
Abstract
Abstract
Purpose:
To determine the incidence of eyes that have an increase in the intraocular pressure (IOP) after subtenon injections of triamcinolone acetonide (TA).
Methods:
The medical records of 147 patients treated with single or multiple subtenon injections of TA (10 mg) were reviewed. The incidence of an IOP elevation (ΔIOP) ≥5 mmHg or an IOP of >21 mmHg was determined. The peak ΔIOP, defined as the difference in the IOP at the peak to the baseline IOP, was also evaluated. Multivariate analyses were used to evaluate the relation between the IOP elevation and the age, gender, refractive error, and lens status.
Results:
A ΔIOP ≥5 mmHg was found in 75 eyes (46%), and an IOP >21 mmHg was found in 48 eyes (30%) after a single injection of TA. The IOP increased within 3 months in 39 eyes (81%) and after 4 months in 9 eyes (19%). The IOP began to increase significantly from 2 weeks up to 5 months (P<0.05) and returned to the baseline IOP in 10 months. The incidence of ΔIOP ≥5 mmHg or an IOP of >21 mmHg after multiple subtenon injections of TA was significantly higher than after a single injection (62%; P=0.027, 47%; P=0.013, respectively). The incidence of IOP >21 mmHg and the peak ΔIOP were significantly related with younger age (P=0.002, P=0.021, Forward stepwise regression analysis). A weak but significant negative correlation was found between the peak ΔIOP and the age (r=−0.216, P=0.006, Pearson's correlation coefficient test), and the peak ΔIOP and the refractive error (r=−0.198; P=0.018).
Conclusion:
Repeated injections of TAs and injection of younger patients or myopic eyes increase the incidence of an IOP elevation.
Introduction
An intravitreal injection is less frequently used because of the risk of endophthalmitis and retinal detachments, and a subtenon injection is preferred because of its safety and convenience.5,6 It has been reported that an increase in the intraocular pressure (IOP) can develop after injections of TA and other corticosteroids to cause steroid-induced ocular hypertension.7,8 Since TA is weakly water soluble and long-acting, the IOP elevations can occur several months after the injection, and the increase in the IOP can last for several months. This complication can result in some eyes having to undergo laser treatment and/or filtering surgery.9–12 In spite of the earlier studies, the exact incidence of eyes that have an increase in the IOP after a subtenon injection of TA has not been published. 13
The purpose of this study was to determine the incidence of an elevation of the IOP after single or multiple injections of TA. To accomplish this, we reviewed the medical records of cases that had received either single or multiple subtenon injections of TA for several retinal disorders associated with major retinal vascular pathologies.
Methods
Subjects
A retrospective case series study was conducted on 162 eyes of 147 patients (79 men, 68 women) who had received single or multiple subtenon injections of 10 mg TA. There were 38 eyes of 26 patients with diffuse diabetic macular edema, 64 eyes of 63 patients with branch retinal vein occlusion, 10 eyes of 9 patients with central retinal vein occlusion, 39 eyes of 38 patients with exudative age-related macular degeneration, 7 eyes of 7 patients with idiopathic choroidal neovascularization, and 4 eyes of 4 patients with macular edema by other ocular diseases that were treated with TA.
The patients had been treated at the Keio University Hospital between June 2002 and January 2007 and were followed for at least 4 months. None of the patients had received an earlier subtenon injection of other corticosteroids. The baseline IOP was measured at least twice at different times on different days before the injection, and patients in whom glaucoma was diagnosed or had a baseline IOP >21 mmHg were excluded. The anterior chamber angle of all patients was open without any evidence of neovascularization.
A written informed consent was obtained from all patients after a full explanation of the purpose and possible complications of the subtenon TA injection. The Ethics Committee of Keio University approved the use of TA including possible additional treatments based on recommendation of the Institutional Review Board. The procedures used conformed to the tenets of the Declaration of Helsinki.
Procedures for subtenon TA injections
To prepare 10 mg of TA, 0.25 mL containing 10 mg of TA (Kenacort-A®, 40 mg/mL; Bristol Myers KK, Tokyo, Japan) was aspirated into a 1 mL syringe. The syringe was placed in a holder for several minutes, and after the crystals of TA had settled on the bottom, the supernatant was reduced to a volume of 0.1 mL. Immediately before the subtenon injection, the mixture in the syringe was shaken well to make a uniform suspension of the TA crystals.
