
Abstract
Dysregulation of immune cells and cytokines, particularly T helper 17 (Th17) cells and their associated cytokines, is implicated in the pathogenesis of both systemic lupus erythematosus (SLE) and chronic kidney disease (CKD). This study aimed to investigate the serum levels of Th17-related cytokines (interleukin [IL]-17A, IL-21, IL-22, and IL-23) in CKD patients with and without SLE and explore their potential role in disease progression. A total of 118 participants were included, comprising 78 patients with CKD (stages 3–5) and 40 healthy controls. Cytokine levels were measured using enzyme-linked immunosorbent assay kits. Patients with CKD exhibited significantly lower IL-21 levels and higher IL-22 and IL-17A levels compared with controls, while patients with end-stage renal disease showed elevated IL-21 and IL-23 levels. Among SLE-negative nephrotic patients, IL-23 and IL-17A were significantly upregulated, whereas SLE-positive nephrotic patients had increased IL-22 and IL-17A levels. In addition, IL-21 and IL-17A were significantly correlated in patients with CKD, suggesting a potential immunoregulatory interplay. These findings indicate that Th17-related cytokines are differentially expressed depending on CKD stage and SLE status, potentially influencing immune responses, inflammation, and kidney fibrosis. Understanding alterations of these cytokines may aid in identifying targeted therapeutic, particularly for patients with CKD at risk of SLE-related complications.

Introduction
Chronic kidney disease (CKD) is characterized by long-term alterations in kidney function that can ultimately lead to kidney failure. CKD typically progresses over time, leading to a decline in the glomerular filtration rate (GFR) until it reaches end-stage renal disease (ESRD) (Faria and de Pinho, 2021). CKD is classified into five stages based on GFR and further categorized into three stages according to albuminuria (Ammirati, 2020). In this classification, ESRD represents the fifth and most severe stage of CKD. Systemic lupus erythematosus (SLE) is an autoimmune disorder characterized by the presence of autoreactive B and T lymphocytes, along with the production of a diverse range of autoantibodies and cytokines (Lou et al., 2022; Tang et al., 2019). The formation of autoimmune complexes and active inflammatory processes contribute to kidney injury, which is a common comorbidity among patients with SLE. This injury often presents as various stages of CKD, including ESRD (Mary, 2023). Lupus nephritis (LN), characterized by inflammation in different parts of renal tissue, is an underlying cause of CKD and ESRD in patients with SLE (Lichtnekert and Anders, 2024). Without appropriate treatment, LN can progress to ESRD.
The etiopathogenesis of LN remains unclear (Khoshmirsafa et al., 2019). However, evidence suggests that its development is associated with aberrant T-cell signaling and the involvement of multiple cytokines (Muhammad Yusoff et al., 2020). T helper 17 (Th17) cells, a subset of CD4-positive T cells, rely on the interleukin (IL)-21/IL-17 axis for their differentiation, maintenance of phenotype, expansion, and inflammatory responses (Seif et al., 2014, 2018). Th17 cells are implicated in the pathogenesis of various inflammatory and autoimmune disorders, including rheumatoid arthritis, psoriasis, and multiple sclerosis (Waite and Skokos, 2012). Recent findings indicate that Th17 cells are significant contributors to several inflammatory kidney injuries, such as LN and diabetic nephropathy (Basile et al., 2021). Th17 cells produce a variety of cytokines, including IL-17A, IL-17F, tumor necrosis factor-alpha, IL-21, IL-22, and IL-26 (Nalbant, 2019; Wan et al., 2023). Their involvement in inflammatory and autoimmune disorders has been well documented, particularly regarding their role in kidney injuries such as LN (Basile et al., 2021). Previous studies involving kidney patients, both with and without lupus, have shown that a wide range of cytokines, including IL-17A, are significantly elevated in patients with LN compared with patients with kidney involvement unrelated to lupus (Pacheco-Lugo et al., 2019).
The present study aimed to investigate the levels of Th17-related cytokines in patients with CKD who also have SLE. By examining the relationship between Th17 cytokines and various disease manifestations, we hope to gain insights into the role of these inflammatory mediators in the pathogenesis of kidney damage associated with SLE. Understanding these associations may contribute to better diagnostic and therapeutic strategies for managing kidney complications in patients with SLE.
