
Abstract
We previously reported the peripheral blood cell patterns of expression for the migration inhibitory factor (MIF) canonical (CD74/CD44) and noncanonical receptors (CXCR2, CXCR4, and CXCR7) in rheumatoid arthritis (RA) patients and correlated this with clinical biomarkers and disease activity. This study aimed to evaluate the expression of these receptors alongside the serum levels of CXCL12 and CXCL8 (ligands for CXCR2, CXCR4, and CXCR7), which potentially regulate the action of these receptors and the influence the downstream effects of MIF. Additionally, we evaluated soluble levels of MIF, as well as its soluble cognate receptor (sCD74), in the serum of RA patients and control subjects (CS). Our findings revealed distinctive membrane expression patterns of MIF receptors in active (moderate and high disease activity) and non-active (low activity and remission) RA patients. Furthermore, RA patients exhibited elevated serum sCD74 levels, which correlated with disease activity, and elevated CXCL12 levels, which correlated with rheumatoid factor titers. Regarding serum CXCL8 and MIF levels, we observed higher CXCL8 levels in RA patients compared to CS, while MIF levels did not significantly differ between groups or by disease activity. The circulating sCD74/MIF ratio was elevated in RA patients, particularly in cases of moderate disease activity. Our study also indicated that treatment protocols did not significantly impact circulating MIF levels or the expression of its receptors. This study extends previous findings by supporting a role for sCD74 in downregulating MIF action and in the potential value of the sCD74/MIF ratio as a disease biomarker in RA.
Introduction
Rheumatoid arthritis (RA) is a chronic inflammatory autoimmune disease of heterogeneous etiology that arises by the interaction between genetic predisposition and environmental factors. The pathogenesis of RA is characterized by synovial inflammation, which causes joint damage and can progress to lifelong disability (Fonseca Peixoto et al., 2022; Kondo et al., 2021). Pathological interactions among cells and mediators of the innate and adaptive immune system drive the local and systemic inflammatory changes observed at various stages of the disease (Petrelli et al., 2022).
A hallmark of RA is the overproduction of pro-inflammatory cytokines, such as TNF-α, IL-1, IL-6, and IL-17, which perpetuate synovial inflammation and joint degradation. Along with these cytokines, molecules such as matrix metalloproteases and RANKL play a significant role in tissue destruction (Gravallese and Firestein, 2023). Macrophage migration inhibitory factor (MIF) is another cytokine identified as a mediator of the inflammatory process, with high levels found in the serum, plasma, and synovial fluid of RA patients (Llamas-Covarrubias et al., 2013; Morand et al., 2006). Initially described in 1966, MIF was identified as a product of T lymphocytes capable of inhibiting the random migration of macrophages (Bloom and Bennett, 1966; David, 1966). Currently, MIF is widely recognized as a pleiotropic cytokine that can be secreted by multiple subtypes of cells and plays a significant role in modulating immune and inflammatory responses (Bilsborrow et al., 2019; Brennan-Bourdon et al., 2015; Bucala, 1996; Llamas-Covarrubias et al., 2013; Morand et al., 2006).
The importance of MIF in RA and other autoimmune diseases stems from its role as an upstream mediator of the inflammatory cascade that is capable of inducing the expression of cytokines such as IL-1 and TNF-α. In RA, MIF directly or indirectly exacerbates the inflammatory process by promoting synoviocyte proliferation and survival, neutrophil chemotaxis, and inducing angiogenesis and osteoclast differentiation (Baugh et al., 2002; Bilsborrow et al., 2019; Llamas-Covarrubias et al., 2013; Radstake et al., 2005).
A particular characteristic of MIF is that it can bind to a series of chemokine receptors known as “noncanonical” (CXCR2, CXCR4, and CXCR7), which also are targeted by other ligands (CXCL8 and CXCL12) with higher affinities for these receptors. Additionally, MIF interacts with a receptor/co-receptor duo (CD74/CD44) that forms the well-established “canonical” MIF receptor complex (Lacy et al., 2018; Leng et al., 2003; Leng and Bucala, 2006; Lue et al., 2011; Shi et al., 2006). Although the role of MIF in RA has been studied extensively, there is a gap in knowledge regarding the contribution of its different receptors in modulating clinical activity in this disease. To address this gap, our research group conducted a study evaluating the expression of both canonical (CD74/CD44) and noncanonical (CXCR2, CXCR4, and CXCR7) MIF receptors in RA patients. We also examined the serum levels of CXCL12 and CXCL8, alternative ligands for CXCR2, CXCR4, and CXCR7, which may potentially regulate the expression of these receptors and influence MIF’s downstream functions. Finally, we determined the soluble levels of MIF and its cognate receptor, CD74, in the serum of RA patients and correlated all measured values with clinical biomarkers and disease activity, as assessed by the Disease Activity Score-28 using the Erythrocyte Sedimentation Rate (DAS28-ESR). This study revealed that the soluble form of CD74 (sCD74) could function as a decoy receptor for MIF, thereby inhibiting MIF signaling through its membrane receptors. Our findings offer insights into the MIF-related mechanisms of RA, potentially guiding the development of more targeted treatment strategies for this disease.