Before the TA injection, the eye was anesthetized with several drops of 4% lidocaine. An eye speculum was used, and the patient was asked to look inferonasally to expose the superotemporal bulbar conjunctiva. A 26-gauge needle was inserted superotemporally into the subtenon space by gently moving the tip of the needle to avoid penetrating the globe. The tip of the needle was not sharp and was similar to the needle attached to a tuberculin syringe.
IOP measurements
The IOP was measured by Goldmann aplanation tonometry. Patients were examined at ∼2 weeks and at 1 month after the TA injection. Thereafter, the follow-up examinations were done monthly. The incidence of IOP elevation (ΔIOP) ≥5 mmHg from the IOP before the injection (baseline IOP) and the incidence of IOP increased to >21 mmHg in any period after TA injection were evaluated. The peak ΔIOP, defined as the difference in the IOP at the peak elevation from the baseline IOP, was also evaluated. If the IOP exceeded 25 mmHg, topical beta-blockers, prostaglandin derivatives, or carbonic anhydrase inhibitors were given. If the IOP continued to be elevated, different combinations of these drugs were used. Selective laser trabeculoplasty (SLT) was usually performed if the IOP continued to be higher than 40 mmHg despite the maximum medication including systemic carbonic anhydrase inhibitors. The eyes that underwent SLT were included in the analysis on the ΔIOP but not included in the analysis evaluating the course of the IOP elevation after the treatments with SLT. The eyes that underwent cataract and/or vitreous surgery during the observation period or simultaneously with the TA injection were excluded to eliminate bias of the host factors.
The topical medication score was defined as the number of anti-glaucoma eye drops being used, and the scores were assessed before and after the TA injection. Statistical analyses were performed by a commercial statistical software package. Paired t-tests were used to assess the significance of differences in the IOPs before and after the TA injections. Fisher's exact probability tests were used to evaluate the significance of the ΔIOP. Forward stepwise regression analysis was used to evaluate the relationship between IOP elevation (IOP >21 mmHg or ΔIOP ≥5 mmHg, or the peak ΔIOP) and age, gender, refractive error, and lens status. Pearson's correlation coefficient test was used to determine the relationship between the age and the refractive error, or the age and the peak ΔIOP. The level of significance was 0.05 for all statistical tests.
Results
Incidence of elevation in IOP
A total of 311 subtenon TA injections were given to the 162 eyes. The mean age of the patients was 62.9±11.9 years (±standard deviation) with a range from 30 to 86 years. The mean baseline IOP before a single TA injection was 14.4±3.5 mmHg with a range from 8 to 21 mmHg (Table 1). A ΔIOP ≥5 mmHg was found in 75 eyes (46%), and an IOP >21 mmHg was found in 48 eyes (30%) after a single injection of TA. After a single injection of TA, a ΔIOP ≥5 mmHg was observed at 2 weeks to 8 months (mean 2.2 months) after the injection (Fig. 1). The mean IOP was elevated significantly for 2 weeks to 5 months. The mean peak ΔIOP was 17.3±6.0 mmHg (range from 8 to 62 mmHg), which was attained at 2 months after the TA injection. The mean IOP decreased to 15.8±4.7 mmHg (ranged 9 to 35 mmHg) at 6 months after the TA injection, and it was not significantly different from that of the baseline IOP. The mean IOP returned to 14.2±3.1 mmHg (approximate the mean baseline IOP) with reduced numbers of medications at 10 months after the TA injection.
