
Abstract
The causal relationship between inflammatory factors and acute pancreatitis (AP), chronic pancreatitis (CP), alcohol-induced acute pancreatitis (AAP), and alcohol-induced chronic pancreatitis (ACP) remains unclear. We aimed to examine the casual relationship between inflammatory factors and various forms of pancreatitis, namely, AP, CP, AAP, and ACP. We employed a two-sample Mendelian randomization (MR) analysis to investigate the causal relationship between 91 inflammatory factors and 41 inflammatory factors with respect to pancreatitis. The primary analysis involved the use of the inverse variance weighting (IVW). MR-Egger intercept test, Cochran’s Q test, MR-PRESSO test, and Leave-One-Out analysis were used to assess the robustness of our findings. IVW analysis revealed evidence of association between 24 inflammatory cytokines and pancreatitis. Specifically, six cytokines were associated with AP, eight cytokines were associated with CP, three cytokines were associated with AAP, and seven cytokines were associated with ACP. The most significant associations were observed with β nerve growth factor (odds ratio [95% confidence interval]: 6.05 [1.59, 23.01]) and interleukin-4 [IL-4; 2.56 (0.91, 7.16)] in AAP, as well as interleukin-2 receiver subunit beta and IL-4 in ACP. Our findings suggest that certain inflammatory cytokines may have a significant role in the development of pancreatitis.
Introduction
Pancreatitis is a complex and chronic inflammatory disease that affects the pancreas. It encompasses various clinical subtypes, including acute pancreatitis (AP), chronic pancreatitis (CP), alcohol-induced acute pancreatitis (AAP), and alcohol-induced chronic pancreatitis (ACP) (Ashizawa et al., 1999). In 2017, it is estimated that pancreatitis affected over 16 million people worldwide, resulting in disability for nearly 4 million individuals (Beger, 1991). AP is a common cause of hospitalization in the gastrointestinal field (Beger and Rau, 1995). Around 8% of AP cases progress to CP, which is associated with an increased risk of metabolic diseases such as diabetes, osteoporosis, and pancreatic cancer. Therefore, it is crucial to identify modifiable risk factors for pancreatitis in order to prevent the disease and reduce the subsequent burden on health and economy (Bollen, 2016).
Inflammatory cytokines, which are signaling molecules produced by immune cells, play a significant role in the aggregation and activation of inflammatory cells such as monocytes, macrophages, and T cells during an inflammatory response (Antkowiak et al., 2022; Barthet et al., 1999). They also induce the expression of inflammation-related genes and the production of cytokines. Currently, it is believed that inflammatory cytokines have the potential to contribute to the development of pancreatitis, making anti-inflammatory cytokine therapy an important treatment strategy (Beger et al., 1997; Bentrem and Joehl, 2003). Studies have demonstrated that certain inflammatory cytokines, such as interleukin 1 (IL-1), interleukin 6 (IL-6), interleukin 17 (IL-17), and tumor necrosis factor α (TNF-α), are elevated in AP, leading to inflammation and pancreatic destruction, thus exacerbating the condition (Biczo et al., 2018). Moreover, research has shown that TNF-α, interleukin 23 (IL-23), IL-17, and other inflammatory cytokines play a crucial role in the development of alcoholic pancreatitis. These cytokines are produced by activated immune cells and stimulate the recruitment of inflammatory cells to the pancreatic tissue, ultimately leading to the deterioration of the pancreatic structure (Binker and Cosen-Binker, 2014).
A number of Genome-Wide Association Studies (GWAS) studies have identified genetic loci closely related to pancreatitis. These studies have also revealed the mechanism of related genes of inflammatory factors, providing feasible instrumental variables (IVs) (Birney, 2022; Sekula et al., 2016). Mendelian randomization (MR) is a research method that uses germline genetic variation as IV to explore and infer causality of various exposures. In this study, we aimed to investigate the causal relationship between inflammatory factors and different types of pancreatitis through a comprehensive multigroup two-sample MR analysis (Larsson et al., 2023). Data on four types of pancreatitis (CP, AP, ACP, and AAP) were obtained from the FinnGen consortium (Ho et al., 2022). By employing an MR strategy, we explored the potential causal impact of inflammatory factors on pancreatitis risk. Based on these findings, we aimed to understand the role of inflammatory factors in the development of pancreatitis and identify potential therapeutic targets for interventions in this disease (Smith and Ebrahim, 2003).
