
Abstract
Purpose:
To determine the effectiveness of topically applied besifloxacin, gatifloxacin, and moxifloxacin for the early treatment of experimental methicillin-resistant Staphylococcus aureus (MRSA) keratitis.
Methods:
Ten hours post-MRSA infection, rabbit eyes were treated topically with 19 doses of phosphate-buffered saline (PBS), besifloxacin, gatifloxacin, or moxifloxacin. Slit-lamp examinations were performed before and after the inoculation. Corneas were harvested for bacterial quantitation and minimal inhibitory concentrations (MICs) were determined.
Results:
All 3 fluoroquinolones significantly lowered the clinical severity of the infection as compared to treatment with PBS (P < 0.05). However, the mean log10 colony-forming unit (CFU) recovered from besifloxacin-treated corneas was significantly lower than all other treatment groups (P < 0.01). CFU recovered from corneas treated with moxifloxacin and PBS showed no significant difference (P = 0.12). Corneas treated with gatifloxacin had a significantly lower log10 CFU recovered as compared to PBS-treated corneas (P < 0.01). The MICs for gatifloxacin and moxifloxacin were 8 μg/mL, whereas the MIC for besifloxacin was 1 μg/mL.
Conclusions:
All 3 fluoroquinolones significantly lowered the clinical severity of the infection. Besifloxacin had an 8-fold lower MIC for MRSA than gatifloxacin and moxifloxacin, and was significantly more effective than gatifloxacin and moxifloxacin in reducing the number of MRSA in the rabbit cornea.
Introduction
S
Methicillin-resistant strains of S. aureus have about 30–50 kb more chromosomal DNA (mec) than susceptible strains.7 This region of DNA contains genes that aid in the ability of the bacterium to evade killing by the β-lactam class of drugs.8 In addition, MRSA has become increasingly resistant to certain fluoroquinolones.9–11 Fluoroquinolones are able to kill bacteria by inhibiting bacterial DNA synthesis. This inhibition is achieved by interfering with DNA gyrase and topoisomerase IV interaction with DNA, thus inhibiting bacterial DNA replication and transcription.12 Resistant bacteria are able to evade the drug through nucleotide changes in the gyrase and/or topoisomerase IV genes or by an efflux pump.13 In 2006, Rhee and colleagues observed 5 patients with MRSA keratitis and found that the bacteria recovered in all 5 cases were resistant to fluoroquinolones.14 Other studies have grown staphylococci in subinhibitory amounts of quinolones.15,16 These studies have demonstrated that these growth conditions can lead to resistance in vitro.
Besifloxacin is a novel fluoroquinolone for topical ophthalmic use recently approved by by the United States Food and Drug for the treatment Administration of bacterial conjunctivitis. Besifloxacin appears to have a broad spectrum of activity against aerobic and anaerobic bacteria, possibly due to its cyclopropyl group and chloride substituent at C-8 improving its activity against DNA gyrase and topoisomerase IV enzymes. Besifloxacin has been shown to be active against Gram-positive (S. aureus, Staphylococcus epidermidis, Streptococcus pneumoniae, Streptococcus pyogenes, Corynebacterium species, and Propionibacterium acnes), Gram-negative organisms (Haemophilus influenzae, Moraxella species, Klebsiella pneumoniae, Escherichia coli, Neisseria gonorrhoeae, and Pseudomonas aeruginosa), and several resistant isolates such as ciprofloxacin- and/or MRSA, methicillin-resistant S. epidermidis, penicillin-resistant S. pneumoniae, and ampicillin-resistant H. influenzae.17
S. aureus keratitis is commonly examined in vivo in the New Zealand white rabbit.18,19 The rabbit eye is large and similar to that of a human eye, making it an appropriate model for keratitis. The current study examined MRSA keratitis in the rabbit using a MRSA strain isolated from the blood of a patient at the V.A. Medical Center in Jackson, MS, USA. A previous study examined the effect of treatment from 16 to 24 h postinfection and demonstrated that besifloxacin was significantly more effective than gatifloxacin and moxifloxacin in reducing the bacterial load in the cornea.20 However, none of the treatment compounds reduced clinical severity scores when compared to the phosphate-buffered saline (PBS) control. The current study determined the effectiveness of topical eye drop administration of 3 fluoroquinolones from 10 to 18 h postinfection in treating MRSA keratitis. The purpose of examining an earlier treatment regimen was to determine whether early intervention could reduce the clinical severity of MRSA keratitis.
