
Abstract
Abstract
Isolated superior ophthalmic vein (SOV) thrombosis is a rare condition usually related to inflammation of the orbit or paranasal sinuses.1–3 Patients present with acute orbital signs, including proptosis, ophthalmoplegia, globe dystopia, and periorbital edema, and may have diminished vision secondary to optic neuropathy. SOV thrombosis is typically seen in the setting of septic cavernous sinus thrombosis, and antimicrobial therapy is the treatment of choice. We herein report what may be the first case of isolated SOV thrombosis related to hypercoagulability in a patient with cancer who was receiving antifibrinolytic and thrombopoietin receptor agonist medications.
Case Report

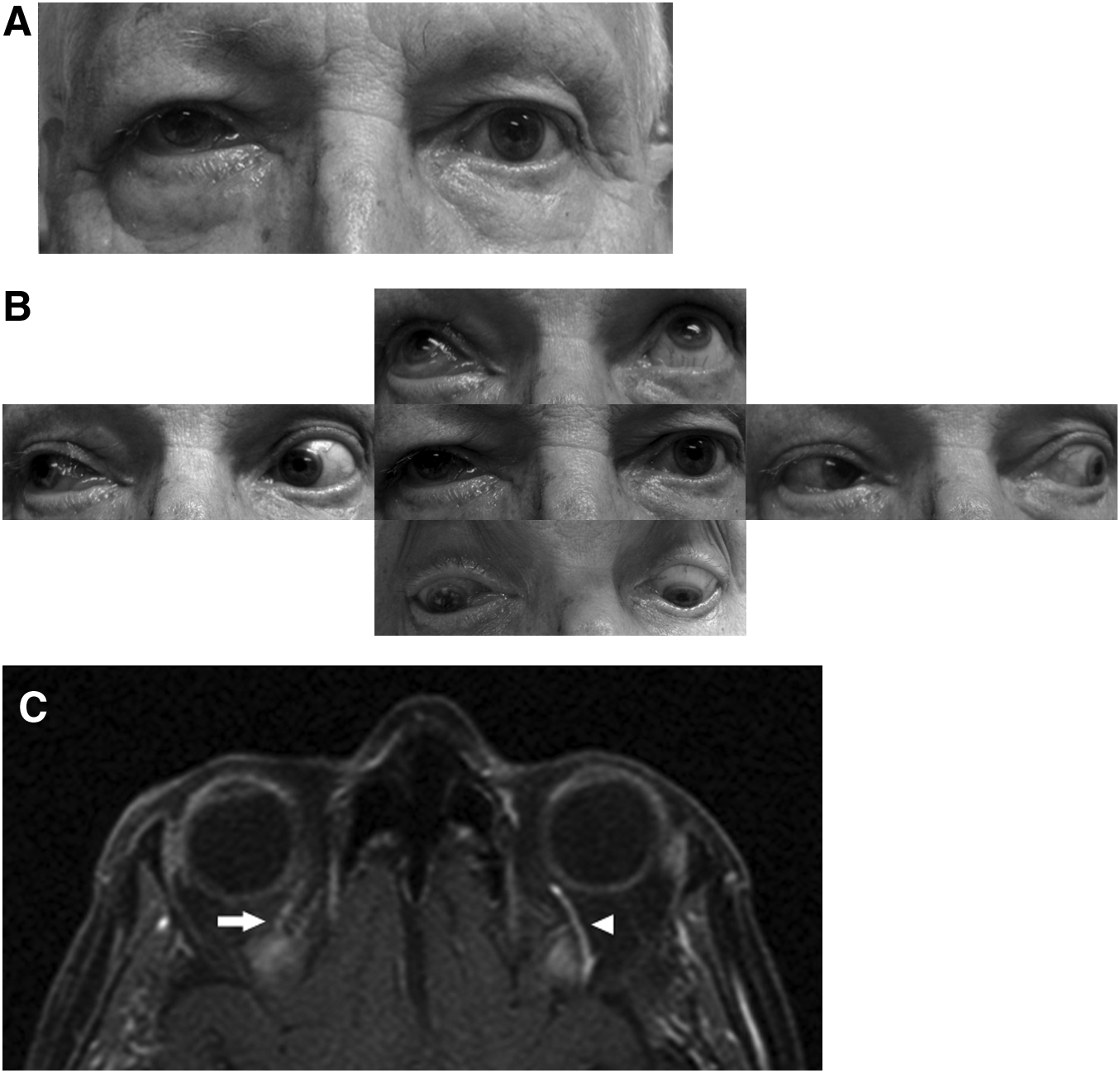
Patient at presentation with right (

Axial T1-weighted magnetic resonance imaging with contrast taken 1 day prior to onset of periorbital edema demonstrates a normal right (arrow) and left (arrowhead) superior ophthalmic vein (
His white blood cell count was elevated, at 34 k/ul with 10% blasts, and this was attributed to CML by the leukemia service. The platelet count was in the normal range, at 371 k/ul. A blood hypercoagulability work-up consisting of lupus anticoagulant, anti-cardiolipin antibodies, protein C and S, anti-thrombin III, homocysteine, and Leiden factor was ordered and was negative. Orbital computed tomography (CT) with contrast revealed a dilated right superior ophthalmic vein (SOV) that did not fill with contrast and mild bilateral mucosal thickening of the ethmoid and maxillary sinuses in keeping with the patient's history of chronic sinusitis (Fig. 2A, B). There was no evidence of compromise of the right medial orbital wall, orbital cellulitis, or cavernous sinus involvement. The findings were consistent with a diagnosis of an isolated right SOV thrombosis. Nasal endoscopy performed by the head and neck surgery service showed normal-appearing mucosa without evidence of infectious sinusitis, including fungal etiology. MRI of the brain, orbits, and skull base was ordered to better assess the cavernous sinus.