Materials and Methods
Sample study
In a recent meta-analysis GWAS, 91 inflammatory cytokines were examined in a study involving 14,824 participants of European ancestry from 11 cohorts. The Olink Target Inflammation panel was used to measure 91 plasma proteins. The GWAS Catalog platform (https://www.ebi.ac.uk/gwas/publications/37563310) provided the data for these 91 cytokines. Additionally, data on 41 inflammatory cytokines were obtained from a study involving 8,293 Finns, which explored the associations between genomic variants and cytokines and growth factors. The GWAS Catalog platform (https://www.ebi.ac.uk/gwas/publications/27989323) was the source for the statistical summary of these 41 cytokines. Single nucleotide polymorphisms (SNPs) associated with the circulating levels of the 91 inflammatory cytokines were selected based on genome-wide significance (P < 5 × 10−8). After pooling the SNP data, SNPs with linkage disequilibrium were pruned using an r 2 threshold of <0.1. Finally, the SNP with the lowest P value was chosen as an independent instrument.
Summary of GWAS statistics for AP, AAP, CP, and ACP were obtained from the FinnGen consortium. The FinnGen research projects involve more than 500,000 people and review their genetic information through the Finland Biological Bank subsidiary (https://finngen.gitbook.io/documentation). The data were integrated with electronic health records from healthcare registries, as well as data from cancer, cause of death, and drug reimbursement registries. We utilized the FinnGen R5 version of the alliance for this analysis. In this dataset, AAP has 457 cases and 218,335 controls (https://risteys.finngen.fi/phenocode/ALCOPANCACU), AP has 195,144 cases and 3,022 controls (https://risteys.finngen.fi/endpoints/K11_ACUTPANC), ACP has 977 cases and 217,815 controls (https://risteys.finngen.fi/phenocode/ALCOPANCCHRON), and CP has 1,737 cases and 195,144 controls (https://risteys.finngen.fi/phenocode/K11_CHRONPANC). Variables such as sex, age, genetic component, and genotyping batch variation were taken into account to calibrate genetic linkage. Ethical approval was obtained from the FinnGen steering committee for all selected GWASs in the FinnGen Consortium, and individuals provided written informed consent.
Statistical methods
We present the findings of our study, which involved conducting a series of MR analyses to ensure reliable causal inference and detect pleiotropy. The primary method we used was the random-effects inverse variance weighting (IVW) or MR-Egger method. IVW assumes the validity of all genetic variants and provides the most powerful estimate of MR (Haller et al., 2016). MR-Egger regression allows for the possibility of all SNPs being null and produces causal estimates that are robust against pleiotropy. To obtain unbiased causal estimates with small standard errors, we employed a maximum likelihood (ML) approach in the absence of heterogeneity and horizontal pleiotropy. This approach maximizes the likelihood of SNP effects on exposure and outcome (Burgess and Thompson, 2011). Additionally, we utilized the weighted median approach, which includes ineffective instruments but still yields precise causal estimates for pleiotropy as long as at least half of the instruments are valid (Bowden and Holmes, 2019).
To ensure the robustness of our findings and address any possible violation of the MR assumption, we conducted a sensitivity analysis. First, we applied Cochran’s Q test to assess the heterogeneity of SNPs in both the IVW and MR Egger’s method. We used MR-PRESSO analysis to identify any outliers (Larsson et al., 2023). Next, we performed a “leave-one-out” analysis to evaluate the impact of individual SNPs on the causal effect estimates, in order to check for potential bias or interference. Additionally, we used the MR Egger intercept test to assess the pleiotropic association between genetic variants and other potential confounders. We examined the deviation of the regression intercept from zero to determine the presence of horizontal pleiotropy (Ho et al., 2022).