Methods
Bacterial cultures
The MRSA strain used was isolated from the blood of a patient at the V.A. Medical Center in Jackson, MS. A frozen stock was streaked for isolation of colonies onto tryptic soy agar (TSA) and incubated overnight at 37°C. Several isolated colonies were inoculated into 10-mL tryptic soy broth (TSB) and incubated for 18–22 h at 37°C and 200 rpm in a shaking air incubator. This culture was diluted 1:100 in TSB and incubated for ~2 h at 37°C and 200 rpm in a shaking air incubator until the optical density of the culture was A600 = 0.2. Serial 10-fold dilutions of this logarithmic-phase culture were made in TSB. The 10−4 dilution, equivalent to 100 colony-forming units (CFU) per 10 μL, was used for corneal infection of rabbits. Accuracy of the inoculum was verified by plating 0.1 mL of each serial 10-fold dilution in triplicate on TSA.
Corneal infection of rabbits
Rabbits were maintained according to the ARVO Statement for the Use of Animals in Ophthalmic and Vision Research and the guidelines of the University of Mississippi Medical Center Institutional Animal Care and Use Committee (IACUC). Specific pathogen-free New Zealand white rabbits, 2–3 kg and of either sex, were used (Harlan Laboratories, Inc., Indianapolis, IN).. Each rabbit was systemically anesthetized by an intramuscular injection of a mixture of xylazine (100 mg/mL; Butler Company, Columbus, OH) and ketamine hydrochloride (100 mg/mL; Butler Company, Columbus, OH; 50:10 mg/kg). One to two drops of 0.5% proparacaine (Bausch & Lomb, Tampa, FL) were applied to each eye for topical anesthesia. Each eye was held steady with clamping forceps, and 10 μL of MRSA (102 CFU) was injected directly within the corneal stroma with a 30-gauge needle on a 0.1-mL gas-tight syringe. This study was repeated and data from both experiments were averaged.
Examination and scoring of rabbit eyes
Eyes were examined by 2 masked observers at 9 h (pretreatment) and 19 h (posttreatment) after infection. Seven parameters were assessed to determine the severity of the infection: injection, chemosis, iritis, corneal infiltrate, corneal edema, fibrin, and hypopyon.21 Each parameter was given a grade of 0 (normal) to 4 (maximally severe) by each observer, and the 7 grades were added to achieve a total score with a theoretical maximum of 28. The first 3 parameters—injection, chemosis, and iritis—were graded without the use of a slit-lamp microscope. The final score for each eye was calculated by totaling the scores of the 2 observers and dividing by 2. At 9 and 19 h postinfection (PI), each eye was stained with fluorescein to aid in measuring corneal epithelial erosions.
Treatment regimen
Treatment commenced 10 h PI immediately following the examination and scoring. The rabbits were divided into 4 treatment groups by an investigator that was not involved in the examination and scoring. The treatment groups were sterile PBS (control), gatifloxacin (Zymar, 3 mg/mL; Allergan, Irvine, CA), moxifloxacin (Vigamox, 5 mg/mL; Alcon, Fort Worth, TX), and besifloxacin (6 mg/mL; Bausch & Lomb, Tampa, FL). Antibiotics were used in their commercially available formulations, and the bottles used for treatment were masked so that the administrators of the drugs were not aware of which drug was used for each treatment group. One drop was placed on each eye every 15 min for 5 doses and then every 30 min for 14 doses (19 total doses over 8 h).
Euthanasia and tissue harvest
For quantitation of baseline CFU per cornea, rabbits were euthanized with an intravenous overdose of sodium pentobarbital (100 mg/kg; Sigma-Aldrich, St. Louis, MO) at 9 h PI. In addition, another set of animals were euthanized at 19 h PI to evaluate the effect of the treatments and to conduct the final examination. Each cornea was harvested, homogenized, serially diluted in sterile PBS, and plated in triplicate on TSA. Plates were incubated overnight at 37°C, and colonies were counted.
Both eyes of one rabbit from each treatment group were removed at 19 h PI for histology. Whole eyes were excised and histology was performed by Excalibur Pathology (Moore, OK).
Minimal inhibitory concentration assays
The minimal inhibitory concentrations (MICs) of gatifloxacin, moxifloxacin, and besifloxacin against the MRSA strain were determined using the macrodilution broth method according to the Clinical and Laboratory Standards Institute (2006).22 The MIC for each antibiotic was determined to be the lowest concentration at which no turbidity was observed, taking into account the final 2-fold dilution of each antibiotic when the bacterial suspension was added.
Statistical analysis
Data were analyzed using the Statistical Analysis System (SAS) program for computers (Cary, NC). Clinical scores were analyzed using a nonparametric one-way analysis of variance, an analysis that has been used extensively and deemed appropriate for the comparison of clinical scores. Bacterial loads were analyzed using the General Linear Models Procedure of Least Squares Means with a Bonferroni adjustment for multiple comparisons, which has been reported as an appropriate analysis for comparisons of bacterial CFU.23 A P value < 0.05 was considered significant.