Materials and Methods
Study design
This cross-sectional study investigated the serum cytokine levels in patients with CKD and SLE. A total of 118 participants were enrolled, categorized into three distinct groups based on their renal status and SLE diagnosis: 38 patients diagnosed with both CKD/ESRD and SLE (SLE-positive group), 40 patients with CKD/ESRD without SLE (SLE-negative group), and 40 healthy individuals (Control group). The stages of CKD are defined based on the estimated GFR (eGFR), which reflects how well the kidneys are functioning. The stages range from 1 to 5, with Stage 5 indicating ESRD. In Stage 3 CKD, with an eGFR of 30–59 mL/min/1.73 m2, kidney function is moderately reduced. Patients may not experience noticeable symptoms, but kidney function is significantly impaired. Some people may begin to show signs of kidney damage, such as swelling, fatigue, or changes in urination. Kidney damage is often identified through laboratory tests showing abnormal levels of protein or blood in the urine. Blood pressure management and lifestyle changes are essential at this stage. In Stage 4 CKD, with an eGFR of 15–29 mL/min/1.73 m2, there is a severe reduction in kidney function. As the kidneys become less able to filter waste, symptoms such as swelling, fatigue, and difficulty concentrating may become more pronounced. This is a critical stage where patients require closer monitoring and management. Dialysis preparation and consideration of a kidney transplant may be discussed. Finally, Stage 5 CKD (ESRD), with an eGFR of <15 mL/min/1.73 m2 or when dialysis is required, represents the final stage of CKD. At this stage, kidney function is severely impaired, and the kidneys are no longer able to filter waste products from the blood effectively. Symptoms such as nausea, vomiting, severe fatigue, and fluid retention become more pronounced. Dialysis or a kidney transplant is required to sustain life (Bauer et al., 2008). In this study, CKD is defined as stages 3 and 4 of the disease. Patients were recruited from the Nephrology Departments of Jalil Hospital in Aqqala, as well as 5th Azar and Sayad Shirazi Hospitals in Gorgan, located in northeastern Iran, between September 2022 and March 2023. Healthy controls were recruited from the general population in the surrounding areas. The study was approved by the Ethics Committee of Golestan University of Medical Sciences (IR.GOUMS.REC.1402.101). Written informed consent was obtained from all participants.