Results
Causal relationship between inflamed cytokines and pancreatitis
In total, 120 SNPs were found to be associated with AP, 125 SNPs with CP, 43 SNPs with AAP, and 91 SNPs with ACP (Table 1; Supplementary Tables S1, S2, S3, and S4; Supplementary Figs. S1, S2, S3, S4, S5, S6, S7, and S8). In our IVW analysis, we discovered evidence of an association between 24 inflammatory cytokines and pancreatitis (Table 1). Among the known inflammatory cytokines, six were associated with AP, eight with CP, three with AAP, and seven with ACP (Table 1; Fig. 1).
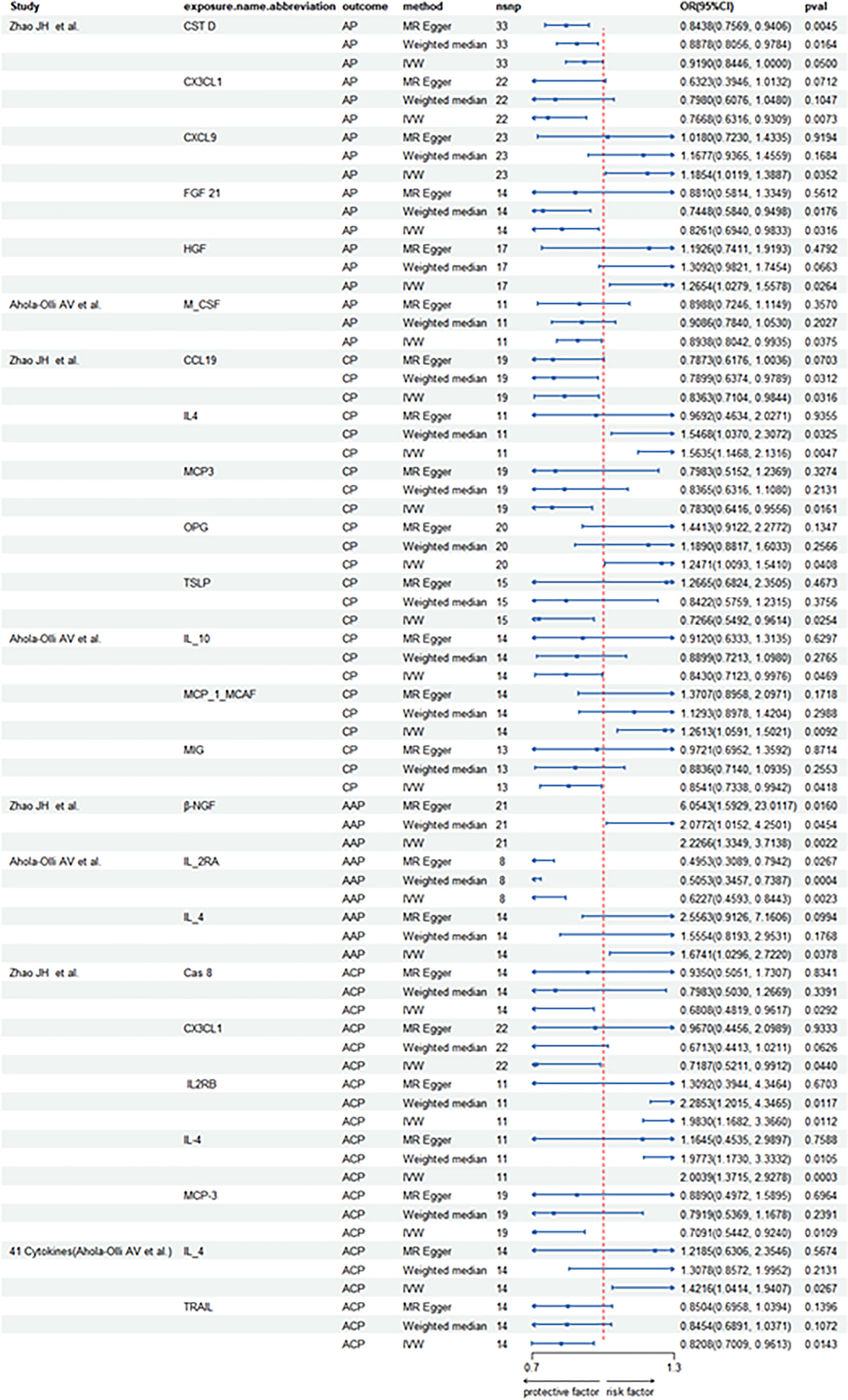
Causal correlations of cytokines on pancreatitis (AP, CP, AAP, and ACP). The change in the odds ratio (OR) of 4 pancreatitis per 1-SD rise in the cytokine level is shown by OR and 95% confidence interval. AAP, alcohol-induced acute pancreatitis; ACP, alcohol-induced chronic pancreatitis; AP, acute pancreatitis; CP, chronic pancreatitis; SD, standard deviation.