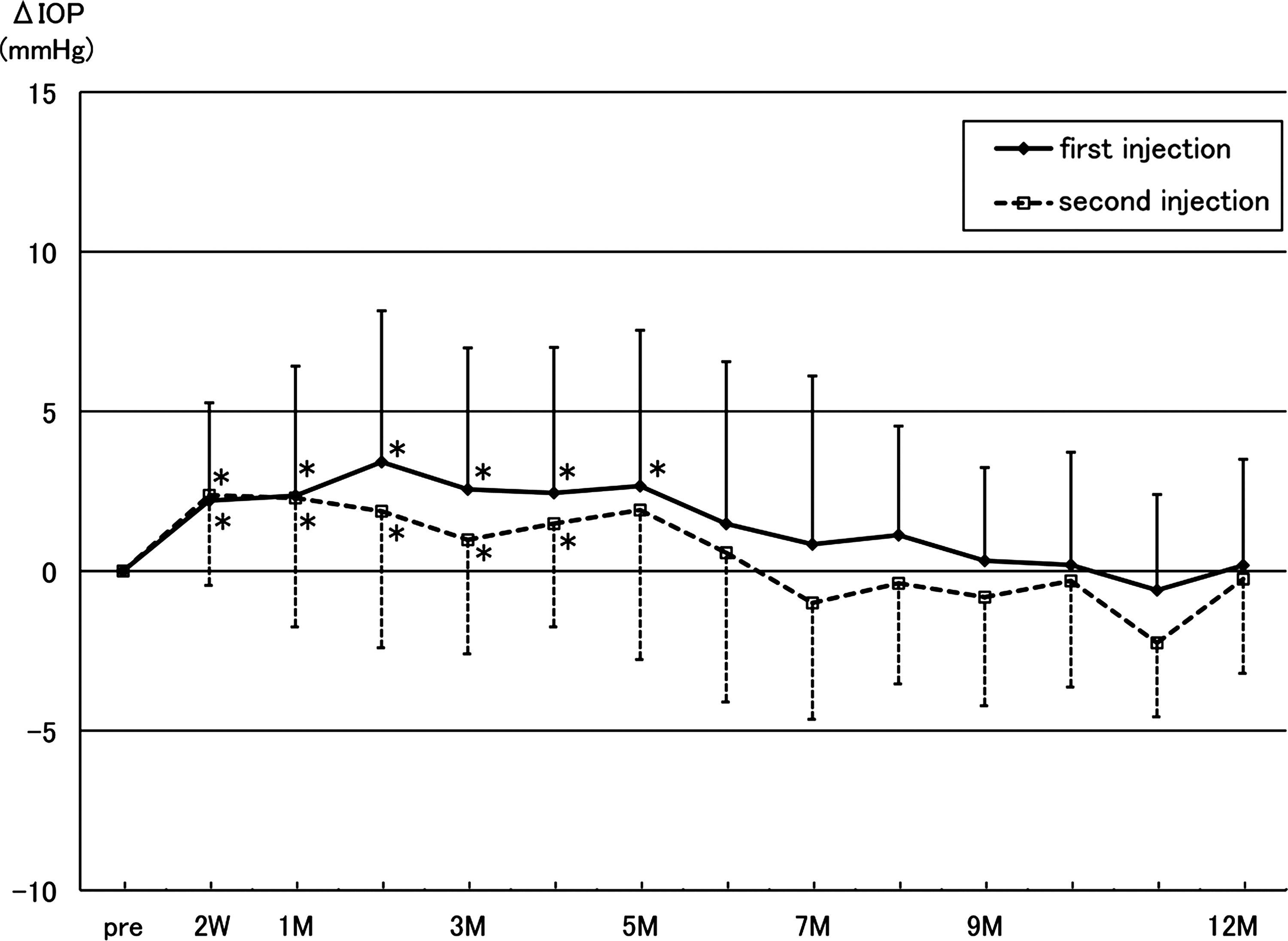
Mean intraocular pressure (IOP) before and after a single and a second injection of TA. The IOPs at 2 weeks, and 1, 2, 3, 4, and 5 months after the injection of TA are significantly higher than the baseline IOP after a single injection. The IOPs at 2 weeks, and 1, 2, 3, and 4 months are significantly higher than the baseline after a second injection (*P<0.05, error bar: standard deviation, Paired t-tests). W, week, M, month; TA, triamcinolone acetonide.
P=0.027.
P=0.013.
P=0.797, Fisher's exact probability test.
IOP, intraocular pressure; ΔIOP, IOP elevation from the baseline IOP.
The IOP began to increase within 3 months in 60 (80%) of the 75 eyes with an IOP elevation ≥5 mmHg after the single TA injection. The increase in the IOP began at 4 months after the injection in the other 15 eyes (20%). The IOP increased to >21 mmHg after a single injection within 3 months in 39 eyes (81%) and in 4 months in the remaining 9 eyes. In 13 of the 162 eyes (8%), the IOP increased to >30 mmHg at 4 months after the injection.