Results
Rabbit keratitis model
All results were calculated from the data of 2 separate experiments that yielded similar results. Although rabbits were randomly assigned to groups at 10 h PI and prior to treatment, statistics on the 9-h clinical scores were performed after the experiment to verify that each group had similar scores prior to treatment. There were no significant differences in scores when besifloxacin, gatifloxacin, moxifloxacin, and PBS grouped rabbits were compared (Table 1; P ≥ 0.11). Similarly, no differences were observed between groups when looking at the average erosion size (Table 1). Figure 1 shows representative eyes at 9 h PI, before treatment.
M
Abbreviations: PBS, phosphate-buffered saline; SLE, slit-lamp examination.
∗ ± Standard errors of the means.
∗∗ SLE score 19 h PI significantly lower than PBS-treated eyes.
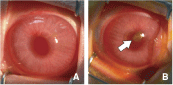
Eyes at 9 h postinfection (pretreatment). Both eyes were representative of all eyes prior to treatment. Erosions were stained with fluorescein for ease of visualization. (
Following treatment (19 h PI), besifloxacin, gatifloxacin, and moxifloxacin caused a significant reduction in clinical scores compared to the PBS control (Table 1; P ≤ 0.01). The clinical scores from the 3 treatment groups were not significantly different from each other (P ≥ 0.35; Table 1). The average erosion size for each group at this time point were as follows: besifloxacin 1.8 mm, gatifloxacin 1.9 mm, moxifloxacin 2.3 mm, and PBS 1.9 mm. Average erosion size seemed to slightly improve with treatment with besifloxacin, gatifloxacin, and PBS by 19 h PI; however, these differences were not statistically significant. Figure 2 shows representative eyes from each treatment group 19 h PI. Corneal ulceration and edema was generally more severe in the PBS-treated eyes as compared to the fluoroquinolone-treated eyes (Fig. 2).

Eyes at 19 h postinfection (posttreatment). Erosions were stained with fluorescein for ease of visualization. Arrow indicates corneal ulcer. Abbreviation: phosphate-buffered saline (PBS)
Corneal CFU recovery
The gatifloxacin and besifloxacin treatment groups had significantly lower CFU recovered from corneas compared to the PBS control group (Table 2; P < 0.01). Moxifloxacin did not significantly reduce the corneal CFU compared to PBS (Table 2; P = 0.12). The besifloxacin treatment group had significantly reduced CFU recovered from corneas compared to the gatifloxacin and moxifloxacin groups (Table 2; P < 0.01).
M
Abbreviations: CFU, colony-forming unit; PBS, phosphate-buffered saline.
∗ Significantly lower than PBS- and moxifloxacin-treated corneas.
∗∗ Significantly lower than PBS-, moxifloxacin-, and gatifloxacin-treated corneas.
Histopathology
Eyes from each group were randomly chosen for histopathology at 19 h postinfection. PBS- (Fig. 3A) and gatifloxacin-treated (Fig. 3C) corneas exhibited severe edema, whereas moxifloxacin-treated corneas (Fig. 3E) had only slight edema, and besifloxacin-treated corneas (Fig. 3G) had moderate edema as shown by swelling of the corneal stroma. Erosion of the epithelium was evident in all groups (small arrows in Fig. 3A, 3C, 3E, and 3G). Polymorphonuclear cell (PMN) infiltration was less severe in the anterior chambers of the gatifloxacin-, moxifloxacin-, and besifloxacin-treated eyes (small arrows in Fig. 3D, 3F, and 3H) as compared to the PBS-treated eyes (Fig. 3B).
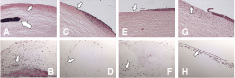
Histology of (
MICs
The MICs for gatifloxacin and moxifloxacin against the MRSA strain were 8 μg/mL for both fluoroquinolones. The MIC for besifloxacin was 1 μg/mL.
Discussion
This study tested the efficacy of topical besifloxacin in comparison with gatifloxacin, moxifloxacin, and a PBS control in the early treatment (10–18 h postinfection) of MRSA keratitis. Besifloxacin treatment was equally effective in reducing the clinical scores of rabbit eyes compared to the other treatments. Moreover, besifloxacin significantly reduced the CFU recovered from corneas compared to the control (reduction of ~3.8 log CFU). The reduction caused by gatifloxacin and moxifloxacin, in contrast, was only ~1.7 and 1.1 log CFU, respectively. Besifloxacin also had a lower MIC than gatifloxacin and moxifloxacin. These data suggest that besifloxacin is more efficacious than gatifloxacin and moxifloxacin in reducing the number of MRSA in the cornea when used topically from 10 to 18 h postinfection. Besifloxacin is also as effective as gatifloxacin and moxifloxacin at reducing the clinical severity when used topically at the same time points.