Cytokine level quantification using enzyme-linked immunosorbent assay
Blood samples were collected from all participants following the acquisition of informed consent. The serum was separated and stored at −80°C until analysis. Cytokine (IL-21, IL-22, IL-23, and IL-17A) levels were quantified in each group using commercially enzyme-linked immunosorbent assay (ELISA) kits (Mabtech, Sweden) according to the manufacturer’s instructions. The sensitivity of the ELISA kits for the detection of IL-21, IL-22, IL-23, and IL-17A was <7 pg/mL, <4pg/mL, <7 pg/mL, and 2 pg/mL, respectively. Optical density readings were taken at 450 nm using a microplate reader to determine the concentration of each cytokine.
Statistical analysis
Data analysis was conducted using SPSS software version 25.0. Descriptive statistics summarized the demographic and clinical characteristics of the participants. The normality of data distribution was assessed using the Kolmogorov–Smirnov test. To compare serum cytokine levels among the three groups, the Kruskal–Wallis test was utilized, followed by post hoc analysis using Mann–Whitney U test with Bonferroni correction for multiple comparisons. Statistical significance was defined as a P value of ≤0.05.
Results
This study provides comprehensive data on various disease groups, including those with positive and negative SLE, CKD, and ESRD. The CKD group consists of subsets of SLE-positive and SLE-negative individuals, including 31 participants. Within the SLE-positive subgroup, there are 18 individuals, accounting for 58.1% of the total SLE population. Conversely, the SLE-negative subgroup comprises 13 individuals, representing 41.9% of the SLE cases. The ESRD group includes 47 participants, with a majority of 27 individuals (57.4%) exhibiting a negative status for SLE. In addition, there are 20 participants with positive SLE status, constituting 42.6% of the CKD population. Overall, this study encompasses a total of 118 individuals across four distinct groups. Among these, the SLE group consists of 38 individuals, representing 32.2% of the total population. Both the SLE-negative and control groups were composed of 40 individuals, equating to 33.9% of the overall cases (Table 1).