In the 75 eyes with a ΔIOP ≥5 mmHg after a single injection, topical anti-glaucoma medications were given to 33 eyes (44%). The topical medication score was 0 at baseline and increased to 1.1 at 5 months after the single injection (Fig. 2). The score gradually decreased to 0.2 at 10 months after the injection. After a single subtenon injection of TA, SLT was performed on 3 eyes, and the IOPs of all 3 eyes were controlled without any medication at 6 months after the TA injection.
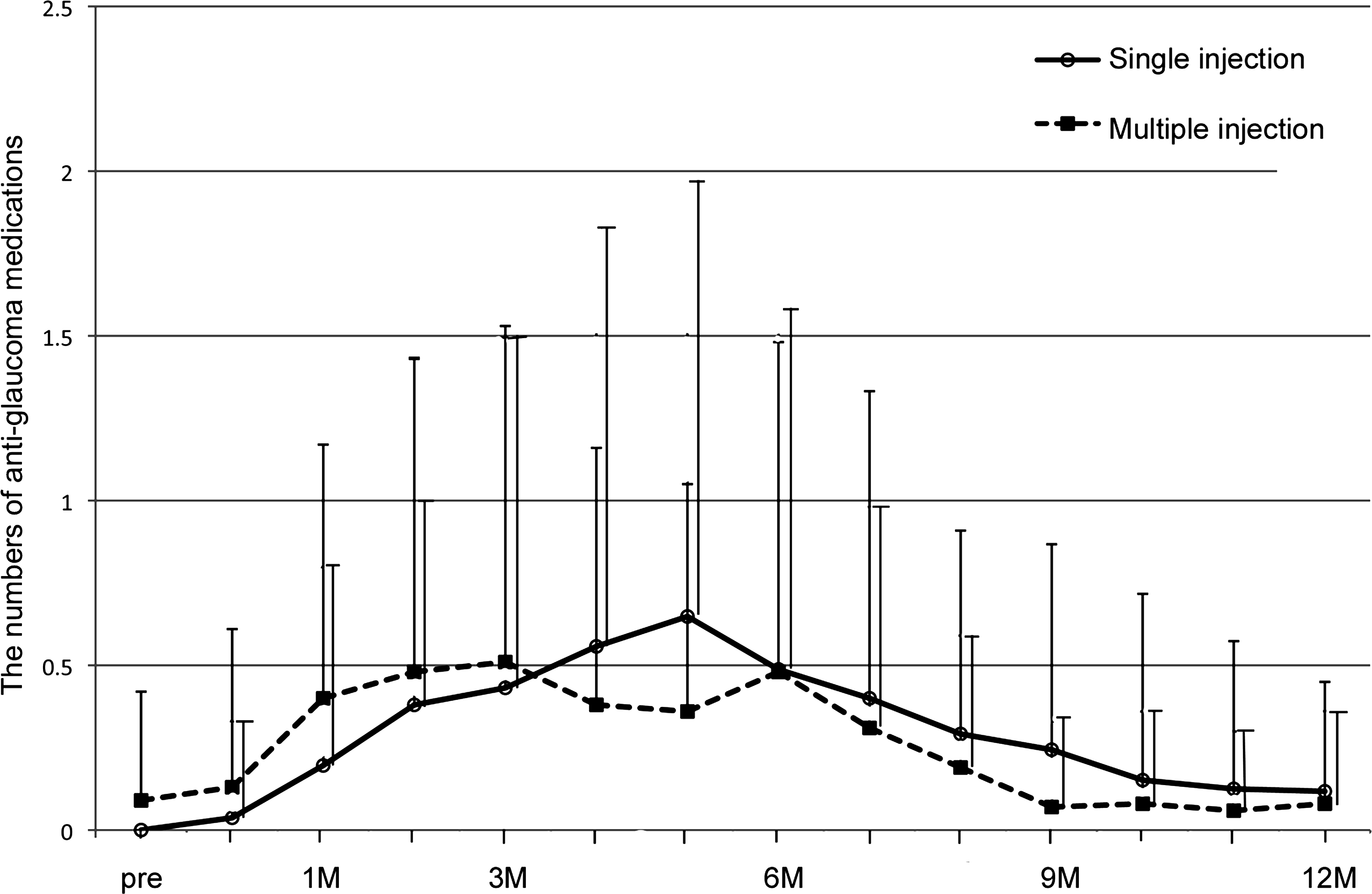
Topical medication score before and after single and multiple injection of TA. The mean number of glaucoma medications increases from 0 to 1.1 at 5 months after the single injection and gradually decreased to 0.2 at 10 months after the injection. The topical medication score was <0.1 before the multiple injections, 0.5 at 4 months after the injection, and 0.2 at 8 months after the injection. The topical medication score rapidly increased compared with eyes with the single injection (error bar: standard deviation, Paired t-tests).
