
Abstract
Abstract
Purpose:
To determine the element that modulates benzalkonium chloride (BAC) toxicity by using a new electrophysiological method to evaluate acute corneal barrier dysfunction induced by travoprost Z with sofZia (Travatan Z®), travoprost with 0.015% BAC (Travatan®), and its additives.
Methods:
Corneal transepithelial electrical resistance (TER) was measured in live white Japanese rabbits by 2 Ag/AgCl electrodes placed in the anterior aqueous chamber and on the cornea. We evaluated corneal TER changes after a 60-s exposure to travoprost Z, travoprost, and 0.015% BAC. Similarly, TER changes were evaluated after corneas were exposed for 60 s to the travoprost additives ethylenediaminetetraacetic acid disodium salt, boric acid, mannitol, trometamol, and polyoxyethylene hydrogenated castor oil 40 (HCO-40) with or without BAC. Corneal damage was examined after exposure to BAC with or without travoprost additives using scanning electron microscopy (SEM) and a cytotoxicity assay.
Results:
Although no decreases of TER were noted after exposure to travoprost Z with sofZia and travoprost with 0.015% BAC, a significant decrease of corneal TER was observed after 0.015% BAC exposure. With the exception of BAC, no corneal TER decreases were observed for any travoprost additives. After corneal exposure to travoprost additives with BAC, HCO-40 was able to prevent the BAC-induced TER decrease. SEM observations and the cytotoxicity assay confirmed that there was a remarkable improvement of BAC-induced corneal epithelial toxicity after addition of HCO-40 to the BAC.
Conclusions:
Travoprost Z with sofZia and travoprost with BAC do not induce acute corneal barrier dysfunction. HCO-40 provides protection against BAC-induced corneal toxicity.
Introduction
Glaucoma is a chronic progressive optic neuropathy that requires long-term treatment with topical medications. Many classes of eye drops are currently used to treat glaucoma, including cholinergic agents, beta-blockers, alpha-adrenergic agonists, carbonic anhydrase inhibitors, and prostaglandin analogs. Among these eye drops, prostaglandin analogs occupy the center stage and are considered to be the first-line medications. 11 The 4 different prostaglandin analogs that are currently available for the treatment of glaucoma are latanoprost, travoprost, bimatoprost, and tafluprost. The formulations of each of these also contain BAC, with levels that range from 0.005% to 0.02%. Previous studies in glaucoma patients have demonstrated that the use of eye drops containing BAC may affect the vision-related quality of life 12 and that chronic use of eye drops containing BAC can reduce the success of glaucoma filtration surgery.13–16 Therefore, the general consensus today is that chronic use of prostaglandin analogs that contain BAC has the potential to cause adverse corneal effects.
There are 2 kinds of travoprost ophthalmic solutions: travoprost Z, which uses the sofZia preservative (Travatan Z®; Alcon, Fort Worth, TX), and travoprost, which is preserved using 0.015% BAC (Travatan®; Alcon). Travoprost Z uses the newly developed sofZia, which is a non-BAC preservative system that was created to prevent the BAC-caused ocular surface side effects. An in vitro study that used conjunctiva-derived epithelial cells has shown that travoprost Z has a significantly lower cytotoxicity and pro-apoptotic effect than travoprost does. 17 To date, however, there have been no reports that have compared acute corneal impairment after exposure to travoprost Z and travoprost in vivo.
On the other hand, we have already developed a new in vivo method for measuring the transepithelial electrical resistance (TER) of live rabbit corneas. 18 This novel approach for examining the clinical instillation of eye drops has revealed that exposure to BAC concentrations between 0.005% and 0.02% immediately causes acute corneal dysfunction.19,20 In our preliminary experiments, we found that travoprost caused low acute corneal impairment regardless of whether it contained 0.015% BAC. Therefore, we decided to further examine this phenomenon by electrophysiologically comparing the acute corneal barrier dysfunction induced by travoprost Z, travoprost, and 0.015% BAC. Additionally, we attempted to determine the element responsible for modulating the BAC toxicity.