Aminocaproic acid was stopped, and anticoagulation with intravenous heparin was started immediately. The patient was admitted to the hospital and started on broad-spectrum intravenous antimicrobials for prophylaxis against infection and topical brimonidine and dorzolamide/timolol for ocular hypertension. Ophthalmic bacitracin ointment was applied to the exposed conjunctiva, and a short 2-day course of intravenous methylprednisolone was given in case vision loss was due to optic neuropathy and could be stabilized or improved.
The patient's examination results remained stable, with normalization of intraocular pressure, until hospital day 3, when visual acuity in the right eye decreased acutely to no light perception. Retinal examination did not reveal any acute vascular event, but did show exudative peripheral choroidal detachments. MRI also confirmed an isolated SOV thrombosis without any evidence of a cavernous sinus thrombosis. The interventional radiology service was willing to inject a thrombolytic agent into the ophthalmic artery in an attempt to lyse the thrombus, but the patient declined as this procedure was thought to at best offer a modest chance of vision restoration and was associated with significant risks. Over the next several days, the patient's extraocular movements and chemosis gradually improved, and his visual acuity remained at no light perception. He was discharged home on hospital day 8 on subcutaneous enoxaparin. Two weeks after initial presentation, the chemosis, periorbital edema, extraocular movements, and choroidal detachments were largely resolved (Fig. 3), and by 7 weeks the SOV thrombosis had resolved radiographically, although vision remained at no light perception.