Bacterial keratitis can ultimately lead to loss of vision if not properly treated. Fluoroquinolones are widely used for treatment of bacterial keratitis because they are broad spectrum and easy to use and prepare.24 Previous studies have shown that fluoroquinolones are very effective in killing the bacteria that cause bacterial keratitis.25,26
There has been an increase in drug resistance of MRSA. There are now strains labeled as fluoroquinolone-resistant S. aureus. The use of quinolones selects for these quinolone-resistant mutants.27,28 Reports have demonstrated that topical antibiotic drops are not always efficient at killing S. aureus in keratitis infections.29,30 This is especially true at the later stages of infection, which could be due to lowered bacterial replication observed in the later stages of growth, the presence of pus inhibiting the activity of the antibiotic, or the quinolone not being able to reach the bacteria in the pus-filled ulcers.31 Previously, dual therapy using a fluoroquinolone and either cefazolin or tobramycin was the treatment of choice. Studies have shown that monotherapy with fluoroquinolones is just as effective, so treatment regimens have since changed.24,32
A study by Silvestri and colleagues (2004) demonstrated that oral vancomycin is a safe way to protect against MRSA infection in the body.33 However, vancomycin can cause adverse effects on the eye. The use of this drug for treating keratitis can lead to corneal edema and conjunctival inflammation.30,34 The use of besifloxacin on an uninfected eye showed no pathology (data not shown). Due to the selection of resistant mutants, and the harm caused by vancomycin that is often used in hospital settings to treat MRSA, new forms of antibiotics are constantly needed.
As mentioned before, a previous study demonstrated that when besifloxacin, gatifloxacin, and moxifloxacin were used for treatment between 16 and 25 h PI, there was not a difference in clinical severity when compared to the PBS treatment control.20 However, by the end of the treatment regimen, besifloxacin had significantly lowered the bacterial load in the cornea as compared to all other groups. Dajcs and colleagues (2004) observed that earlier treatment (10 h PI) was helpful in lowering bacterial load; however, that study did not examine differences in clinical severity of infection.18 This study demonstrated that besifloxacin was able to significantly lower the clinical severity of MRSA infection as effectively as moxifloxacin and gatifloxacin as compared to PBS when the early treatment is implemented. This finding is clinically relevant because it indicates a more positive outcome for keratitis patients who receive treatment as early as possible.
Erosions were observed in all groups pre- and posttreatment, and were approximately the same diameters in all of the corneas regardless of treatment. It appears that fluoroquinolone therapies at the time points utilized in this study are unable to prevent the production of S. aureus α-toxin, which is the primary toxin responsible for causing corneal erosions.31,35 Erosions were already forming prior to therapy, as shown in Figure 1B, so the bacteria that were present prior to therapy were able to secrete α-toxin. However, fluoroquinolone therapy was effective at reducing ocular infiltrate (Fig. 2). This reduction is important, as corneal infiltration and ulceration is largely responsible for subsequent scarring and impairment of vision.31 Also, a decrease in inflammation was observed in the fluoroquinolone-treated eyes, as demonstrated by more severe PMN infiltration in the anterior chamber in PBS-treated eyes (Fig. 3).
A study by Zhang and colleagues (2008) observed the anti-inflammatory effect of besifloxacin on human corneal epithelial cells in vitro.36 Besifloxacin inhibited the NFκB and MAPK pathways. Also, Zhang and Ward (2008) observed the anti-inflammatory effect of besifloxacin versus moxifloxacin on human THP-1 monocytes in vitro. In these studies, moxifloxacin was efficacious at 10 μg/mL, whereas besifloxacin significantly inhibited key inflammatory cytokines including interleukin (IL)-1α, granulocyte macrophage colony-stimulating factor (GM-CSF), IL-1 receptor antagonist, and IL-6 at 1 μg/mL showing a possible correlation to the MIC values.37 In multicenter, prospective, randomized, double-masked, vehicle-controlled clinical trials, treatment with 0.6% suspension of besifloxacin for 5 days significantly lowered clinical severity of bacterial conjunctivitis with bacterial load in patients.38,39
The current study demonstrated that besifloxacin, like the other fluoroquinolones used in this study, can significantly lower the clinical severity observed in MRSA keratitis when early treatment is implemented. Most importantly, besifloxacin showed a statistically significant efficacy improvement when compared to moxifloxacin and gatifloxacin, reducing the bacterial load recovered from the corneas after treatment.
Footnotes
Acknowledgment
The authors would like to thank Dr. William Johnson for his consultation in using the appropriate statistics for this study, Paula Pierce from Excalibur, Inc. for performing the histopathology, and Andrea Swiatlo for providing the MRSA isolate.
Author Disclosure Statement
Melissa Sanders, Quincy Moore III, Erin Norcross, and Mary Marquart have received funds for research from Bausch & Lomb. Afshin Shafiee works for Bausch & Lomb.