
Abstract
Abstract
Purpose:
To investigate the influence of 2% carteolol long-acting solution (long-acting carteolol) and 0.5% timolol gel-forming solution (timolol gel) on ocular wavefront aberrations.
Methods:
Ocular aberrations were assessed in the right eye of 24 healthy volunteers at baseline and at 2, 5, 10, and 15 min after instillation of long-acting carteolol, timolol gel or physiological saline using the Hartmann-Shack aberrometer. Ten serial measurements were taken over 10 s at each time point, and the root mean square (RMS) of second-, third-, fourth-, and total higher-order aberrations were calculated. The stability index and fluctuation index were also determined.
Results:
Second-order aberrations did not change significantly after instillation of study eye-drops. Higher-order aberrations increased significantly after instillation of long-acting carteolol and timolol gel. Timolol gel induced significantly larger changes than long-acting carteolol in third-order RMS at 2 min (P = 0.001), fourth-order RMS at 2 (P < 0.001) and 5 (P = 0.013) min, and total higher-order RMS at 2 (P < 0.001) and 5 (P = 0.016) min after instillation, but not at 10 and 15 min after administration. Fluctuation index increased significantly after instillation of each eye-drop (P < 0.001), with significantly larger increases after timolol gel than long-acting carteolol at 2 min (P = 0.005) and 5 min (P = 0.011). No significant changes were observed in stability index.
Conclusions:
Both topical β blockers with a once-daily dosing regimen temporarily deteriorate optical quality of the eye by increasing higher-order aberrations, and the increases are much larger after instillation of timolol gel than long-acting carteolol.
Introduction
One adverse event associated with timolol gel-forming solution is a transient blurring of vision after instillation, probably due to changes in tear film dynamics. 8 The incidence of blurred vision varies considerably between studies, with reported incidences ranging from 2.5% to 66.7%.3–5,9–11 In a study that used a questionnaire to assess the incidence and duration of blurred vision after instillation of timolol gel-forming solution, 11 66.7% of patients reported blurred vision and the mean duration was 4.5 ± 7.3 min. The longest duration of blurred vision after instillation was reported to be 30 min, and 38.2% of patients reported that blurred vision lasted longer than 5 min. We previously investigated the influence of timolol gel-forming solution on ocular wavefront aberrations during 12 h after instillation and found that higher-order aberrations significantly increased at 5 min after instillation but not at 30 min and thereafter. 8 Unfortunately, we did not set the measurement points between 5 and 30 min and, thus, the detailed time course of changes in higher-order aberrations shortly after instillation remains unclear.
Carteolol is another β blocker widely used in the treatment of glaucoma and ocular hypertension. 2 Standard formulations of carteolol are administered twice daily. Recently, a new carteolol ophthalmic solution containing alginic acid (carteolol long-acting solution) was developed to allow once-daily administration, 12 while offering similar efficacy and tolerability as the standard formulation. 13 The addition of alginic acid in this formulation prolongs the action of eye-drops by increasing viscosity of the preparation, resulting in increased precorneal retention time of carteolol.12,14 In addition, alginic acid has good mucoadhesive properties,15–17 which increases the corneal contact time of carteolol and allows increased penetration of carteolol into the aqueous humor. 12 This formulation does not produce a gel on the corneal surface and has a relatively low viscosity that is not significantly affected by contact with tears, 14 but still blurred vision is caused by carteolol long-acting solution in some patients. 13
However, there have been no studies that investigated the influence of carteolol long-acting solution on optical quality of the eye. As for timolol gel-forming solution, there is a need to examine changes in optical quality in more detail in the early phase after instillation. Since both eye-drops are widely used in patients with visual disturbances such as visual field defect, it is important to assess the exact influence of these drugs on the optical quality of the eye, so that patients and practitioners are well informed. In this study, we objectively and quantitatively investigated the influence of carteolol long-acting solution and timolol gel-forming solutions on the optical quality of the eye by evaluating ocular wavefront aberrations for up to 15 min after instillation.
Patients and Methods
This single-center study enrolled healthy volunteers without systemic and ocular diseases (except mild refractive errors). Subjects were excluded from the study if they used contact lenses, had a history of eye surgery or trauma, had symptoms of dry eye, or were regular users of eye-drops. A total of 24 volunteers [10 men and 14 women; 30.7 ± 10.0 years (mean ± standard deviation)] were enrolled. All study participants had a best-corrected visual acuity of 20/20 or better at the time of enrolment. The study was approved by the institutional review board of Tsukuba University Hospital and adhered to the tenets of the Declaration of Helsinki. The nature and possible consequences of the study were explained to the study participants in detail, and all study participants gave informed consent.