Methods
Chemicals
Two kinds of travoprost ophthalmic solutions, travoprost Z (Travatan Z) and travoprost (Travatan), were obtained from Alcon. BAC 10% solution and trometamol were purchased from Wako Pure Chemical Co. (Osaka, Japan). Boric acid and mannitol were obtained from Nacalai Tesque (Kyoto, Japan) and Sigma-Aldrich Japan (Tokyo, Japan), respectively. Polyoxyethylene hydrogenated castor oil 40 (HCO-40) was purchased from Nikko Chemicals (Tokyo, Japan). Ethylenediaminetetraacetic acid disodium salt (EDTA), 2-(4-lodophenyl)-3-(4-nitrophenyl)-2H-tetrazolium, monosodium salt (WST-1), and 1-methoxy-5-methylphenazinium methylsulfate (1-methoxy PMS) were obtained from Dojindo Laboratories (Kumamoto, Japan). Hank's balanced salt Ca2+- and Mg2+-free solutions (HBSS) were purchased from Invitrogen (Carlsbad, CA). Rabbit corneal epithelial cell growth medium (RCGM) and culture reagents were obtained from Kurabo (Osaka, Japan). Test solutions such as 0.02% BAC, 0.1% EDTA, 2% boric acid, 2% mannitol, 0.5% trometamol, and 1% HCO-40 were prepared in HBSS or RCGM. The concentrations for each of the agents were set at levels that corresponded to those found in the clinically used ophthalmic solutions.
Experimental animals
Male white Japanese rabbits (KBT Oriental, Tosu, Japan) weighing 2.5–3.0 kg were individually housed in cages under a controlled temperature (21°C) and humidity (50%±5%) and a 12:12 h light/dark cycle at the Laboratory Animal Center for Biomedical Research, Nagasaki University School of Medicine. Initiation of the study occurred once the rabbits reached weights of 3.0–4.0 kg, as this was the point where corneal diameters were of a suitable size for experimentation. The rabbits were treated in compliance with the Association for Research in Vision and Ophthalmology (ARVO) Statement for the Use of Animals in Ophthalmic and Vision Research.
TER measurement
The rabbits were anesthetized with an intramuscular injection of 30 mg/kg ketamine (Ketalar; Sankyo, Tokyo, Japan) and 5 mg/kg xylazine (Celactal; Bayer Health Care, Osaka, Japan). The experimental procedure was started within 10 min of the induction of anesthesia. After a slit lamp examination of the eyes to confirm that the cornea was intact, adhesive tape was applied so that one eye was kept open while the other eye was kept closed.
After a small incision was made with an 18-gauge sharp needle (Terumo, Tokyo, Japan) in the peripheral cornea, a 1.0-mm-diameter custom-made Ag/AgCl electrode (Physiotech, Tokyo, Japan) was inserted into the anterior chamber. A 6.0-mm-internal-diameter (0.28 cm2 inner area) nitrile rubber O-ring (Union Packing; SAN-EI, Osaka, Japan) was fixed on the cornea using biomedical adhesive (Alon-Alpha A; Sankyo). Subsequently, 80 μL of HBSS was placed inside the ring, with the second electrode then placed in HBSS on the cornea. This initial procedure was carefully conducted to avoid damaging the center of the cornea. The specific methodology and photographs of the in vivo corneal TER measurement system have been previously published. 18
The TER was measured in real time using a volt-ohm meter (EVOMX; World Precision Instruments, Sarasota FL) that generated a±20 μA AC square wave current at 12.5 Hz. Data were recorded using a thermal array recorder (WR300-8; Graphtec, Tokyo, Japan). In just a few seconds, 1 mL of either the eye drops or the test solutions was gently poured into the ring, with all of the overflow being aspirated. After an exposure for 60 s, the rings were washed out using 1 mL of HBSS. After obtaining the TER of the cornea before and after the exposure, results were then calculated as a percentage of the pre-exposure TER value (100%).