Materials and Methods
Patient biospecimens
We adhered to the ethical guidelines and principles established during the original study by using the same patient cohort in this study. Informed consent was obtained from all participants. Additionally, the study protocol received ethical approval from the Research, Ethics, and Biosafety Committee of CUCS,
Clinical assessment
A rheumatologist evaluated all patients and recorded their clinical and demographic data. Clinical activity was assessed by the DAS28, considering ESR values. According to DAS28 score, patients were stratified into remission (DAS28 <2.6; n = 27), low activity (DAS28 ≥2.6 <3.2; n = 16), moderate activity (DAS28 ≥3.2 <5.1; n = 35), and high activity (DAS28 ≥5.1; n = 23). Functional disability was evaluated by the Spanish version of the Health Assessment Questionnaire-Disability Index (HAQ-DI). In the RA patients’ group, rheumatoid factor (RF) and high-sensitivity C-reactive protein (hsCRP) were determined by turbidimetry (A25 Biosystems, Spain) and anti-cyclic citrullinated peptide antibodies (anti-CCP) by indirect ELISA (Axis-Shield, UK; FCCP400). Erythrocyte sedimentation rate (ESR) was measured in both study groups using the Wintrobe method.
Flow cytometry
The expression of canonical and noncanonical MIF receptors in the membrane of T lymphocytes, B lymphocytes, monocytes, and granulocytes from RA patients and CS was determined by flow cytometry from whole blood samples. Multicolored labeling was performed using the following corresponding monoclonal antibody panel to identify cellular sub-populations: CD3 (APC/Cy7 anti-human CD3 Antibody Cat. 300426, Biolegend), CD4 (Alexa Fluor® 488 anti-human CD4 Antibody Cat. 300519, Biolegend), CD14 (PE/Cy7 anti-human CD14 Antibody Cat. 325618, Biolegend), and CD19 (PerCP/Cy5.5 anti-human CD19 Antibody Cat. 302230, Biolegend). In addition, labeling included CD74 (anti-human PE CD74 Antibody Cat. 326808, Biolegend), CD44 (APC anti-human CD44 Antibody Cat. 338806, Biolegend), CXCR2 (PE anti-human CD182 [CXCR2] Antibody Cat. 320706, Biolegend), CXCR4 (APC anti-human CD184 [CXCR4] Cat. 306510, Biolegend), and CXCR7 (APC anti-human CXCR7 Antibody Cat. 391406, Biolegend). Isotype control IgG antibodies conjugated with the same fluorochromes served as negative controls (Biolegend Inc., San Diego, CA, USA). A fluorescence minus one (FMO) experiment was included as a negative control to accurately identify positive events for CD74, CD44, CXCR2, CXCR4 and CXCR7. Samples were analyzed in the acoustic focusing Attune® NxT flow cytometer (Life Technologies). The data obtained were analyzed using FlowJo software v10.0 (TreeStar, Inc., Ashland, Oregon, USA). Initially, lymphocytes were gated based on their forward scatter (FC) and side scatter (SSC) characteristics. Subsequent gates were placed around CD3 + CD4 + T cells, CD19+ B cells, CD14+ monocytes, and granulocytes to evaluate the expression of canonical and noncanonical receptors.
Quantification of soluble levels of MIF, sCD74, CXCL12, and CXCL8
To quantify the serum levels of cytokines and chemokines, including MIF, sCD74, CXCL12, and CXCL8, serum was obtained from peripheral blood samples collected from the study groups.
Serum MIF quantification
Serum MIF levels were quantified using the Enzyme-Linked Immunosorbent Assay (ELISA) method, specifically with the Human MIF ELISA Kit (Biolegend®) following the manufacturer’s instructions. The assay’s minimum detection limit for soluble MIF is 6 pg/mL.
Serum CD74 quantification
Serum CD74 levels were quantified with the Human CD74 ELISA Kit (Sigma-Aldrich), according to the manufacturer’s instructions. The assay has a detection limit of 2500 pg/mL for soluble CD74.
Serum CXCL12 quantification
Serum CXCL12 levels were quantified using the SDF-1 alpha/CXCL12A Human ELISA Kit (Thermo Fisher) according to the manufacturer’s instructions. The assay’s detection limit for soluble CXCL12 is 6000 pg/mL.
Serum CXCL8 quantification
Serum CXCL8 levels were quantified with the IL-8 Human ELISA Kit (Thermo Fisher), following the manufacturer’s instructions. The assay’s detection limit for soluble CXCL8 is 1000 pg/mL.