Only 1 eye of each subject was used for assessments. Study participants received 1 drop of 2% carteolol long-acting solution (long-acting carteolol) (Mikelan LA®; Otsuka Pharmaceutical Co. Ltd., Tokyo, Japan), 0.5% timolol maleate gel-forming solution (timolol gel) (Timoptol XE®; Banyu Pharmaceutical Co. Ltd., Tokyo, Japan) or physiological saline (saline) in the right eye. Saline was used as a control solution. The order of study eye-drops was randomized; all participants received all study drugs in a crossover design. Ocular aberrations were assessed in a darkened room at baseline and at 2, 5, 10, and 15 min after instillation of the eye-drops, using the Hartmann-Shack aberrometer (KR-1W; Topcon Corp., Tokyo, Japan). At each assessment time point, 10 serial images were obtained at 1-s intervals (over 10 s) after a blink. Study subjects were instructed to keep their eyes open during the image capture.
Normalized Zernike polynomials were used to expand the acquired data sets and, from the Zernike coefficients, the root mean square (RMS) was calculated for second-, third-, fourth-, and total higher-order (third- and fourth-order) aberrations in the central 4-mm diameter. The fluctuation index (FI) and stability index (SI) of the total higher-order aberrations were calculated from the sequential changes in ocular aberrations over time. The FI is the standard deviation of the total higher-order aberrations during the serial 10-s assessments, which reflects the higher-order aberration fluctuations during the measurements. The SI, calculated as the slope of the linear regression line of the total higher-order aberrations obtained, reflects the trend of the sequential changes in higher-order aberrations during the measurement.18,19
The 10 serial measurements were averaged for each time point assessment and analyzed using repeated-measures analysis of variance (ANOVA) to determine the time course of changes in aberrations over 15 min. If significant differences were observed, the Dunnett post hoc test for multiple comparisons was used to identify time points with a significant difference from baseline. At each time point, each parameter was compared between the 3 study eye-drops using 1-way ANOVA. Bonferroni's multiple comparison test was performed if 1-way ANOVA was significant. A P value of <0.05 was considered statistically significant. All statistical analyses were performed using SPSS version 15.0J software.
Results
The time courses of changes in second-, third-, fourth-, and total higher-order RMS over 15 min after instillation are shown in Figs. 1–4. There were no significant changes in second-order RMS by instillation (P = 0.586 for saline, P = 0.241 for long-acting carteolol, and P = 0.212 for timolol gel, repeated-measures ANOVA), and there was no difference between the 3 eye-drops at any time point (P = 0.929–.984, 1-way ANOVA) (Fig. 1).

Time course of changes in second-order RMS after instillation. There were no significant changes in second-order RMS up to 15 min after instillation (P = 0.586 for saline, P = 0.241 for long-acting carteolol, and P = 0.212 for timolol gel, repeated-measures ANOVA). Graphs are expressed as the mean + standard deviation. ANOVA, analysis of variance; RMS, root mean square.
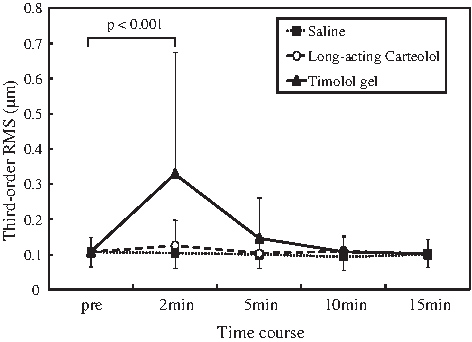
Time course of changes in third-order RMS after instillation. Third-order RMS significantly changed after instillation of timolol gel (P < 0.001, repeated-measures ANOVA), but did not change after instillation of long-acting carteolol (P = 0.127) or saline (P = 0.250). There was a significant increase from baseline in third-order RMS at 2 min after instillation of timolol gel (P < 0.001, Dunnett post hoc test), but not at 5, 10, or 15 min after instillation (P = 0.799, 0.999, and 0.999, respectively). Graphs are expressed as the mean ± standard deviation.