Scanning electron microscopy observation
The rabbits were anesthetized with an intramuscular injection of 30 mg/kg ketamine and 5 mg/kg xylazine. All corneas were evenly soaked in each of the test solutions for 60 s, with HBSS used to wash out the corneas. After the corneal washing, the rabbits were immediately sacrificed using a lethal dose of intravenous sodium pentobarbital (Nembutal; Dainippon Pharmaceutical, Osaka, Japan). The corneas were carefully excised, fixed in 4% glutaraldehyde in 0.05 M cacodylate buffer for 1 h, and then post-fixed in 1% osmium tetroxide in veronal acetate buffer containing 0.22 M sucrose. The fixed materials were dehydrated through a series of ethanol washes. Corneas were placed in t-butyl alcohol after being treated in a freeze-drying apparatus (EIKO ID-2; EIKO, Tokyo, Japan), sputter coated with gold using an auto fine coater (JEOL JFC-1600; JEOL, Tokyo, Japan), and then examined using a scanning electron microscope (Hitachi S2360; Hitachi, Tokyo, Japan).
Cytotoxicity assay
The normal rabbit corneal epithelial (NRCE) cells were obtained from Kurabo. The NRCE cells were maintained in RCGM, which was supplemented with 5 μg/mL insulin, 10 ng/mL epidermal growth factor, 0.5 μg/mL hydrocortisone, 50 μg/mL gentamicin, 50 ng/mL amphotericin B, and 0.4% bovine pituitary extractives reagent. The cells were grown at 37°C in a humidified atmosphere with 5% CO2. Cytotoxicity tests on NRCE cells were carried out using a WST-1 commercially available cell proliferation reagent. The assay was based on cleavage of the tetrazolium salt WST-1 by active mitochondria to produce a soluble colored formazan salt. Since the conversion can only occur with viable cells, results are directly correlated to the cell number. The stock solutions of WST-1 (5.5 mM) and 1-methoxy PMS (2 mM) were prepared in sterilized phosphate-buffered saline. Just before each of the experiments, the mixture was prepared by combining 0.9 mL of WST-1 solution and 0.1 mL of 1-methoxy PMS solution. NRCE cells were plated at 3×103 cells/well in 96-well microtiter plates (Becton-Dickinson, Franklin, NJ). Six days after plating, the growth medium was replaced with 100 μL of the test solutions for 60 s. The cells were washed with fresh growth medium, and then 100 μL of fresh growth medium and 10 μL of WST-1 mixture solution were added to each well. After incubation of the cells for 3 h at 37°C, a microplate reader (Thermo Fisher Scientific, Waltham, MA) was used to measure the absorbance at a wavelength of 450 nm, with a reference wavelength of 630 nm. The results are presented as a percentage of the untreated cells.
Evaluation of physicochemical properties
The zeta potential was measured for the surface charge of the particles. Zeta potential is defined as the potential difference between the dispersion medium and the stationary layer of fluid that is attached to the dispersed particle. The particle size and zeta potential for each agent were measured using the Zetasizer Nano ZS (Malvern Instruments, Malvern, Worcestershire, UK). Measurements were performed 13 and 15 times for the particle size and the zeta potential, respectively. The temperature was maintained at 25°C throughout the measurement period.
Statistical analysis
The results were expressed as the mean±standard error of at least 3 experiments. Statistical comparisons were performed by analysis of variance followed by the Tukey-Kramer test for the TER measurement and cytotoxicity assay. The Student's t-test was used to analyze the measurement of the particle size and zeta potential. Values of P<0.05 were considered to indicate statistical significance.
Results
Corneal exposure to travoprost Z, travoprost, and 0.015% BAC
The mean corneal TER for the live rabbits used in this study was 701.6±43.1 Ω·cm2 (52 eyes). Figure 1 shows the TER changes that occurred after corneal exposure to HBSS, travoprost Z, travoprost, and 0.015% BAC. While there was no change in the corneal TER after exposure to HBSS or to the travoprost Z, which did not contain BAC, a significant decrease of the corneal TER was observed after the exposure to 0.015% BAC. However, no decrease in the TER was observed after corneal exposure to travoprost, regardless of whether it contained 0.015% BAC.

Corneal TER changes after a 60-s exposure to travoprost Z (without BAC), travoprost (containing 0.015% BAC), or 0.015% BAC. Data represent the percentage to pre-exposure TER value (100%). Each value is the mean±SE (n=4–5). **P<0.01 as compared with HBSS, travoprost Z, and travoprost. TER, transepithelial electrical resistance; BAC, benzalkonium chloride; HBSS, Hank's balanced salt Ca2+- and Mg2+-free solution; SE, standard error.