Causal Effects of Significant Cytokines Traits on AP, CP, AAP, ACP, and Cholelithiasis Estimated by Different Two-Sample MR Methods
AAP, alcohol-induced acute pancreatitis; ACP, alcohol-induced chronic pancreatitis; AP, acute pancreatitis; CP, chronic pancreatitis; IVW, inverse variance weighting; Ici95, lower confidence interval (95%); MR, Mendelian randomization; OR, odds ratio; se, standard error; uci95, upper confidence interval (95%).
For AP, there are two inflammatory factors that have positive effects on AP, the odds ratio [95% confidence interval] of C-X-C motif chemokine 9 (CXCL9) was 1.1854 [1.0119,1.3887] and the OR [95% CI] of hepatocyte growth factor (HGF) was 1.2654 [1.0279,1.5578]. Four inflammatory factors had the opposite effect on AP, these cytokines include cystatin D (CST D), fractalkine (CX3CL1), fibroblast growth factor 21 (FGF21), and macrophage colony-stimulating factor (M_CSF) (Table 1; Supplementary Table S1; Fig. 1; Supplementary Figs. S4 and S8).
For CP, we found that eight inflammatory factors were associated with it, three of which were positive. The identified inflammatory factors are osteoprotegerin (OPG), interleukin-4 (IL-4), and monocyte chemoattractant protein-1 (MCP-1/MCAF), with odds ratios (ORs) and 95% confidence intervals (CIs) as follows: OPG, 1.24 (1.00, 1.55), IL-4, 1.14 (1.14, 2.13) and MCP-1/MCAF, 1.26 (1.05, 1.50). At the same time, there were five inflammatory factors that had the opposite effect on CP, including C-C motif chemokine 19 levels (CCL19), Monocyte chemoattractant protein-3 levels (MCP3), and monocyte chemoattractant protein-3 levels (MCP3). Thymic stromal lymphopoietin levels (TSLP), interleukin-10 levels (IL_10), and monokine induced by gamma interferon levels (MIG) (Table 1; Supplementary Table S2; Fig. 1; Supplementary Figs. S3 and S7).