Statistical analysis
Statistical analysis was conducted using STATA v12.0, GraphPad Prism v5.0, and R Studio v1.4.1103. For descriptive analysis, nominal discontinuous variables were expressed as frequencies, continuous variables with a parametric distribution as means ± SD, and nonparametric variables as medians along with minimums, maximums or 5-95th percentiles. For inferential analysis, the Mann–Whitney U test was applied to non-parametric data from two groups, while the Kruskal–Wallis test was used for comparisons involving more than two groups. Statistical significance was established at a P value of <0.05.
Results
Clinical and demographic characteristics of RA patients
This study included 101 RA patients, 80.2% of whom were women (81 out of 101). Additionally, 30 healthy individuals served as control subjects (CS), with 76.3% being women (23 out of 30). The median age for RA patients was 54 years (range: 19–91), while for CS, it was 48.5 years (range: 32–79), showing no significant age difference (P > 0.05).
RA patients had a median disease duration of 7 years (range: 1–40). For autoantibodies, the median rheumatoid factor (RF) was 67.31 IU/mL (range: 22–90), and the median anti-cyclic citrullinated peptide (anti-CCP) was 291.73 U/mL (range: 0–5873.7). A significant number of patients exhibited high RF titers (≥60 IU/mL, 64.2%) and elevated anti-CCP levels (≥15 U/mL, 89.6%). The mean high-sensitivity C-reactive protein (hsCRP) level in RA patients was 6.8 mg/L (range: 0.3–60.4).
Compared to the CS group, RA patients exhibited significantly higher erythrocyte sedimentation rate (ESR) values with a median of 37 mm/h (range: 3–64) versus 14.5 mm/h (range: 4–45), for the CS group (P < 0.05). Disability was assessed using the Spanish version of the Health Assessment Questionnaire-Disability Index (HAQ-DI), which yielded an average score of 0.625 (range: 0–2.9). This indicates that most patients experienced mild disabilities, typically scoring between 0 and 1 on the HAQ-DI. In terms of treatment, the majority of patients were receiving one or more disease-modifying anti-rheumatic drugs (DMARDs) and nonsteroidal anti-inflammatory drugs (NSAIDs).