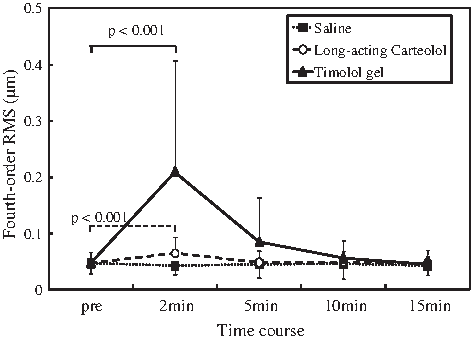
Time course of changes in fourth-order RMS after instillation. Fourth-order RMS significantly changed after instillation of timolol gel (P < 0.001, repeated-measures ANOVA) and long-acting carteolol (P < 0.001), but did not change after instillation of saline (P = 0.516). Multiple comparison analysis showed significant increases in fourth-order RMS at 2 min after instillation of timolol gel and long-acting carteolol compared with the baseline values (both P < 0.001, Dunnett post hoc test), but there were no significant increases from the baseline at 5,10, and 15 min after instillation (P = 0.492–0.999). Graphs are expressed as the mean ± standard deviation.
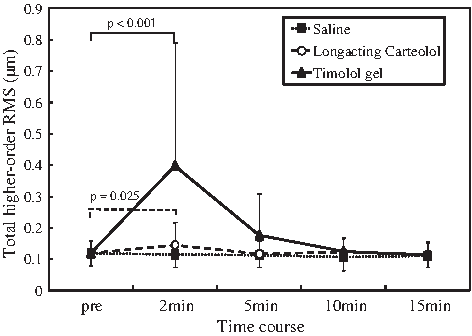
Time course of changes in total higher-order RMS after instillation. Total higher-order RMS significantly changed after instillation of timolol gel (P < 0.001, repeated-measures ANOVA) and long-acting carteolol (P = 0.011), but did not change after instillation of saline (P = 0.344). Multiple comparison analysis showed significant increases in total higher-order RMS at 2 min after instillation of timolol gel (P < 0.001, Dunnett post hoc test) and long-acting carteolol (P = 0.025) compared with the baseline values, but there were no significant increases from the baseline at 5,10, and 15 min after instillation (P = 0.662–0.999). Graphs are expressed as the mean ± standard deviation.
Third-order RMS changed significantly after instillation of timolol gel (P < 0.001, repeated-measures ANOVA), but it did not change after instillation of long-acting carteolol (P = 0.127) or saline (P = 0.250). Multiple comparison analysis revealed that there was a significant increase in third-order RMS at 2 min after instillation of timolol gel compared with the baseline value (P < 0.001, Dunnett post hoc test), but the increase from the baseline value at 5, 10, and 15 min after instillation of timolol gel was not significant (P = 0.799, 0.999, and 0.999, respectively) (Fig. 2). When the 3 eye-drops were compared, significant differences were found only at 2 min after instillation (P < 0.001, 1-way ANOVA) but not at 5, 10, and 15 min after instillation (P = 0.068, 0.391, and 0.996, respectively). Bonferroni's multiple comparison test showed that there were significant differences between timolol gel and long-acting carteolol (P = 0.001) and between timolol gel and saline (P < 0.001) at 2 min after instillation (Table 1).
Statistically significant difference observed with Bonferroni's test.
Saline, physiological saline; Carteolol, carteolol long-acting solution; Timolol, timolol maleate gel-forming solution; NS, not significant.
Fourth-order RMS changed significantly during the 15 min after instillation of timolol gel (P < 0.001, repeated-measures ANOVA) and long-acting carteolol (P < 0.001), but it did not significantly change after instillation of saline (P = 0.516). Multiple comparison analysis showed significant increases in fourth-order RMS at 2 min after instillation of timolol gel and long-acting carteolol compared with the baseline values (both P < 0.001, Dunnett post hoc test), but there were no significant increases from the baseline at 5, 10, and 15 min after instillation (P = 0.492–0.999) (Fig. 3). When the 3 eye-drops were compared, significant differences were found at 2 and 5 min after instillation (P < 0.001 and P = 0.012, 1-way ANOVA) but not at 10 and 15 min after instillation (P = 0.349 and P = 0.581, respectively). Bonferroni's multiple comparison test showed that there were significant differences between timolol gel and long-acting carteolol (P < 0.001 at 2 min and P = 0.013 at 5 min) and between timolol gel and saline (P < 0.001 and P = 0.007, respectively) (Table 1).
Total higher-order RMS changed significantly during the 15 min after instillation of timolol gel (P < 0.001, repeated-measures ANOVA) and long-acting carteolol (P = 0.011) but not after instillation of saline (P = 0.344). Multiple comparison analysis showed significant increases in total higher-order RMS at 2 min after instillation of timolol gel (P < 0.001, Dunnett post hoc test) and long-acting carteolol (P = 0.025) compared with baseline values, but there were no significant increases from baseline at 5, 10, and 15 min after instillation (P = 0.662–0.999) (Fig. 4). When the 3 eye-drops were compared, significant differences were found at 2 and 5 min after instillation (P < 0.001 and P = 0.017, 1-way ANOVA) but not at 10 and 15 min after instillation (P = 0.295 and P = 0.941, respectively). Bonferroni's multiple comparison test showed that there were significant differences between timolol gel and carteolol long-acting (P < 0.001 at 2 min and P = 0.016 at 5 min) and between timolol gel and saline (P < 0.001 and P = 0.011, respectively) (Table 1).