Demographic and Immunological Data of Patients at the Time of the Study
GN, glomerulonephritis; LN, lupus nephritis; CKD, chronic kidney disease; ESRD, end-stage renal disease; M, male; F, female; WBC, white blood cells; IQR, range with 75th and 25th percentiles; SLE, systemic lupus erythematosus.
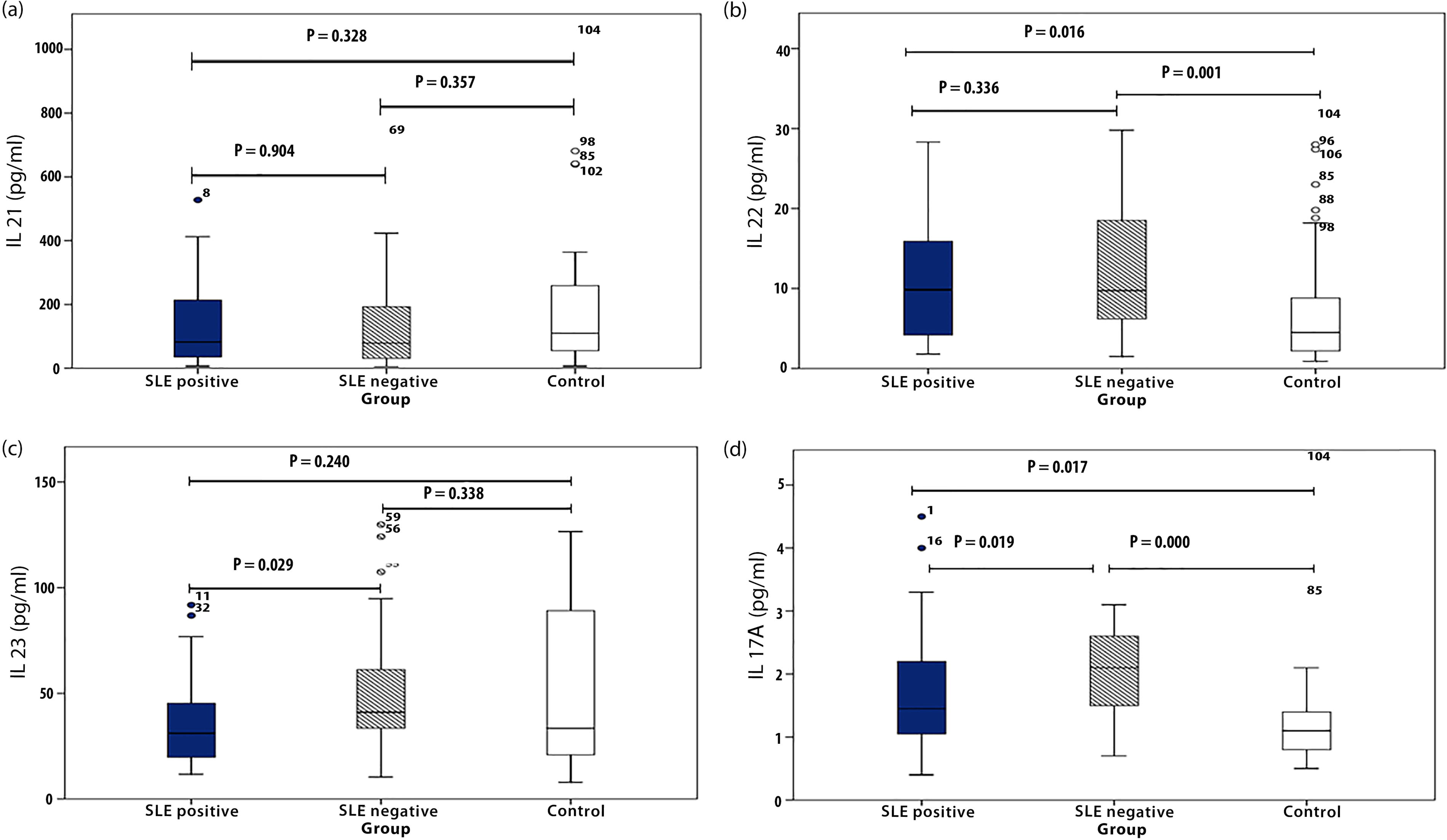
Comparison of serum concentration of IL-17A, IL-21, IL-22, and IL-23 among SLE-positive, SLE-negative, and control groups
The serum concentrations of IL-17A, IL-21, IL-22, and IL-23 across the study groups are summarized in Table 2. No significant differences were observed in serum IL-21 levels among the study groups (Fig. 1a). IL-22 levels were significantly lower in the control group compared with both SLE-positive and SLE-negative groups. However, no difference was observed in serum IL-22 concentrations between the SLE-positive and SLE-negative groups (Fig. 1b). In contrast, the SLE-negative group exhibited markedly higher serum levels of IL-23 compared with the SLE-positive patients (Fig. 1c). Furthermore, the levels of IL-17A were significantly elevated in both SLE-positive and SLE-negative patients compared with healthy individuals. Among the patients, the SLE-negative group demonstrated relatively higher levels of IL-17A compared with the SLE-positive group (Fig. 1d).
Kruskal–Wallis Test Results for Systemic Lupus Erythematosus-Positive, Systemic Lupus Erythematosus-Negative, and Control Groups
Comparison of IL-21
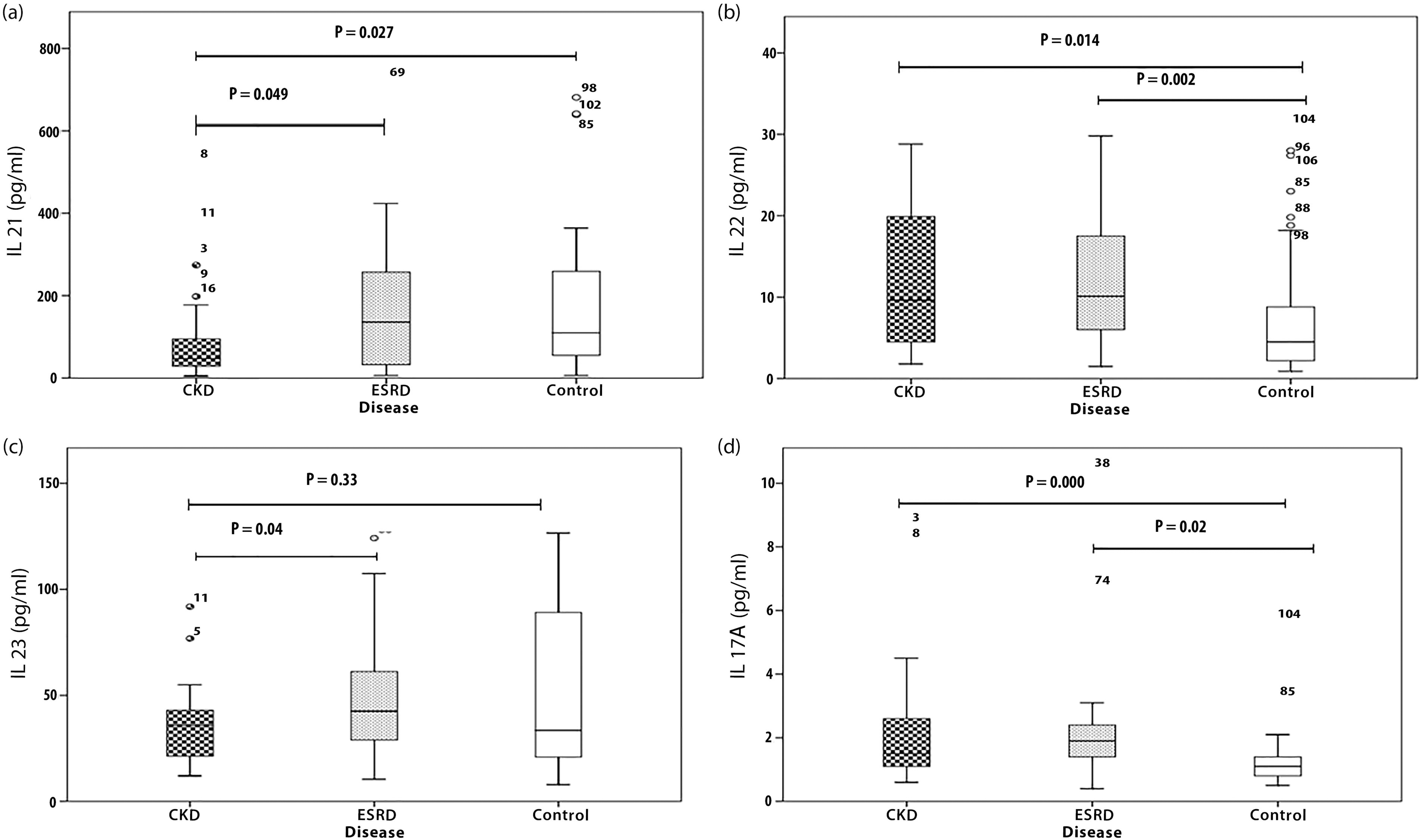
Comparison of serum levels of IL-17A, IL-21, IL-22, and IL-23 cytokines between patients with CKD and ESRD
The serum levels of the Th17 family of cytokines, including IL-17A, IL-21, IL-22, and IL-23, were compared between patients with CKD and ESRD and the control group (Table 3). The analysis revealed that IL-21 and IL-23 levels were significantly elevated in the ESRD group (P = 0.049 and 0.04, respectively). When comparing patients with CKD to controls, both IL-22 and IL-17A levels were significantly higher in the CKD group (P = 0.027 and 0.020, respectively), while IL-21 levels were significantly lower in patients (P = 0.027). In addition, when comparing patients with ESRD to controls, both IL-22 and IL-17A concentrations were significantly higher in patients with ESRD (P = 0.002 and 0.000, respectively) (Fig. 2).