Principal component analysis (PCA) of the membrane expression of the canonical (CD74/CD44) and noncanonical (CXCR2, 4, and 7) receptors of MIF in patients with active and non-active RA
PCA was employed to identify patterns in the membrane expression of canonical (CD74/CD44) and noncanonical (CXCR2, CXCR4, and CXCR7) MIF receptors among whole blood CD3+ CD4+ T helper cells, CD19+ B cells, CD14+ monocytes, and granulocytes. This analysis showed that in patients with active RA (moderate and high disease activity), granulocytes exhibited variations in receptor expression patterns compared to non-active RA patients (those in low activity or remission). No distinct expression patterns were observed for other receptors in the remaining cell populations (Fig. 1).
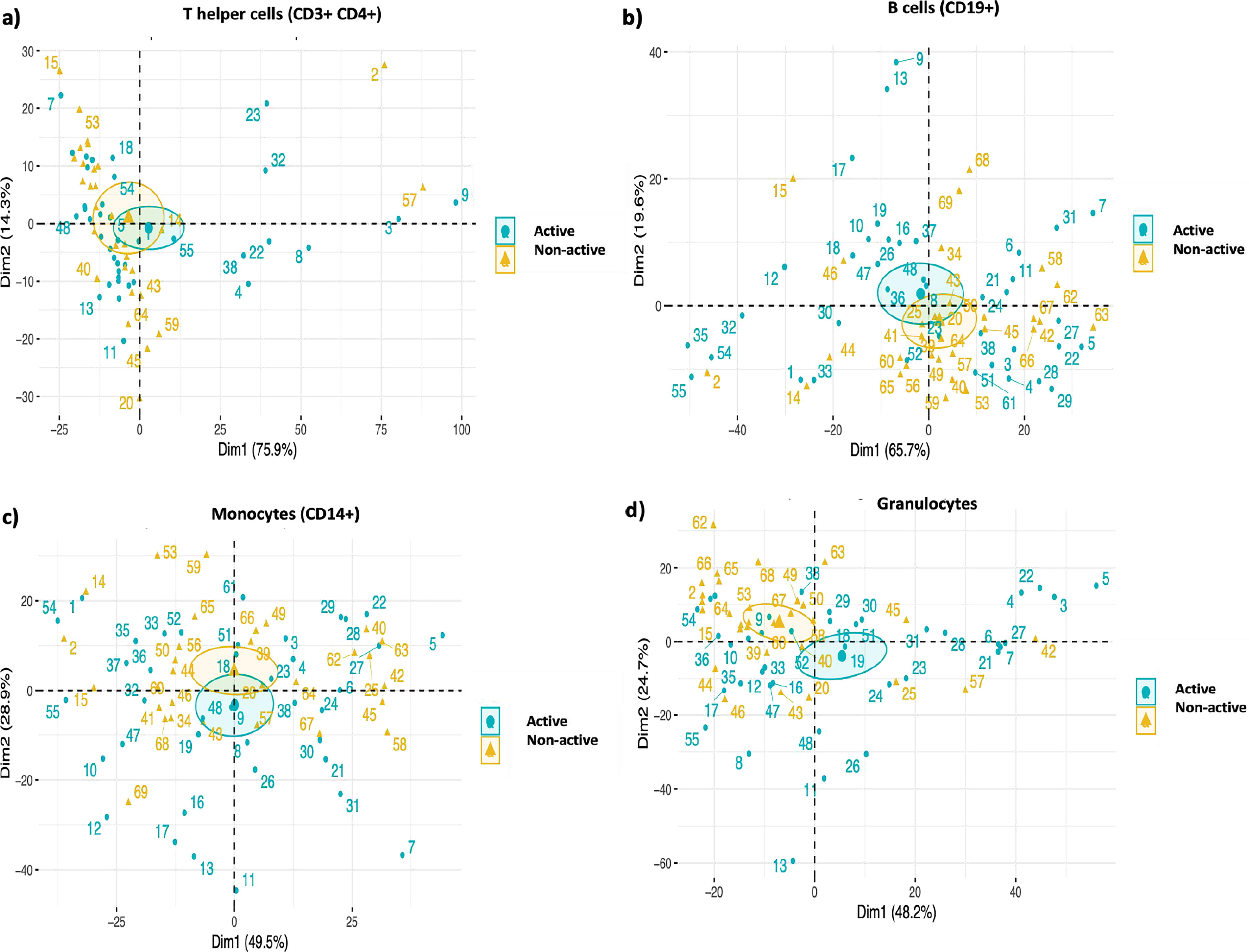
Principal component analysis (PCA) of the expression of the canonical (CD74/CD44) and non-canonical (CXCR2, 4, and 7) receptors of migration inhibitory factor (MIF) in patients with active and non-active rheumatoid arthritis (RA). PCA of CD74, CD44, CXCR2, CXCR4, and CXCR7 expression in
Serum sCD74 levels in patients with RA and CS
Serum sCD74 levels were measured in patients with RA (n = 93) and CS (n = 25). RA patients exhibited significantly higher sCD74 serum levels compared to CS [(median and range): 3080 pg/mL (1230–38860) versus 1590 pg/mL (740–39720)] (P < 0.001) (see Fig. 2, a). Furthermore, the study also examined serum sCD74 levels across different disease activity levels, including remission (n = 26), low activity (n = 12), moderate activity (n = 33), and high activity (n = 22). Patients in moderate disease activity displayed higher sCD74 levels than those in remission [4670 pg/mL (1240–25000) versus 25000 ng/mL (1230–11120)] (P < 0.01) (see Fig. 2, e). Additionally, serum sCD74 levels exhibited a positive correlation with ESR values (P < 0.01, r = 0.322) (Fig. 2, i) and DAS28-ESR (P < 0.01, r = 0.322) (see Fig. 2, j).
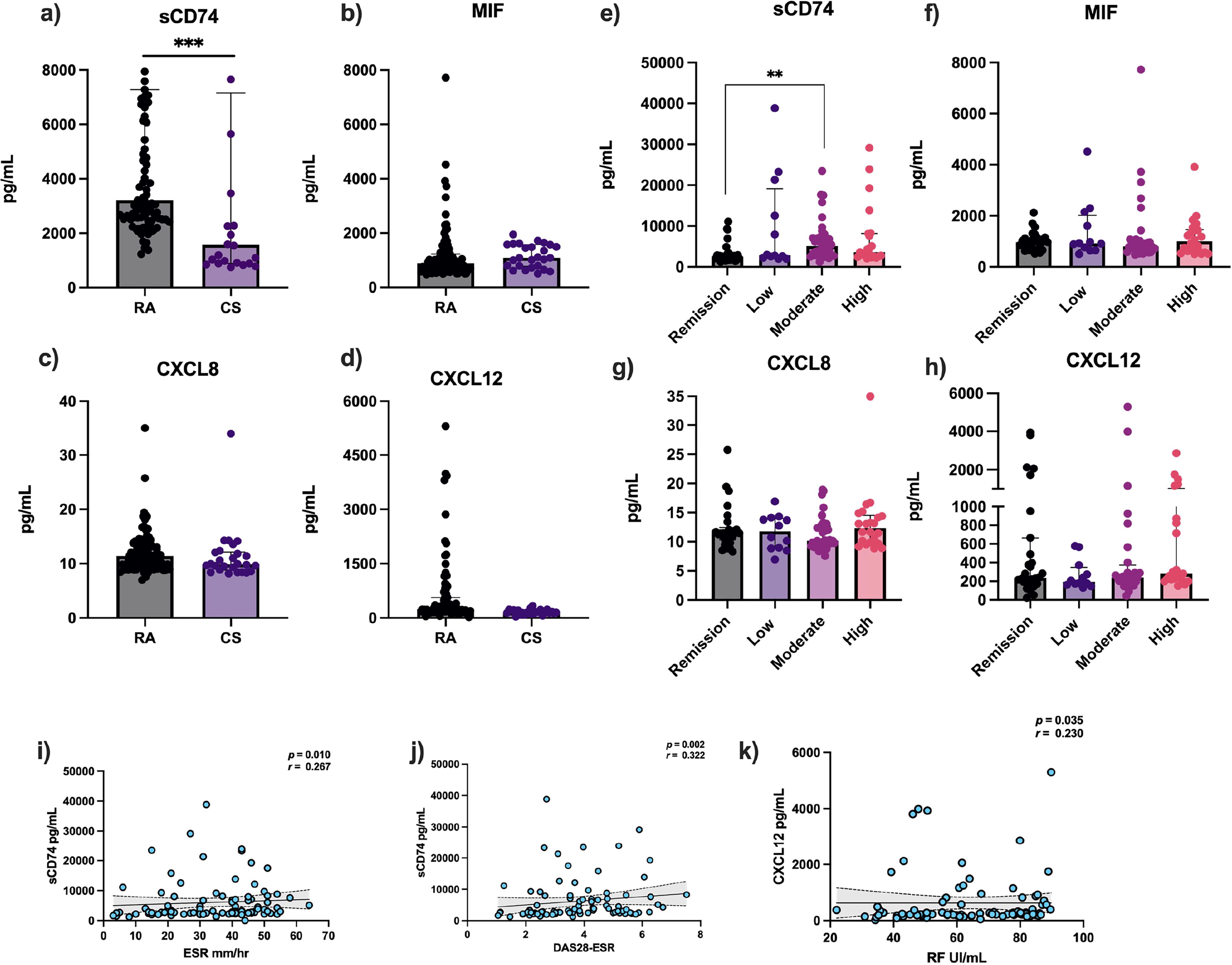
Serum levels of sCD74, MIF, TNF-α, CXCL8, and CXCL12 in patients with RA and control subjects (CS).