Three inflammatory factors associated with autoimmune pancreatitis (AAP) were identified, with β-nerve growth factor (β-NGF; OR [95% CI]: 6.05 [1.59, 23.01]) and interleukin-4 (IL-4; OR [95% CI]: 2.56 [0.91, 7.16]) showing positive correlations. Conversely, interleukin-2 receptor subunit alpha (IL-2RA) exhibited an opposite effect (Table 1; Supplementary Table S3; Fig. 1; Supplementary Fig. S2; Supplementary Fig. S6). On the contrary, ACP was associated with seven inflammatory factors, four of which showed positive correlations. These included interleukin-2 receptor subunit beta (IL2RB; OR [95% CI]: 1.98 [1.17, 3.37]), IL-4 (OR [95% CI]: 1.16 [0.45, 2.99]), and IL-4 (OR [95% CI]: 1.22 [0.63, 2.35]) (Table 1; Supplementary Table S4; Fig. 1; Supplementary Figs. S1 and S5). Among the four types of pancreatitis, β-NGF (OR [95% CI]: 6.05 [1.59, 23.01]) had the strongest positive association, followed by IL-4 (OR [95% CI]: 2.56 [0.91, 7.16]) (Table 1). It is noteworthy that all causal effects were estimated in the same direction as the IVW pattern, which enhances the robustness of the causal effects of inflammatory factors on pancreatitis. Although some causal effects estimated by the MR-Egger method did not reach statistical significance, the Rucker framework in MR analysis deemed IVW to be more suitable for interpreting the MR results (Table 1; Supplementary Tables S1, S2, S3, and S4; Fig. 1; Supplementary Figs. S1, S2, S3, S4, S5, S6, S7, and S8).
Sensitivity analysis
To evaluate the robustness of the findings, several sensitivity analyses were conducted. Based on Cochran’s Q test of the IVW method and MR Egger method, it was found that none of the inflammatory cytokines significantly associated with pancreatitis exhibited heterogeneity in the IV variables (P > 0.05).
The results of MR Analysis did not show any significant horizontal pleiotropy, as confirmed by MR-Egger regression intercept analysis. The effect directions of the three methods were consistent with the IVW method. The IVW radial MR results demonstrated that the corrected results were consistent with the precorrected results. Additionally, when each SNP was removed one by one using Leave-One-Out, the effect size of the result remained almost the same as that of the total MR, indicating strong robustness (Table 1; Supplementary Tables S9, S10, and S11; Supplementary Figs. S1, S2, S3, S4, S5, S6, S7, and S8).
Discussion
In this study, we utilized multigroup MR Analysis to comprehensively assess the potential causal relationship between 91 inflammatory cytokines (including growth factors, interleukins, and chemokines) and 41 inflammatory cytokines with four clinical subtypes of pancreatitis. The findings revealed significant associations, suggesting that a genetic predisposition to pancreatitis is linked to elevated levels of inflammatory factors, which contribute to the positive effects mentioned earlier. Regarding AP, our results demonstrate that CXCL9 and HGF have positive effects, whereas CSTD, CX3CL1, FGF-21, and M_CSF have inverse effects. Genetic susceptibility indicates that these factors mitigate the increase in AP pathogenesis. OPG, TSLP, and MCP_1_MCAF have positive effects on AP pathogenesis. In the case of alcoholic pancreatitis, the inflammatory factors that positively correlate with AAP include β-NG and IL_4, whereas those positively correlated with ACP include IL2RB, IL-4, and IL_4. The genetic predisposition to pancreatitis provides suggestive evidence of elevated levels of inflammatory factors contributing to the aforementioned positive effects, and sensitivity analyses confirm the robustness of these findings.
Pancreatitis is an inflammatory disease of the pancreas that can be acute or chronic. It is characterized by the destruction of acinar cells, leading to the activation of various inflammatory cells such as macrophages and granulocytes. These inflammatory cells secrete large amounts of proinflammatory cytokines, which in turn activate pancreatic stellate cells, the main cells involved in pancreatic fibrosis. During pancreatic injury, atrophic acinar cells activate key players in inflammation, including macrophages and granulocytes, and release various proinflammatory cytokines, such as IL-4. IL-4 has been implicated in the pathogenesis of AP, and studies have suggested its role, along with the IL-4 receptor (IL-4R), in pancreatic pathogenesis. Additionally, increased serum levels of IL-1β have been associated with the development of AP, further supporting our study’s conclusion that IL-4 has a detrimental effect on the development of AAP.