Results of the Comparison of Th17-Related Cytokines Between Patients with Chronic Kidney Disease and End-Stage Renal Disease, as Well as Comparing Them Between the Patients and the Controls
P-values of less than 0.05 are statistically significant.
Comparison of serum levels of IL-21
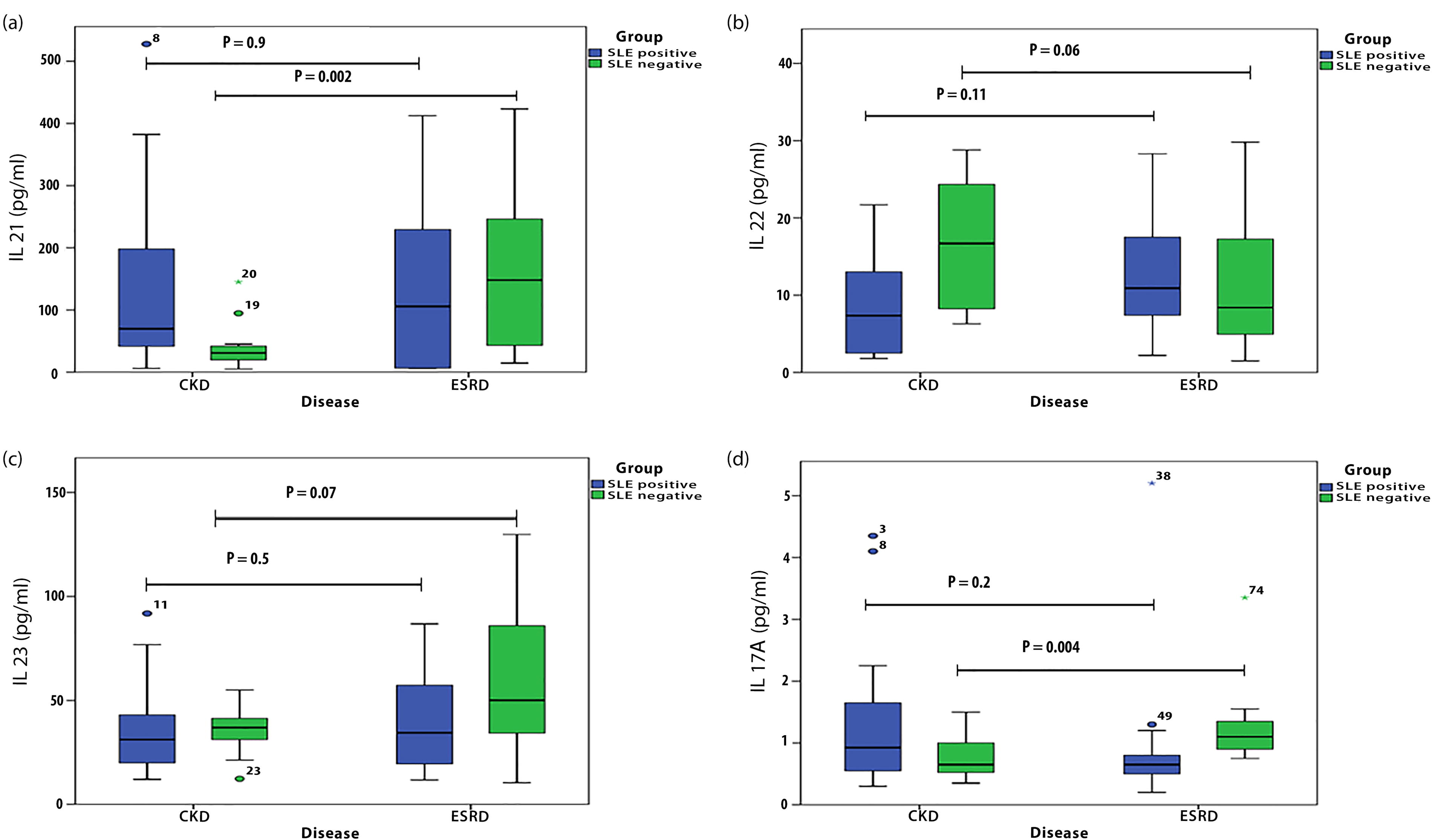
Comparison of serum concentrations of IL-17A, IL-21, IL-22, and IL-23 cytokines between the patients with CKD and ESRD among SLE-positive and SLE-negative groups
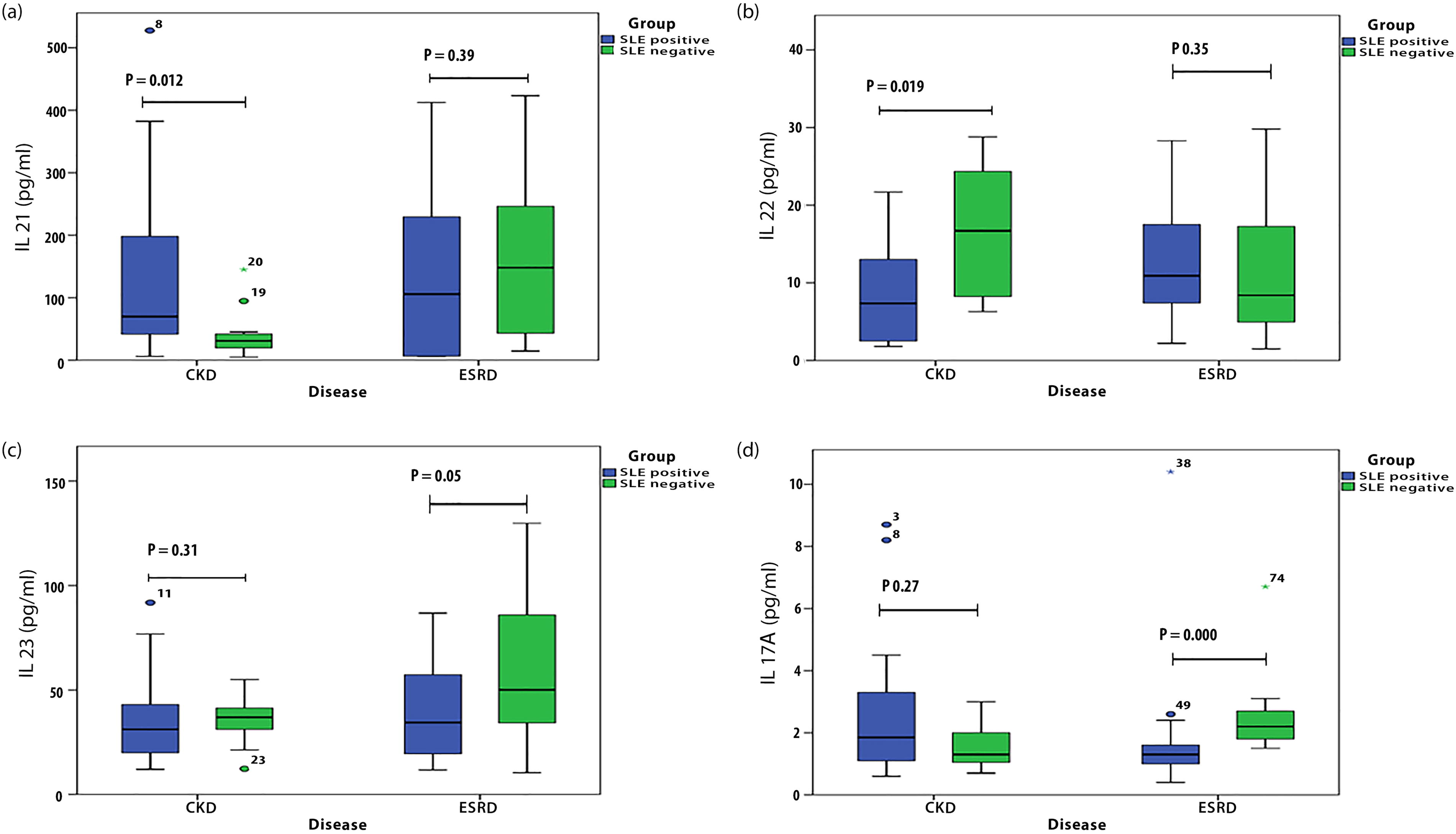
This analysis focused on the comparison of Th17 family cytokines between patients with CKD and ESRD, considering the presence or absence of SLE. In SLE-negative patients, IL-21 levels were significantly higher in the ESRD group compared with the CKD group (P = 0.02) (Fig. 3a). Conversely, IL-22 levels showed a significant reduction in patients with ESRD compared with patients with CKD within the same SLE-negative patients (Fig. 3b). In SLE-positive patients, IL-23 levels were significantly upregulated in patients with ESRD compared with patients with CKD (P = 0.05), while other cytokines—IL-21, IL-22, and IL-17A—did not show statistically significant differences (Fig. 3c). Notably, IL-17A was significantly elevated in patients with ESRD compared with the patients with CKD among SLE-negative cases (Fig. 3d). Moreover, the results indicated a significant elevation in IL-21 levels in patients with CKD with SLE compared with those without SLE (P = 0.012) (Fig. 4a). In addition, IL-22 concentrations were significantly higher among patients with CKD without SLE compared with those with SLE (P = 0.019) (Fig. 4b). This study also demonstrated significantly elevated levels of IL-23 (Fig. 4c) and IL-17A (Fig. 4d) in SLE-positive patients compared with patients with ESRD without SLE (P = 0.05 and 0.000, respectively). In addition, within the CKD group, a significant correlation was observed between IL-21 and IL-17A (Fig. 5). This suggests a potential interaction in disease progression. No significant correlation was observed among cytokines and clinical parameters (data not shown).