The patient 2 weeks after initial presentation with improved right (
Discussion
Isolated SOV thrombosis is a rare clinical finding that can have aseptic or, more commonly, septic causes. Septic causes include infectious sinusitis, osteomyelitis, and orbital cellulitis.1,3 Examples of aseptic causes include hypercoagulability (due to oral contraceptive pills, pregnancy, and thrombocytosis), inflammatory conditions (systemic lupus erythematosis, Behcet syndrome, sarcoidosis, idiopathic orbital inflammation, or thyroid eye disease), invasion by tumor (leukemia, lymphoma, or meningioma), trauma (fracture or surgery), and spontaneous closure of a dural sinus fistula.1–3 Clinical signs all stem from a disruption in orbital venous outflow and include periorbital edema, proptosis, globe dystopia, ophthalmoplegia, chemosis, episcleral vascular tortuosity, ocular hypertension, a shallow anterior chamber, and choroidal effusion. 3 Visual acuity may become compromised due to a central retinal artery or vein occlusion or due to optic neuropathy, and a relative afferent pupillary defect may be elicited. 3 The loss of vision in this report to no light perception without an intraretinal vascular insult was consistent with an ischemic optic neuropathy stemming from the SOV thrombosis.
MRI is the radiographic modality of choice, and diagnosis is typically made when an enlarged SOV is noted on orbital imaging without involvement of the cavernous sinus. The cavernous sinus, however, is affected in 33%–75% of septic cases and is associated with a significant mortality rate of 20%–30%.3,4 It is therefore crucial to carefully investigate whether the cavernous sinus is involved in patients with suspected SOV thrombosis. CT angiography, MR venography, and orbital color Doppler ultrasonography may be useful in the work-up by studying SOV flow.
Treatment of SOV thrombosis is dependant on the etiology. It is important to always consider an infectious cause, and antimicrobials should be administered without delay in septic cases. In aseptic cases, anticoagulation therapy is typically given, and the addition of a short course of steroids has been described. 3 Clinical trials have yet to validate anticoagulation therapy in patients with SOV thrombosis, and our use of anticoagulants parallels established practices of treating thromboses of other anatomic locations. Consideration of anticoagulation should always be determined with the patient's risk for bleeding complications in mind, as this represents the major risk of treatment. Visual prognosis is difficult to estimate given the rarity of SOV thrombosis, but poor prognostic indicators include septic causes and involvement of the cavernous sinus.
It is well established that patients with leukemia are at risk for thrombotic events. The incidence of thrombosis in patients with hematologic malignancies ranges from 5% to 34%. 5 Specific risk factors for thrombosis in patients with leukemia include hyperviscosity from leukocytosis and adverse effects of systemic medications. 5 The pathogenesis of the SOV thrombosis in our patient likely was multifactorial: his risk factors included cancer history, recent romiplostim-induced thrombocytosis, leukocytosis, and antifibrinolytic treatment with aminocaproic acid. Romiplostim is a relatively new thrombopoietin receptor agonist available as a weekly subcutaneous injection used in the treatment of chronic thrombocytopenia. 6 The half-life of romiplostim is 3.5 days. 6 It was given to our patient in an attempt to stimulate platelet formation and improve his gastrointestinal bleed. The platelet count in our patient acutely increased from 9 to 618 k/ul upon administration of romiplostim. Aminocaproic acid inhibits plasminogen activators, thereby interfering with fibrinolysis. The drug has a half-life of 2 h. 7 It is given in the setting of various bleeding disorders such as chronic bleeding following dental procedures or for traumatic hyphema. A known side effect of both aminocaproic acid and romiplostim is thrombosis, 6 and although not previously reported in the literature, a potential synergistic effect of causing thrombosis may exist as highlighted in this report. Our patient had been taking aminocaproic acid suppressing fibrinolytic activity, and then romiplostim was introduced, which increased his platelet count, and the administration of these 2 drugs in concert may have produced the thrombogenic environment leading to his SOV thrombosis. To our knowledge, SOV thrombosis caused by either medication has not previously been described in the literature.
Isolated SOV thrombosis is a rare but serious condition associated with a risk of poor visual outcome. This report highlights the need to consider this diagnosis in patients with cancer and acute onset of proptosis and increased orbital pressure who may have been exposed to antifibrinolytic therapy or medications that can induce thrombocytosis.
Footnotes
Acknowledgments
No funding was received for the work presented in this article.
Author Disclosure Statement
No competing financial interests exist.