Serum MIF levels in patients with RA and CS
No significant differences were observed in serum MIF levels between groups (RA n = 96 versus CS n = 27) (see Fig. 2, b), nor were there significant differences when analyzed by disease activity (remission n = 26, low n = 13, moderate n = 34, and high n = 23) (P > 0.05) (see Fig. 2, f).
Serum CXCL8 levels in patients with RA and CS
Serum CXCL8 levels were higher in RA patients (n = 97) compared with CS (n = 27) [(median and range): 11.37 pg/mL (6.97–34.99) versus 9.8 pg/mL (8–33.95)] (P < 0.05) (see Fig. 2, c). However, when stratifying the analysis by disease activity groups, no significant differences were observed (P > 0.05) (see Fig. 2, g).
Serum CXCL12 levels in patients with RA and CS
Serum CXCL12 levels were quantified in patients with RA (n = 85) and CS (n = 26), revealing that RA patients exhibited higher concentrations of CXCL12 compared to CS [(median and range): 243.1 pg/mL (22.3–5299.08) versus 155.84 pg/mL (33–335.36)] (P < 0.001) (see Fig. 2, d). However, when stratifying the data by disease activity groups, including remission (n = 26), low activity (n = 12), moderate activity (n = 26), and high activity (n = 21), no significant differences were observed (P > 0.05) (see Fig. 2, h). Additionally, a positive correlation was noted between serum CXCL12 levels and RF titers (P < 0.05, r = 0.230) (see Fig. 2, k). Nonetheless, there was no statistically significant association between the membrane expression of the receptors and serum levels of CXCL12 (P > 0.05).
sCD74/MIF molar ratio in RA and CS patients
Following the methodology reported by Assis et al. (Assis et al., 2014), the molar ratio between serum sCD74 (20 kDa) and MIF (12.5 kDa) was calculated. RA patients (n = 92) exhibited higher molar ratios compared to CS (n = 24) [237.05 pg/mL (31.25–3749) versus 89.82 pg/mL (29.12–1545.79)] (P < 0.001) (see Fig. 3, a). When stratifying the data based on disease activity, the moderate activity group exhibited higher levels compared to patients in remission [307.4 pg/mL (31.25–2712.11) versus 154.15 pg/mL (60.53–1037.24)] (P < 0.05) (see Fig. 3, b).