Comparison of IL-21, IL-22, IL-23, and IL-17A concentrations between patients with CKD and ESRD among SLE-negative and SLE-positive cases.
Variation in concentrations of IL21, IL-22, IL23, and IL-17A between patients with CKD and ESRD among SLE-negative and SLE-positive cases.
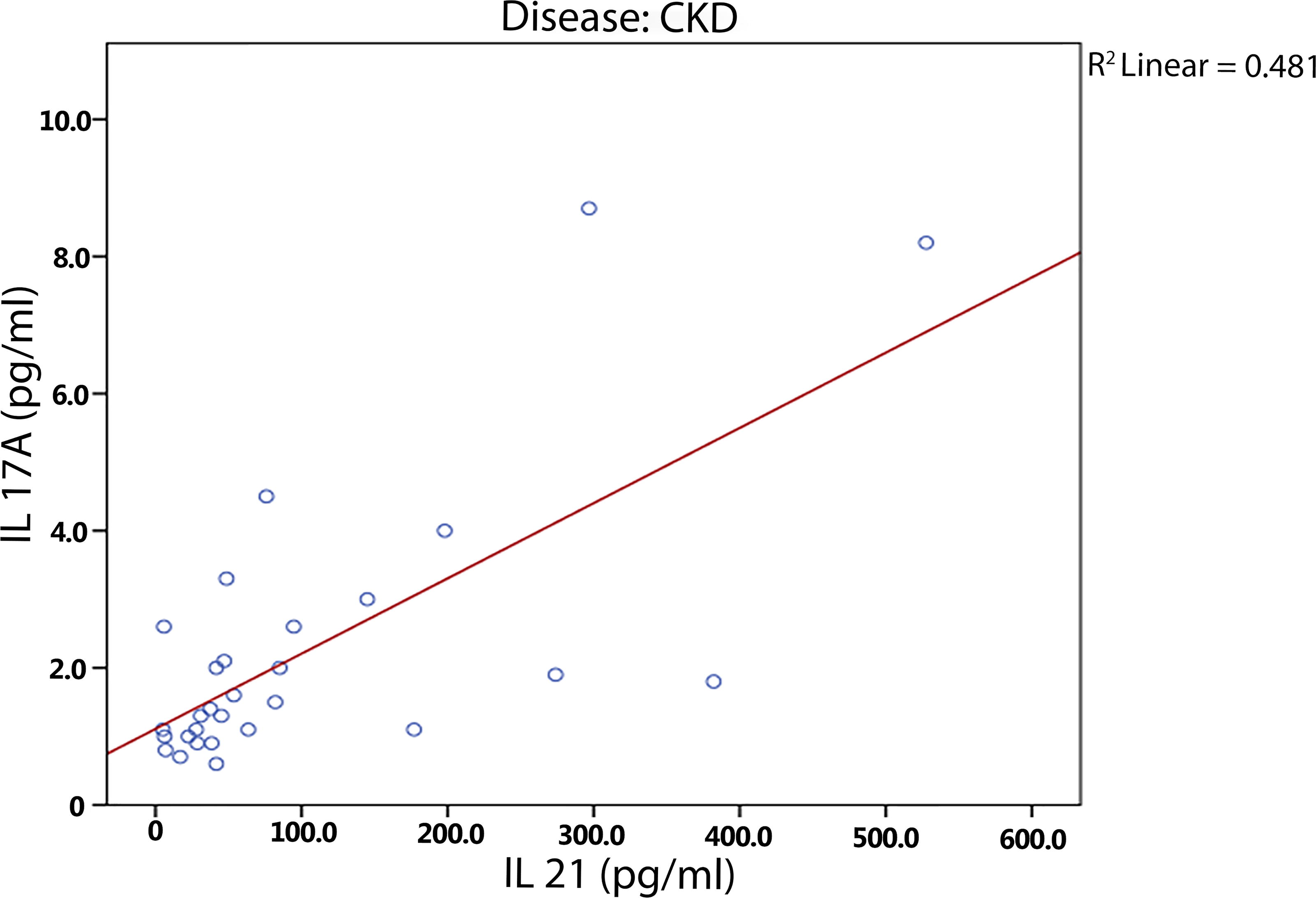
Correlation between IL-17A and IL-21 levels in the CKD group.