FI changed significantly during the 15 min after instillation of each of the 3 eye-drops (P < 0.001 for all eye-drops, repeated-measures ANOVA). Multiple comparison analysis showed significant increases in FI at 2 min after instillation compared with baseline values (P < 0.001 for all eye-drops, Dunnett post hoc test), but the increases from baseline were not significant at 5, 10, and 15 min after instillation of any of the eye-drops (P = 0.706–.999) (Fig. 5). When the 3 eye-drops were compared, significant differences were found at 2 and 5 min after instillation (P = 0.003 and P = 0.009, 1-way ANOVA) but not at 10 and 15 min after instillation (P = 0.601 and P = 0.690, respectively). Bonferroni's multiple comparison test showed that there were significant differences between timolol gel and long-acting carteolol (P = 0.005 at 2 min and P = 0.011 at 5 min after instillation) and between timolol gel and saline (P = 0.002 and P = 0.006, respectively) (Table 1).
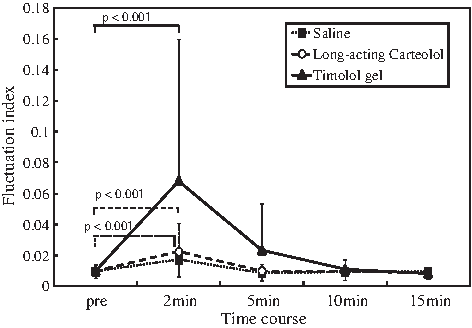
Time course of changes in FI after instillation. FI significantly changed after instillation of all 3 eye-drops (P < 0.001 for all eye-drops, repeated-measures ANOVA). Multiple comparison analysis showed significant increases in FI at 2 min after instillation compared with the baseline values (P < 0.001 for all eye-drops, Dunnett post hoc test), but the increases from the baseline were not significant at 5, 10, and 15 min after instillation of any eye-drops (P = 0.706–0.999). Graphs are expressed as the mean ± standard deviation. FI, fluctuation index.
No significant fluctuations were observed in SI for any of the study eye-drops over the study period (P = 0.544 for timolol gel, P = 0.900 for long-acting carteolol, and P = 0.269 for saline, repeated-measures ANOVA). In addition, there were no significant differences in SI between the 3 eye-drops at any time point (P = 0.464–0.889, 1-way ANOVA) (Fig. 6).

Time course of changes in stability index after instillation. No significant fluctuations were observed in stability index over the study period (P = 0.544 for timolol gel, P = 0.900 for long-acting carteolol, and P = 0.269 for saline, repeated-measures ANOVA). Graphs are expressed as the mean ± standard deviation.
Discussion
The tear film is formed by blinking and creates a smooth, regular surface over the anterior of the cornea. It is the first refractive surface of the eye and an important optical element; consequently, irregularities in the tear film can alter the optical quality of the eye and quality of vision.20–25 Wavefront sensing has been used to objectively and quantitatively evaluate the degradation of optical quality caused by tear film irregularity and instability.20,22,23 However, these changes are not static but dynamic. Hence, sequential changes in ocular wavefront aberrations have been recently assessed with serial measurements to understand the influence of dynamic changes in tear film on the optical quality of the eye.8,18,19,21,26,27 In many previous studies, sequential wavefront aberrations were measured in normal and dry eyes to evaluate tear film behavior after blinking.18,19,26,27 However, little is known about tear film dynamics and optical changes after instillation of eye-drops. In this study, we investigated and compared the influence of 2 antiglaucoma eye-drops on tear film dynamics by evaluating sequential wavefront aberrations.
As shown in the results, the changes in optical quality significantly differed between the eye-drops. None of the eye-drops affected second-order aberrations, but higher-order aberrations increased significantly after instillation of timolol gel and long-acting carteolol, but not saline. Timolol gel increased both coma-like and spherical-like aberrations, whereas long-acting carteolol increased spherical-like aberration alone, which was significantly smaller than that observed with timolol gel. Oshika et al. 28 reported that contrast sensitivity function significantly correlated with ocular higher-order aberrations in normal human eyes, coma-like aberration was primarily responsible for the loss of contrast sensitivity, and spherical-like aberration had little influence. The authors speculated that rotationally symmetrical aberration might be more forgiving in terms of the adverse influence on visual images, whereas rotationally asymmetrical (off-axis) aberration (i.e., third-order coma-like aberration) caused greater degradation of visual images. 28 Thus, it appears that the influence of timolol gel on visual function and symptom is much larger than that of long-acting carteolol. Unfortunately, we did not examine visual function in this study. The verification of this speculation requires further studies.
