with lupus erythematosus have focused on SLE in women of childbearing age. However, many gaps continue to exist in elderly female patients with SLE, male patients with SLE, and CLE patients. The present study focused on changes in sex hormone levels in these patients. IL-6, IL-8, and TNF-α levels in SLE patients were moderately positively associated with the adenohypophysis-inducible sex hormones.
E2 levels increased in the SLE and CLE patients at the follicular stage compared with the healthy people. Meanwhile, TESTO and F-T levels decreased in the SLE patients. These findings are consistent with previous findings (Singh and Bischoff, 2021; Yousefi et al., 2019). Gonadotropin levels can be regulated by positive and negative feedback of E2 and negative feedback of PROG and androgen. In the follicular phase of lupus erythematosus, a statistical difference in FSH levels was noted among the three groups, but the pairwise comparison was corrected. Moreover, changes in sex hormone levels in the CLE group indicated that the gender differences in this group may be an effect of E2, but the effect of other sex hormones was not obvious. The role of sex hormones in CLE is not as obvious as that in SLE.
TESTO levels were significantly lower in menopausal SLE patients than in healthy menopausal individuals. These findings are consistent with those of previous studies (Singh and Bischoff, 2021; Yousefi et al., 2019), indicating the role of estrogen and androgen in disease pathogenesis in females. In the present study, menopausal patients were further categorized into early-onset SLE and late-onset SLE patients. TESTO levels were significantly lower in both early-onset SLE and late-onset SLE groups than in the healthy control groups. This result indicated that the decrease in androgen levels in menopausal patients is not only a factor of age but was also promoted by the disease itself.
Estrogen acts primarily through estrogen receptors (ER). ERα and β activate T cells and upregulate crucial mediators of T cell activation, such as calcineurin and CD40L, thereby playing a role in T cell-mediated inflammation. In addition, estrogen is involved in the development, differentiation, and function of CD4+T cells. A study (Bereshchenko et al., 2018; Pan et al., 2019) unveiled that low E2 levels triggered the Th1 response, whereas high E2 levels might induce the Th2 response. Contrary to estrogen, androgen plays a protective role in SLE. By upregulating Fas ligand expression in T cells to increase their apoptosis (Kim et al., 2010), androgens upregulate the Treg number and function and inhibit Th1 and Th17 cell proliferation and their cytokine secretion (Walecki et al., 2015). PROG exerts an immunomodulatory effect and can hinder the effect of estrogen. It can inhibit T cell proliferation, downregulate the Th1/Th2 proportion (Hughes and Choubey, 2014; Tan et al., 2015), and inhibit the production of Th1 immune response and inflammatory factors. PRL promotes T cell activation and proliferation by increasing the expression of activation molecules such as CD25, CD69, and CD154. It changes the Th1/Th2/Th17 balance, which is associated with SLE pathogenesis (Legorreta-Haquet et al., 2022). Few studies have investigated the involvement of FSH and LH in SLE pathogenesis; hence, a clear understanding of the action mechanism is lacking.
PRL levels increased in the early-onset SLE menopausal group, which indicated that the effect of PRL on the disease does not stop because of menopause. By contrast, PRL levels were higher in the late-onset SLE group than in the healthy control group, but no statistical difference was observed. In menopausal women, because of the decrease in estrogen and PROG levels, the negative feedback effect of gonadotropin decreased and the gonadotropin level increased. The present study exhibited a significant difference in LH levels among the 4 menopausal groups. The statistical method was considered to lose part of its statistical efficacy, making the overall differences and pairwise comparison differences not obvious. In addition, no differences in PROG levels were noted between the SLE menopausal patients and healthy controls, which suggested that PROG exerts no significant protective effect on postmenopausal patients. Moreover, no significant difference was observed between the CLE and SLE patients or healthy people. This indicated that sex hormones exert a slight effect on CLE after menopause, but this needs to be further verified in a larger sample size.
FSH levels were significantly higher in the adult male SLE patients than in the healthy controls, which may be because of the combined action of estrogens and androgens. No changes in E2, PROG, PRL, and androgen levels were noted, which suggested that the imbalance between immune-promoting and protective sex hormones in male SLE patients is related to SLE occurrence.
Regarding the relationship between sex hormones and immune indicators, a weak negative correlation was observed between E2 and IL-8 levels. This finding was consistent with the results of previous studies (Bereshchenko et al., 2018; Pan et al., 2019). The current study on gonadotropins is predominantly focused on PRL. PRL promotes the production of CD40L and cytokines, such as IL-6, thereby leading to autoantibody production (Legorreta-Haquet et al., 2022). In SLE, PRL prolonged the life cycle of autoreactive B-lymphocytes and their ability to produce pathogenic autoantibodies. PRL increases the ability of immune cells to proliferate and produce cytokines such as TNF-α (Fojtíková et al., 2010). Moreover, serum IL-8 and FSH levels were elevated in SLE patients (Mao et al., 2018; Wen and Li, 1993). Adenohypophysis-inducible sex hormones are predominantly involved in SLE pathogenesis through an interaction between the sex hormones. They also influence the occurrence of lupus erythematosus by affecting the immune system.
This study has some limitations. While including patients, the number of male patients with lupus erythematosus was small. Moreover, this study did not classify CLE patients. Furthermore, the action mechanism of gonadotropin secreted by the pituitary gland on inflammation in SLE patients remains unclear. Therefore, in follow-up studies, the sample size must be increased to explore changes in the sex hormone levels of male and CLE patients. Additional animal experiments and molecular biology experiments are required to elucidate the role of hormones in SLE pathogenesis.
Conclusions
In conclusion, IL-6, IL-8, and TNF-α levels in SLE patients are positively correlated with PRL, FSH, and LH levels, which indicates that sex hormone levels can serve as new indicators of disease activity during SLE diagnosis. The precise mechanism underlying the effect of these hormones on disease development in SLE should be explored in future studies.
Footnotes
Acknowledgments
This work was supported by
Authors’ Contributions
F.L.: Data curation, formal analysis, investigation, writing—original draft. Y.T.: Formal analysis, investigation, writing—review and editing. Z.Q.: Validation, writing—review and editing. Q.L.: Writing—original draft, writing—review and editing. Y.X.: Conceptualization, supervision, writing—review and editing. X.H.: Conceptualization, data curation, formal analysis, supervision, writing—original draft, writing—review and editing.
Author Disclosure Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding Information
This work was supported by
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.