Corneal exposure to travoprost additives with or without 0.02% BAC
The concentration of BAC was set at 0.02% in the subsequent experiments, as this is the highest concentration that is normally applied in commercial eye drops. The influence of the travoprost additives on the TER changes was analyzed by examining each additive in the presence and absence of 0.02% BAC (Fig. 2). Data for the negative and positive controls were obtained by exposing the cornea to only HBSS or to BAC, respectively. As shown in Fig. 2A, there were no corneal TER changes noted for any of the additives. While mixing HCO-40 with BAC prevented BAC-induced corneal barrier dysfunction, EDTA, boric acid, mannitol, and trometamol were not able to modulate BAC toxicity (Fig. 2B).

Corneal TER changes after a 60-s exposure to travoprost additives in the absence
Scanning electron microscopy observation
After exposure to HBSS, the scanning electron microscopy (SEM) images in the control corneal epithelium exhibited a normal appearance of superficial cells with a high density of microvilli (Fig. 3). However, after exposure to 0.02% BAC, there was detaching and wrinkling of the superficial cells, dissociations between the cells, and degenerated microvilli observed in the corneal epithelium (Fig. 4). Conversely, no damage to the corneal epithelium was observed after it was exposed to a solution of 0.02% BAC and 1% HCO-40 (Fig. 5).

Scanning electron microscopy images of the corneal epithelium after a 60-s corneal exposure to HBSS. Magnification: 300×
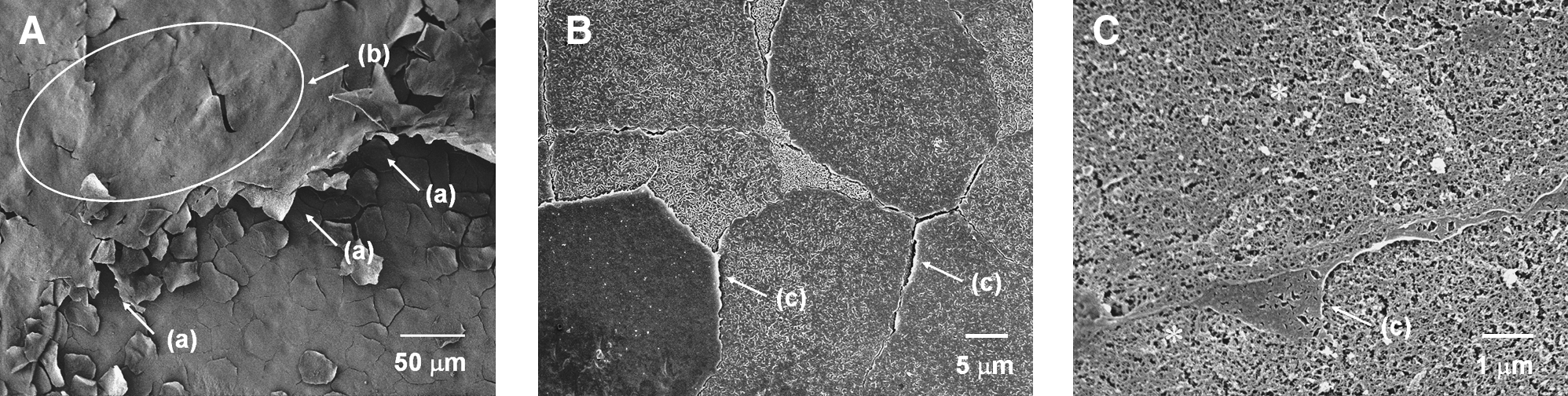
Scanning electron microscopy images of the corneal epithelium after a 60-s corneal exposure to 0.02% BAC. Magnification: 300×

Scanning electron microscopy images of the corneal epithelium after a 60-s corneal exposure to 0.02% BAC with 1% HCO-40. Magnification: 300×
Cytotoxicity assay
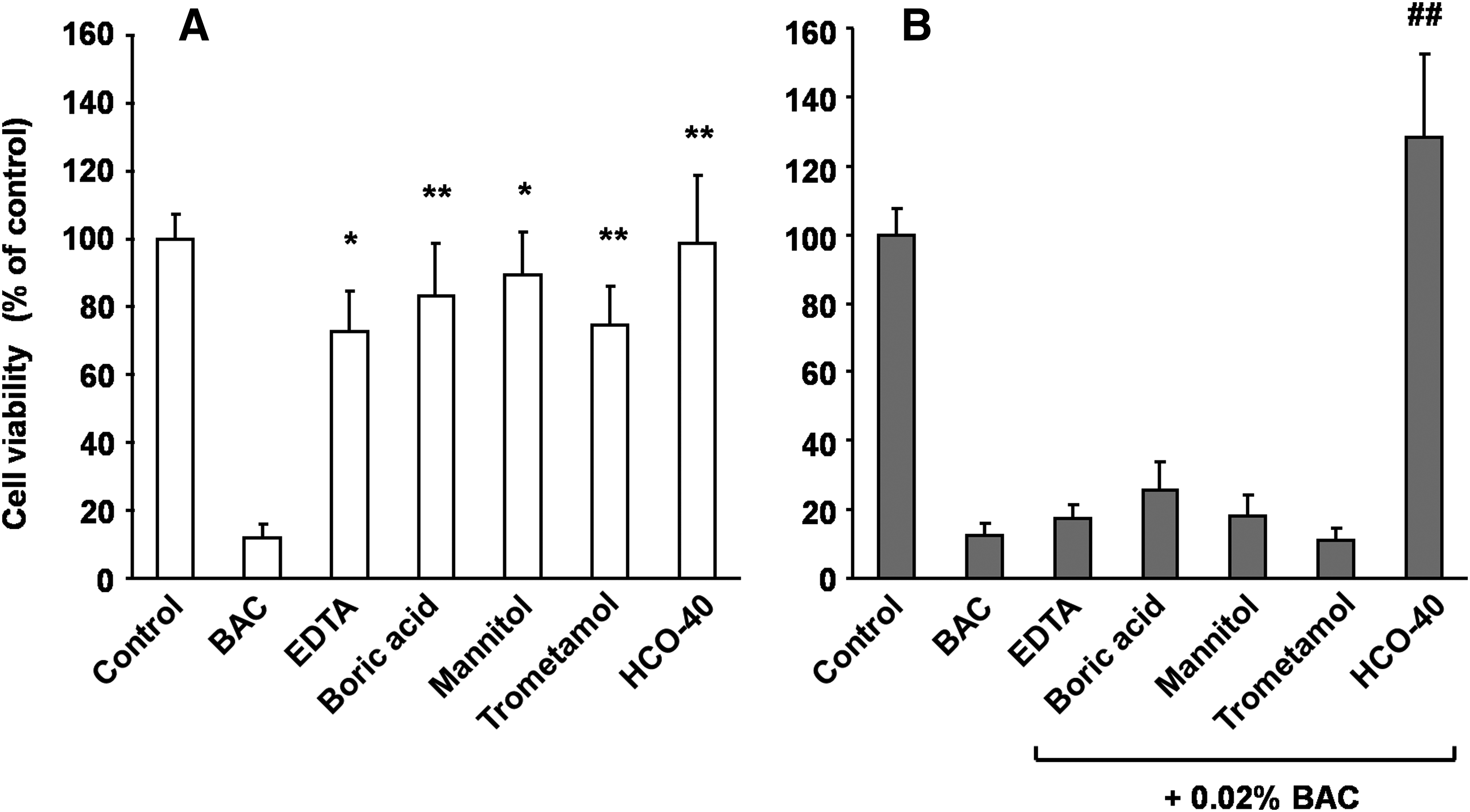
Cytotoxicity of the travoprost additives on the NRCE cells was examined by a WST-1 assay in the presence and absence of 0.02% BAC (Fig. 6). Exposure to BAC by itself was used as the positive control. As shown in Fig. 6A, none of the additives caused any significant decrease in the cell viability as compared with untreated cells (control). While mixing HCO-40 with BAC decreased the cytotoxicity of the BAC, EDTA, boric acid, mannitol, and trometamol did not prevent the cytotoxicity (Fig. 6B).