The changes in higher-order aberrations continued for 5 min after instillation and were greater at 2 min than at 5 min. In our previous study, 8 we assessed ocular aberrations only at 5 and 30 min in the early phase after instillation of timolol gel. In the current study, we examined ocular aberration at 2, 5, 10, and 15 min after instillation and revealed that the mean amount of higher-order aberrations at 2 min was approximately twice as large as that at 5 min and that the higher-order aberrations returned to baseline levels at 10 min after instillation of timolol gel.
The long-acting carteolol significantly increased higher-order aberrations shortly after application, but those changes were small and transient, and their magnitude and time course were almost similar with those after instillation of saline. The influence of long-acting carteolol on optical quality of the eye was found to be significantly smaller than that of timolol gel.
The results of FI analysis indicated that higher-order aberrations were unstable immediately after instillation of the eye-drops, especially after instillation of timolol gel, reflecting the instability of the tear film, although these fluctuations returned to the baseline level by 10 min after instillation. SI did not change significantly by any of the eye-drops, suggesting that the time course of changes in higher-order aberrations do not have monotonic patterns similar to an upward or downward tendency.
These objectively measured differences are consistent with patients' subjective evaluation, that is, patients receiving timolol gel generally report a higher incidence of blurred vision3–5,9–11 than those receiving long-acting carteolol. 13 These results suggest that ocular wavefront analysis is a useful method to objectively and quantitatively evaluate the influence of ocular treatment, such as long-acting eye drops, on optical quality of the eye.
The difference between these 2 once-daily ophthalmic solutions in terms of their influence on the optical quality seems attributable to the behavior of the solution in the context of physicochemical environment of the ocular surface. 29 For timolol gel, gellan gum rheology depends on the presence of mono- and divalent cations such that it forms a gel on mixing with the tear fluid. 4 The in-situ gelling of timolol gel resists ocular drainage, thereby prolonging the precorneal contact time. 30 Once the gel forms, the formulation is subsequently dispersed by the shearing action of the eyelids that fragments the gel, and the gel fragments are gradually cleared from the ocular surface through the nasolacrimal duct. 31 If the gel fragments are unevenly distributed between the center and periphery of the cornea, rotationally symmetrical changes in higher-order aberrations, such as increases in spherical aberration, would be produced. It is also considered that the gel fragments easily move on the ocular surface after blinking and result in inferosuperior and/or temporonasal asymmetrical distribution, 8 leading to increases in coma-like aberration. On the other hand, the carteolol long-acting formulation does not form a gel on the ocular surface. The prolonged activity of long-acting carteolol compared with standard carteolol is due to the good mucoadhesive properties of alginic acid, 16 which allows increased contact time on the surface of the eye. Therefore, unlike the gel-forming solution, this formulation is unlikely to greatly affect tear film dynamics. Although a significant increase in spherical-like aberration was observed immediately after instillation of long-acting carteolol in the current study, the change was extremely small. We speculate that the small increase in spherical-like aberration was induced by uneven adhesion of alginic acid to the ocular surface especially between the center and periphery of the cornea. Further, in vitro release studies suggest that there are ionic interactions between carteolol and alginic acid that result in slow release of the drug. 12 Combined, these observations can explain the enhanced delivery of carteolol by the alginic acid in the absence of substantial changes in ocular aberrations.
There is a weakness of our study. We did not evaluate visual function and subjective symptoms such as blurred vision after instillation. It is interesting to know how the changes in ocular aberration after instillation affect visual performance and subjective visual symptoms. This will be the theme of future studies.
In conclusion, both long-acting carteolol and timolol gel transiently increased higher-order aberrations after instillation. However, the changes were much larger after instillation of timolol gel than long-acting carteolol. In clinical practice, patients should be informed of possible temporal reduction in optical quality of the eye immediately after the application of these eye-drops. Since glaucoma is a disease that generally requires lifelong daily treatment, minimizing treatment-related adverse effects on visual quality would be beneficial for patients.
Author Disclosure Statement
No competing financial interests exist. The authors have no commercial or proprietary interest in any of the companies, products, or methods described in this article.