CXCL9 is a vital proinflammatory cytokine that influences the progression of both acute and CP, as well as pancreatic cancer (Ohkawara et al., 2017). CXCL9 activates the gp130 and JAK/STAT signaling pathway. This activation contributes to inflammation and damage in the pancreas. Additionally, research indicates that pancreatitis patients have higher serum levels of CXCL9 than healthy individuals (Melzer et al., 2023).
Laboratory studies have shown that human pancreatic periacinar myofibroblasts have a greater capacity to secrete HGF when exposed to inflammatory mediators such as TNF-α, IL-17, and IL-1β (Ohkawara et al., 2017). Abnormal expression and dysregulation of HGF, which is a secondary signaling molecule involved in pancreatic inflammation, suggest that it may be a valuable early marker for pancreatitis. Furthermore, our study reveals a strong association between TSLP and both the development and progression of CP. TSLP, or thymic stromal lymphoprotein, continues to be present whenever there are defects in the pancreatic barrier, suggesting that it could serve as a biomarker for CP (Shen and Li, 2015; Shimizu et al., 2022; Szatmary et al., 2022).
This study possesses several strengths in terms of data sources and study design. First, the MR Design enables the estimation of the causal relationship between two intricate genetic traits, thereby circumventing the biases inherent in traditional observational epidemiological studies. Multiple sensitivity analyses were conducted to validate the IV assumptions and interpret the results while accounting for horizontal pleiotropy and outliers. Second, the GWAS data utilized in this study predominantly consisted of participants with European ancestry, potentially minimizing population stratification bias.
Using MR analyses, we provide strong evidence of a causal relationship between inflammatory factors and pancreatitis. However, there are certain limitations to this study. First, there may be sample overlap issues that could affect the precision of the conclusions. Although we minimized this by carefully selecting GWAS datasets and utilizing a relative bias of less than 0.002. Second, the samples primarily consisted of European populations, which may limit the generalizability of the results. To improve the generalizability, future studies should include data from more ethnic groups. Third, despite excluding pleiotropic instruments and using MR-Egger intercept and MR-PRESSO tests, the potential indirect effects of IVs remain a challenge. Fourth, we did not explore the nonlinear effects of inflammatory factors and pancreatitis. This can be further investigated through single-sample MR Analysis in future studies. Fifth, we did not consider reverse causality between inflammatory factors and pancreatitis. Future trials should assess the effect of inflammatory factor interventions on pancreatitis. In summary, this study systematically explored the causal relationship between pancreatitis and inflammatory factors, providing new insights into the understanding of risk factors and mechanisms of pancreatitis. It also lays the foundation for the development of targeted treatment strategies.
Conclusions
Our study found evidence of an association between 24 inflammatory cytokines and pancreatitis. Specifically, six cytokines were associated with AP, eight with CP, three with AAP, and seven with ACP. We observed a positive effect of CXCL9 and HGF on AP. OPG, TSLP, and MCP_1_MCAF were found to have positive effects on CP. Inflammatory factors such as β-NG and IL_4 were positively correlated with AAP, whereas IL2RB, IL-4, and IL_4 were positively correlated with ACP. Our findings suggest that individuals with a genetic predisposition to pancreatitis may have elevated levels of inflammatory factors, contributing to these positive effects. This study lays the foundation for further understanding the etiology of pancreatitis and provides new insights into the role of pancreatitis and inflammatory factors in its pathogenesis.
Footnotes
Acknowledgments
The authors thank all authors for their contributions to the article.
Authors’ Contributions
H.Y. and Y.Z.: Methodology. W.C.: Formal analysis and investigation. H.L.: Writing—original draft preparation. H.Y.: Writing—review and editing.
Data Availability
Author Disclosure Statement
The authors have declared that no competing interests exist.
Funding Information
This work was supported by Beilun Health Technology Project (2024BLWSQN014).
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
Supplementary Figure S6
Supplementary Figure S7
Supplementary Figure S8
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4
Supplementary Table S5
Supplementary Table S6
Supplementary Table S7
Supplementary Table S8
Supplementary Table S9
Supplementary Table S10
Supplementary Table S11