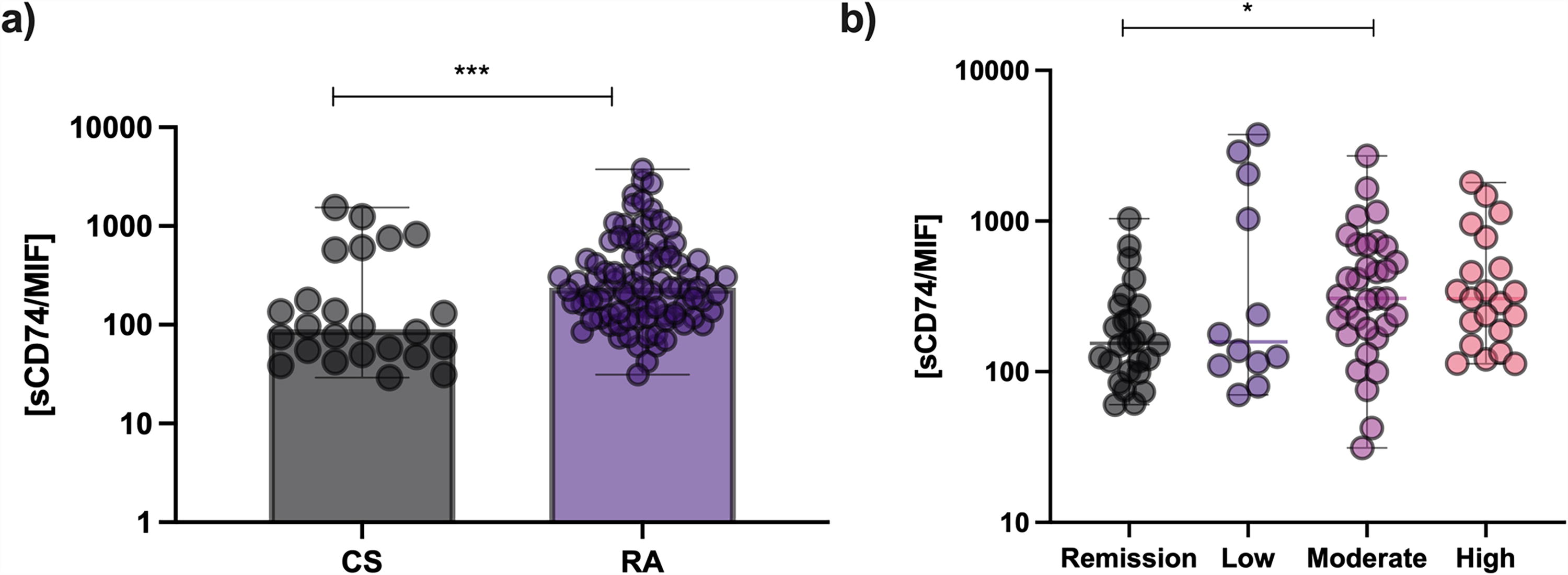
Molar sCD74/MIF relationship in patients with RA and CS. Molar sCD74/MIF relationship in patients with RA (n = 92) and CS (n = 24).
Discussion
In a previous work, we reported the expression profiles of canonical (CD74/CD44) and nonanonical (CXCR2, CXCR4, and CXCR7) MIF receptors on the membrane of immune cells in RA patients, reporting how these expressions correlate with clinical biomarkers and disease activity. Those results led us to hypothesize that sCD74, the soluble form of CD74, could act as a decoy receptor for soluble MIF, subsequently inhibiting MIF signaling through its membrane-bound counterparts. Additionally, we observed that the membrane-bound expression of CXCR4 and CXCR7 suggested that CXCR7 could act as a decoy receptor to prevent the endocytosis and degradation of CXCR4 during inflammatory conditions (Sánchez-Zuno et al., 2021). Building upon this knowledge, the main objective of the current study was to further assess the membrane expression of canonical and non-canonical MIF receptors as well as the serum levels of CXCL12 and CXCL8, which are ligands that potentially regulate receptor expression and MIF’s downstream functions. Furthermore, we also measured the soluble levels of the released MIF cognate receptor (sCD74) in the serum of RA patients.
Various studies have explored the mechanisms that generate sCD74, with evidence suggesting that SPPL2a protease cleavage of the membrane form of CD74 mediates the generation of sCD74 (Schneppenheim et al., 2013). The production of sCD74 has important implications for immune regulation and modulation of CD74 activation by binding to extra-cellular MIF, neutralizing its activity, and possibly regulating systemic MIF signaling (Schneppenheim et al., 2013; Soppert et al., 2018). Echoing our prior research (Sánchez-Zuno et al., 2021), we observed higher serum concentrations of sCD74 in RA patients compared to CS. Furthermore, within the RA group, those with moderate disease activity exhibited higher sCD74 levels than those in remission. Correspondingly, sCD74 levels positively correlated with the DAS28-ESR index score (r = 0.322) and ESR (r = 0.267). Evaluating the molar ratio between sCD74 and circulating MIF shows valuable potential as an indicator of inflammatory activity and a counter-regulatory mechanism against pathological MIF effects. Notably, our findings revealed significantly higher molar ratios in the patient group compared to the control group, and particularly higher ratios in patients with moderate disease activity compared to those in remission. Additionally, the sCD74/MIF ratio positively correlated with ESR values in RA patients. These results suggest that the sCD74/MIF molar ratio could differentiate between clinical stages of RA and potentially predict disease progression. Given that this is the first study describing this relationship in RA patients, further research involving a larger cohort of treatment-naïve patients is crucial to ascertain whether this molar ratio can serve as a potential biomarker for RA.