Cytotoxicity assay of travoprost additives to NRCE cells in the absence
Physicochemical properties of BAC, HCO-40, and HCO-40 with BAC
To elucidate the modulation mechanism of HCO-40, the particle size and zeta potential of either 0.02% BAC alone or 1% HCO-40 solution with or without 0.02% BAC were measured (Table 1). The particle size and zeta potential of 0.02% BAC could not be detected. With 1% HCO-40, which forms dispersion, the mean particle size was 25.7 nm and the mean zeta potential was −0.8 mV. On the other hand, after adding 0.02% BAC to 1% HCO-40, the particle size decreased from 25.7 to 13.5 nm and the zeta potential increased from −0.8 to +18.5 mV.
Each value is the mean±standard error (n=3).
p<0.01, as compared with 1% HCO-40.
ND, not detected; BAC, benzalkonium chloride; HCO-40, hydrogenated castor oil 40.
Discussion
Most commercially available prostaglandin analogs contain BAC, which is associated with ocular surface side effects. Currently, new prostaglandin analog formulations that do not contain BAC are being developed. In one of these new agents, travoprost Z, BAC has been replaced with sofZia, which is a non-BAC preservative system that contains boric acid, sorbitol, propylene glycol, and zinc chloride. Several comparative studies of ocular surface changes induced by prostaglandin analogs have shown that travoprost Z causes significantly less corneal and conjunctival toxicity as compared to the latanoprost ophthalmic solution that contains 0.02% BAC.21–24 In these reports, however, comparisons of travoprost Z with travoprost were not performed. Therefore, we decided to evaluate the corneal toxicity of travoprost Z and travoprost using a newly developed electrophysiological method.
The cornea is generally recognized as the major route of ocular penetration for topically instilled drugs. It is composed of 5 layers, which include the epithelium, Bowman's membrane, stroma, Descemet's membrane, and the endothelium. Among these 5 layers, the barrier function that protects against foreign matter primarily depends upon the epithelium, which is composed of superficial cells, wing cells, and basal cells. Superficial cells and the tight junctions that are found between them play a major role in the epithelial barrier function.25,26 TER can be mathematically described as follows: TER=Rtj×(Ra+Rb)/(Rtj+Ra+Rb). Apical and basolateral cell membrane electrical resistances are, respectively, represented as Ra and Rb, whereas the tight junctional electrical resistance is represented as Rtj. Corneal TER reflects the electrical resistances of the superficial cells and the tight junctions. In addition, TER is a highly sensitive electrophysiologic parameter that can be used to measure the epithelial barrier change, with lower corneal TER values indicative of the penetration of greater amounts of electrical current through the damaged superficial cells and tight junctions.8,18,27–32
We have recently developed an in vivo corneal TER measurement system that makes it possible to measure corneal changes both continuously and quantitatively within only a few seconds. 18 The ability to evaluate eye drop-induced corneal toxicity over a short period is invaluable, as normally tears dilute the eye drops immediately after instillation. 33 By using this method, we determined that the TER of the cornea of normal live rabbits was 701.6±43.1 Ω·cm2, which is considered to be an adequate value when compared to previous reports that have measured the corneal TER.18,19,28–30 After exposure to travoprost Z, which uses sofZia as the preservative system, TER exhibited almost the same results as those of the negative control, HBSS. This suggests that travoprost Z does not cause acute corneal barrier dysfunction. On the other hand, 0.015% BAC caused a dramatic reduction of TER. Our previous experiments have indicated that routine clinical concentrations (0.005%–0.02%) of BAC can cause an intense concentration-dependent decrease in the TER. 19 Further, it has been reported in a previous study that used isolated rabbit cornea that commercial eye drops containing BAC resulted in a lowering of the TER. 32 However, when there was exposure to travoprost that contained 0.015% BAC, no significant changes were noted in the TER. The finding that travoprost, similar to travoprost Z, maintained the pre-exposure TER values was totally unexpected. Therefore, we believe that valuable information could potentially be discovered by more closely examining the mechanism used by travoprost to inhibit the BAC-induced corneal barrier dysfunction. Thus, we performed further experiments that electrophysiologically examined the influence of the travoprost additives on BAC.