Discussion
This study found that IL-21 levels were lower in patients with CKD but increased in ESRD, while IL-22 and IL-17A were elevated in both groups. The IL-23/IL-17 axis was more active in SLE-negative patients, suggesting a potential protective role against SLE. In contrast, SLE-positive patients showed higher IL-22 and IL-17A levels, indicating Th17 activation in inflammation. In addition, IL-23 was significantly upregulated in ESRD compared with CKD, highlighting its role in disease progression and inflammation.
Compared with healthy individuals, IL-21 was significantly lower in patients with CKD, while IL-22 was significantly higher, along with increased IL-17A. Since these cytokines function in a shared pathway downstream of Th17 cell activation, IL-21 was also expected to be higher in the patient group. It is highly unlikely that the reduced concentration of IL-21 was due to the medications used by the patients since the same effect was not observed in the other cytokines. In line with our data, Krystyna Pawlak and others demonstrated that the plasma concentration of IL-21 in hemodialyzed patients was approximately half that of healthy individuals. Also it was observed that among the patients, higher IL-21 was associated with glomerulonephritis (Pawlak et al., 2011).
It seems that the lower IL-21 levels in patients with CKD could compromise their immune system since this cytokine is involved in multiple aspects of immune functions in both the innate and adaptive arms of the immune system (Spolski and Leonard, 2014). At the same time, the lower concentration of this cytokine in patients with CKD could increase their chance of developing autoimmune responses due to its ability to modulate the immune responses; in fact, CKD is commonly pursued by SLE as observed in the clinical setting (Long et al., 2019). On the other hand, elevated levels of IL-22 in patients with CKD could be indicative of the dynamic epithelium resistance to chronic inflammation and injury or it can be a contributing factor to the inflammatory response within the renal tissue (Ma et al., 2022). Conversely, in patients with ESRD, IL-21 was observed to be slightly elevated compared with the controls; maybe this observation is due to the dual immunomodulatory/inflammatory existence of IL-21 such that in the lower stages of CKD, it tends to be lower and contributes to a limited immune response but with the progression of the disease toward later stages with higher injury and inflammation, this cytokine rises to counterbalance the inflammation. Consistent with our data, Kyoung Woon Kim and others assessed B cell profiles among the patients with ESRD and found a slight elevation of IL-21 in the predialysis patients with ESRD (Kim et al., 2012).
It was observed that IL-23 was significantly elevated in SLE-negative nephrotic patients; besides IL-17A was significantly increased in this study group as well, indicating that both the inducer and the effector cytokine of Th-17 cells known as IL-23/IL-17 axis are actively functioning in the SLE-negative patients and this might be suggestive of a protective role of this axis in the patients with CKD/ESRD in the prevention of developing SLE. Although it was expected to obtain a different result where the IL-23/IL-17 would be higher in SLE-positive patients, this paradoxical event could also be explained by the fact that the SLE-positive patients would typically receive heavier anti-inflammatory treatments in comparison with the SLE-negative nephrotic patients. On the other hand, it was found that in comparison between the control group and the SLE-positive nephrotic patients, IL-22 and IL-17A were higher in the SLE-positive patients. This demonstrates that in this subset of patients Th17 cells are active and could contribute to the inflammatory responses observed in the SLE-positive nephrotic patients.
Increased expression of IL-22 has been described in the serum of patients with SLE without renal involvement. However, in patients with LN, serum IL-22 expression was reported to be downregulated, which is contrary to our findings, showing that patients with SLE tend to have higher serum IL-22 (Ahmed et al., 2022; Haouami et al., 2018; Haroon et al., 2023; Paust et al., 2009; Zhang et al., 2009). Also, we compared the Th17 cytokine profile between controls and SLE-negative patients and it was found that IL-22 and IL-17A were significantly elevated in the nephrotic SLE-negative patients. This further explains that nephrotic patients have higher levels of IL-17A and IL-22 compared with the controls. However, these cytokines are found in higher concentrations in SLE-negative subsets, which might seem contradictory to the assumption that in patients with SLE the Th17 axis is more active. Although several studies also have reported decreased serum IL-22 in patients with LN (Mary, 2023; Pan et al., 2009). Also it was shown that the number of IL-22-producing T cells is significantly reduced in patients with SLE as compared with the controls (Dolff et al., 2019). Further analysis revealed that in comparison between the CKD and the patients with ESRD, IL-23 as the inducer of the Th17 cells was upregulated in patients with ESRD. This suggests that inflammatory cells such as dendritic cells and macrophages are responsible for secreting IL-23. This cytokine serves as a bridge for linking the innate immune responses and the adaptive immune responses, which increase in activity with the progression of the disease toward higher stages.