In our assessment of serum chemokine levels, we found higher concentrations of the canonical CXCR2 ligand, CXCL8, in patients with RA compared to CS. Consistently, previous studies have shown that both CXCL8 and MIF—key ligands of CXCR2—are elevated in the serum of RA patients (Barsante et al., 2008). Higher concentrations of these ligands can result in excessive CXCR2 activation, triggering receptor endocytosis and membrane recycling. In certain instances, overstimulation may also activate ADAM17-mediated degradation or proteolysis of CXCR2, primarily observed in granulocytes. This degradation process manifests in reduced membrane receptor levels (Mishra et al., 2015). While there is no direct evidence showing reduced CXCR2 expression specifically in RA patients, our previous study observed a trend towards lower membrane expression of CXCR2 in T cells, monocytes, and granulocytes in RA patients (Sánchez-Zuno et al., 2021). This suggests that chronic CXCR2 activation may contribute to the receptor’s downregulation in RA.
CXCR7 has been identified as a decoy receptor that binds and internalizes CXCL12, thereby indirectly modulating CXCR4 function by influencing the availability of its ligands (Koenen et al., 2019). Unlike typical G protein-coupled receptors, CXCR7 does not trigger second messenger responses upon binding to its canonical ligands, CXCL12 and CXCL11. Instead, it engages in β-arrestin-dependent signaling pathways. Upon binding its agonists, CXCR7 undergoes rapid internalization via a β-arrestin-dependent pathway and is subsequently recycled to the cell surface. Importantly, CXCR7 does not degrade after internalization but directs its ligands, such as CXCL12 and CXCL11, to lysosomes, resulting in ligand degradation (Marchese, 2014). It has also been reported that CXCR7 interaction with MIF mirrors this internalization pattern, similar to its interaction with CXCL12 (Alampour‐Rajabi et al., 2015).In our study, we observed higher levels of CXCL12 in RA patients compared to CS, and these levels were positively associated with RF titers. We hypothesize that this finding may be explained by CXCR7’s high affinity for CXCL12, which is ten times greater than that of CXCR4. By acting as a decoy receptor, CXCR7 may clear CXCL12 from the extracellular environment, thereby regulating local CXCL12 availability and reducing CXCL12/CXCR4 signaling. This action may prevent CXCR4 endocytosis in response to excessive CXCL12 concentrations, potentially leading to an upregulation of CXCR4 expression (Marchese, 2014; Piovan et al., 2018) (see Fig. 4 for the proposed mechanism).
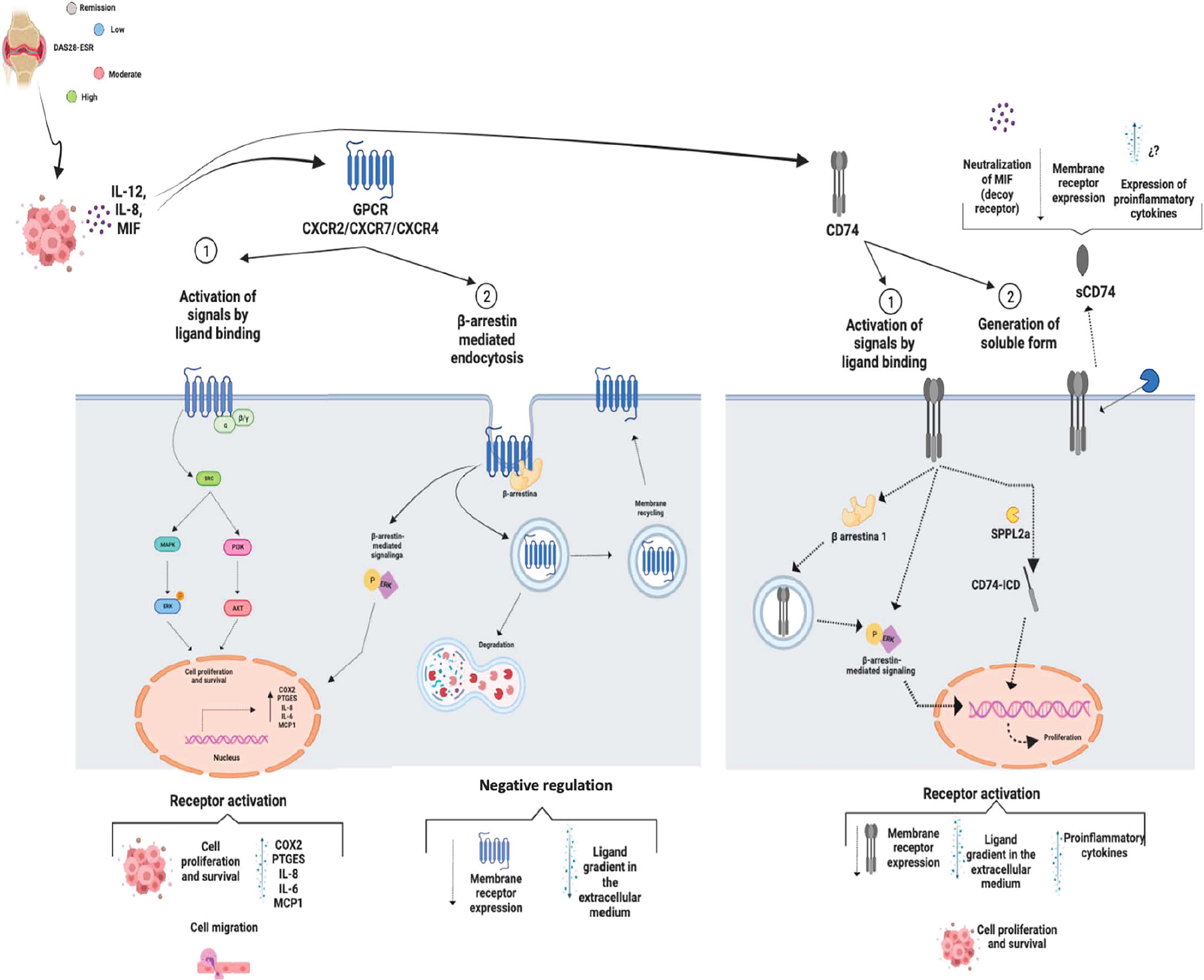
Hypothesized mechanisms of MIF and its receptors in regulating inflammation in RA. Various regulatory mechanisms, the inflammatory state, and different treatment regimens may influence the expression of both canonical and non-canonical MIF receptors, along with their respective ligands, in RA. Soluble CD74 (sCD74) may function as a decoy receptor, potentially attenuating the effects of membrane-bound receptors by modulating ligand binding.