The additives contained within the travoprost solution include EDTA, boric acid, mannitol, trometamol, HCO-40, and BAC. While there was no suppression of the BAC-induced TER decrease for EDTA, boric acid, mannitol, and trometamol, HCO-40 was found to remarkably prevent the BAC-induced corneal barrier dysfunction during the acute phase. Both SEM and a cytotoxicity assay confirmed these results. SEM-based histological analyses of the control corneas indicated that the appearance of the superficial layer was good and that there was clear damage of the corneal epithelium in corneas exposed to 0.02% BAC. These corneal epithelial images are consistent with previously published reports.4–7,18,34 The results of the NRCE cell viability assay after exposure to travoprost additives with or without BAC were similar to the results of the TER measurements. When HCO-40 was added to BAC, remarkable improvement of the BAC-induced corneal epithelial toxicity was noted for both the SEM and cytotoxicity assay results. This supports our belief that HCO-40 provides protection against the BAC-induced corneal toxicity that occurs with travoprost.
Protective effects against BAC-induced ocular toxicity have also been reported for hyaluronic acid.35–37 These studies also postulated that the mechanism of this protective effect could possibly be related to the ionic attraction between the positive charge of BAC and the negative charge of the hyaluronic acid, with the ionic complexes able to neutralize the toxic effect caused by the cationic charge of BAC. It was also suggested that part of the action might be caused by the penetration and subsequent dispersal of BAC within the sponge-like domain of the hyaluronic acid.
HCO-40 and BAC, however, are nonionic and cationic surfactants, respectively. These agents consist of 2 components that include a large nonpolar hydrocarbon chain that attracts hydrophobic substances along with a hydrophilic group that is strongly attracted by water molecules. Based on this, the protective mechanism of HCO-40 should differ from hyaluronic acid, which is composed of disaccharides. To elucidate this modulation mechanism, we decided to measure the particle size and zeta potential of BAC alone followed by the measurement of HCO-40 in the absence and presence of BAC. The particle size and zeta potential of 0.02% BAC were not detectable, as 0.02% BAC was much lower than the required 5 mM (approximately 0.2%) critical micelle concentration. 38 On the other hand, measurement of 1% HCO-40 found that there was a 25.7-nm mean particle size that had a slightly negative surface charge. Furthermore, the addition of 0.02% BAC, which had a cationic charge, induced a reduction of the particle size and modified the surface charge from negative to positive. These results indicate that the micelles of the 1% HCO-40 with 0.02% BAC have a coating layer of BAC molecules. When the BAC molecules combine with the micelles, there is strong hydrophobic and ionic bonding that reduces the particle size. Therefore, these findings suggest that the protective effect of HCO-40 is induced by an interaction between HCO-40 and BAC. If so, then a decrease in the amount of free BAC molecules that attach to the corneal epithelium should be observed. To definitively elucidate the details of the protective mechanism of HCO-40, further studies will be necessary. Furthermore, this study only examined the corneal epithelial change that occurred in animal corneas during the acute phase. It should be noted that the current study was not able to sufficiently clarify whether chronic corneal epithelial impairment occurs after long time usage of these drugs in humans.
In general, ophthalmic formulations that contain high concentrations of the preservative BAC are associated with corneal toxicity. However, results from the present study indicate that BAC concentrations listed on a label do not always reflect whether there will be an eye drop-caused acute corneal toxicity. When considering this potential toxicity, it is also necessary to examine the possible interaction of BAC with the other ophthalmic additives.
In conclusion, our results demonstrated that travoprost preserved with either sofZia or 0.015% BAC did not cause acute cornel barrier dysfunction and that HCO-40 can modulate the BAC-induced corneal toxicity.
Footnotes
Acknowledgments
The authors thank Yumiko Tsunenari (Department of Ophthalmology and Visual Sciences, Graduate School of Biomedical Sciences, Nagasaki University) for her technical assistance with the SEM observations and Dr. Takurou Niidome (Department of Applied Chemistry, Faculty of Engineering, Kyushu University) for his assistance with the Zetasizer Nano ZS measurement. The authors also thank Tomoaki Kurosaki (Nagasaki University Hospital of Medicine and Dentistry) for his advice and instruction.
Author Disclosure Statement
No competing financial interests exist.