We further subdivided the study groups and evaluated the Th17 profile of patients with CKD and ESRD who were either SLE-positive or negative. It was observed that there was no significant difference between the patients with CKD and ESRD in the SLE-positive group, while in the SLE-negative group, the IL-21 and IL-17A were significantly increased in patients with ESRD. Furthermore, comparing the results between the SLE-negative and positive patients in the CKD group showed that in the SLE-negative patients, IL-22 was upregulated, while in the SLE-positive group, IL-21 was significantly elevated. In addition, IL-17A was shown to be upregulated in patients with ESRD who were SLE-negative. For further assessment of the data, a series of Spearman correlation tests were performed to elucidate any association between various tested parameters in different conditions. Correlation studies of the tested Th17 cytokines in whole patient data revealed that IL-22 strongly correlated with IL-8, CCL2, CCL20, as well as CXCL10. Moreover, IL-23 strongly correlated with CCL2 and CCL5; IL-17A correlated with IL-8, CCL2, and CCL20. For a better understanding of the correlation results, data were categorized into subgroups of CKD, ESRD, SLE-positive, and SLE-negative. It was found that in the CKD group, IL-21 significantly correlated with IL-17A, and IL-22 significantly correlated with CCL20.
In the ESRD group, it was observed that IL-21 correlated with IL-17, IL-23 significantly correlated with CCL20 and CXCL10, and IL-17 significantly correlated with IL-8 and CCL2. In another correlation analysis, the patients were categorized into two individual groups of SLE-positive and SLE-negative. Accordingly, it was found that in the SLE-positive group, IL-17A significantly correlated with IL-21, while in the SLE-positive group, IL-21 significantly correlated with IL-8; IL-22 significantly correlated with CXCL1; IL-23 significantly correlated with CXCL1; and IL-17A significantly correlated with IL-8. Further Spearman’s correlation analyses were performed in subgroups of patients with CKD and ESRD who were also SLE-positive and, patients with CKD and ESRD who were SLE-negative; no significant correlation was found in the first group, whereas in the second group, significant correlations were found between IL-21 and CCL2, as well as between IL-22 and CCL2 in CKD/SLE-negative group. Also, in the ESRD/SLE-negative group, IL-22 significantly correlated with IL-17; IL-23 significantly correlated with CXCL10; and IL-17A significantly correlated with IL-8 and CCL20. Overall, these correlation analyses could indicate that the Th17 cytokines contribute to the pathogenesis of nephritis by impacting the chemokines necessary for the recruitment of neutrophils and macrophages to the kidney injury sites. This study has some limitations, including a relatively small sample size, which may affect the generalizability of the findings. In addition, the cross-sectional design prevents establishing causal relationships between cytokine levels and disease progression. The potential influence of medications and comorbidities on cytokine expression was not fully accounted for, which may have impacted the results. Future studies with larger cohorts and longitudinal follow-ups are needed to validate these findings and explore the mechanistic role of Th17 cytokines in CKD and ESRD.
Conclusion
This study highlights the critical role of Th17-related cytokines in CKD and ESRD, especially in association with disease progression and the presence of SLE. The findings suggest that IL-21, IL-22, IL-17A, and IL-23 are differentially regulated in CKD and ESRD, with IL-21 being lower in CKD but increasing in ESRD, while IL-22 and IL-17A were consistently elevated in both conditions. The upregulation of IL-23 in ESRD suggests its involvement in advancing renal dysfunction. In addition, the observed differences in cytokine expression between SLE-positive and SLE-negative patients imply distinct inflammatory pathways that may influence disease manifestation and severity. Clinically, these findings emphasize the potential utility of Th17 cytokines as biomarkers for monitoring CKD progression and identifying patients at higher risk for ESRD. Furthermore, targeting IL-23 and IL-17A pathways could provide new therapeutic avenues for managing renal inflammation and preventing disease exacerbation, particularly in patients with immune-related complications such as SLE. Future studies should explore the therapeutic modulation of these cytokines to improve outcomes in patients with CKD and ESRD.
Footnotes
Acknowledgment
The authors extend their grateful gratitude to Alejalil Hospital from Golestan University of Medical Sciences for their invaluable support. The authors also deeply appreciate the voluntary participation and cooperation of all the patients involved in this study.
Authors’ Contributions
K.H.K. and Y.B.: Conceptualization. S.G. and P.B.: Formal analysis. K.H.K. and A.M.: Investigation. Y.B. and S.S.: Methodology. K.H.K. and M.A.: Project administration. Y.B.: Supervision. F.S. and Y.B.: Validation. K.H.K. and P.B.: Writing—original draft. F.S. and H.D.: Writing—review and editing.
Ethical Considerations
The research conducted in this study adhered to the principles outlined in the Declaration of Helsinki and was approved by the Ethics Committee of Golestan University of Medical Sciences (Ethical code No. IR.GOUMS.REC.1402.01). Before any intervention, all participants provided written informed consent. The authors have fully complied with ethical issues, such as plagiarism, data fabrication, and double publication.
Ethics Approval and Consent to Participate
The study was approved by the Ethics Committee of Golestan University of Medical Sciences (IR.GOUMS.REC.1402.101). Informed written consent was obtained from all participants.
Availability of Data and Material
Please get in touch with the corresponding author for data requests.
Author Disclosure Statement
The authors declared no conflict of interest.
Funding Information
This study received no funds or grant. This research received no specific grant, funding, equipment or supplies from any funding agency in the public, commercial, or not-for-profit sectors.