The heterogeneity in some of our data may be attributed to the different treatment regimens among the study participants, most of whom were treated with disease-modifying anti-rheumatic drugs (DMARDs). These drugs, including methotrexate (MTX), hydroxychloroquine (HQ) and sulfasalazine (SSZ), are known to exert anti-inflammatory effects by directly or indirectly inhibiting the release of proinflammatory cytokines and chemokines (Samimi et al., 2020). In our study, a significant proportion of patients were on combined therapy, predominantly with MTX and SSZ. Despite this, our analysis did not reveal any clear associations between cytokine serum levels and specific treatment regimens, whether it was MTX monotherapy, dual DMARD therapy, or triple therapy. This indicates that while DMARDs generally suppress inflammation, their impact on individual serum cytokine levels may not directly correlate with the treatment regimen employed (data not shown).
Our study’s findings offer promising implications for clinical management of RA. The identification of higher concentrations of sCD74 in RA patients suggests a potential role for sCD74 as a novel biomarker reflecting inflammatory activity in RA. Particularly, the molar ratio between sCD74 and circulating MIF emerges as a promising indicator for predicting disease progression in RA. Additionally, the observed patterns in serum levels of the canonical CXCR2 ligand, CXCL8, provide insights into the inflammatory response in RA patients. Such insights have the potential to guide clinicians in developing more tailored and effective treatment strategies for RA patients, emphasizing the importance of a personalized approach to managing inflammatory diseases. This comprehensive understanding could further assist in how RA is monitored and treated, improving patient outcomes through more precise and targeted therapies.
While our study sheds light on crucial aspects into the role of MIF receptors and associated biomarkers in RA patients, it is essential to acknowledge certain limitations. We recognize the variability in treatment regimens among our RA patient cohort could influence cytokine levels, yet our study did not establish a clear correlation between specific treatments and the observed discrepancies. Additionally, the molar ratio between sCD74 and MIF, while promising, requires validation in larger cohorts to ascertain its reliability and effectiveness as a predictive tool for disease progression in RA. Future studies addressing these limitations are crucial to fortify the robustness and applicability of our findings, potentially leading to more precise and personalized therapeutic strategies for RA management.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethics Committee of the
Footnotes
Authors’ Contributions
Conceptualization: J.F.M.-V. Data curation: G.A.S.-Z. and J.H.-B. Funding acquisition: J.F.M.-V. Methodology: G.A.S.-Z. and C.A.P.-S. Writing—original draft, G.A.S.-Z. Writing—review and editing: R.B., J.F.M.-V., and A.M.V.-Q.
Author Disclosure Statement
The authors declare no conflict of interest.
Funding Information
This research was funded by the National Council of Science and Technology (CONACYT Ciencia Básica grant number A1-S-8774) and the Universidad de Guadalajara through Fortalecimiento de la Investigación y el Posgrado 2020 and by the NIH grants AR078334 and the Rheumatology Research Fund (RB).