In the eyes that required 2 TA injections, the IOP increased significantly from 2 weeks after the second injection, but the IOP was not significantly higher at 5 months after the injection (Fig. 1). Seventy-seven of the 162 eyes received multiple subtenon injections of TA (Table 1). The incidence of a ΔIOP ≥5 mmHg after multiple subtenon injections of TA was significantly higher than that after a single injection (P=0.027, Fisher's exact probability test). The incidence of an IOP increasing to >21 mmHg was significantly higher than that after a single injection (P=0.013), but the difference in the incidence of an IOP increasing to >30 mmHg was not significant (P=0.797). In the 5 eyes whose IOP increased to >30 mmHg, the IOP elevation was seen within 3 months after the last injection.
Among the 48 eyes whose ΔIOP increased by ≥5 mmHg after multiple injections, anti-glaucoma topical drops were prescribed to 22 eyes (46%). The topical medication score was <0.1 before the additional injections, 0.5 at 4 months after the last injection, and 0.2 at 8 months after the last injection (Fig. 2). The topical medication score was higher than that after the initial single injection although the scores were relatively low.
One hundred and one eyes (62%) of 91 patients with a mean age of 63.3 years including 50 men and 41 women had a ΔIOP ≥5 mmHg at least once after the subtenon injections of TA. Sixty-one eyes (38%) of 56 patients with a mean age of 62.9 years including 29 men and 27 women did not show a ΔIOP ≥5 mmHg after the subtenon injections of TA. There were 15 cases that had subtenon TA injections in both eyes (Table 2), and the incidence of IOP >21 mmHg was 27% (8 eyes) of bilateral injections comparing with 30% (40 eyes) of unilateral injections (P=0.826, Fisher's exact probability test). In 8 eyes with bilateral injections with IOP increased to >21 mmHg, the IOP increased bilaterally in 3 cases (60%) and unilaterally in 2 cases (40%). However, there was a selection bias because both eyes from 15 patients were included in this analysis.
6 eyes of 3 cases and 2 eyes of 2 cases, P=0.826, Fisher's exact probability test.
Relationship between change in IOP elevation and refractive error
One hundred and forty-two of the eyes (88%) of 127 patients were phakic, and 20 eyes of 20 patients were pseudophakic. None of the eyes was aphakic. The effect of the refractive error was only evaluated for the phakic eyes. The mean refractive error in the phakic subjects was −2.3±3.8 diopters (D) with a range from −19.0 D to +2.5 D. In 142 phakic eyes, 91 eyes (64%) of 85 patients including 55 eyes of 50 men and 36 eyes of 35 women had a ΔIOP ≥5 mmHg after single or multiple subtenon injections of TA. The mean refractive error (spherical equivalent) with a ΔIOP ≥5 mmHg was −2.4±3.3 D, and the mean age was 60.5 years. The mean refractive error without a ΔIOP ≥5 mmHg was −2.1±4.7 D, and the mean age was 62.3 years. Forward stepwise regression analysis showed a significant negative correlation between the age and IOP >21 mmHg (P=0.002), and the age and peak ΔIOP (P=0.021, Table 3). The relationship between the age and the peak ΔIOP was calculated by Pearson's correlation coefficient test, and a weak but significant negative correlation was found (r=−0.216, P=0.006; Fig. 3). A weak but significant negative correlation was also found between the refractive error and the peak ΔIOP (r=−0.198, P=0.018; Fig. 4). This indicated that the IOP was more likely to be elevated after a TA injection in younger patients and eyes with higher myopia.
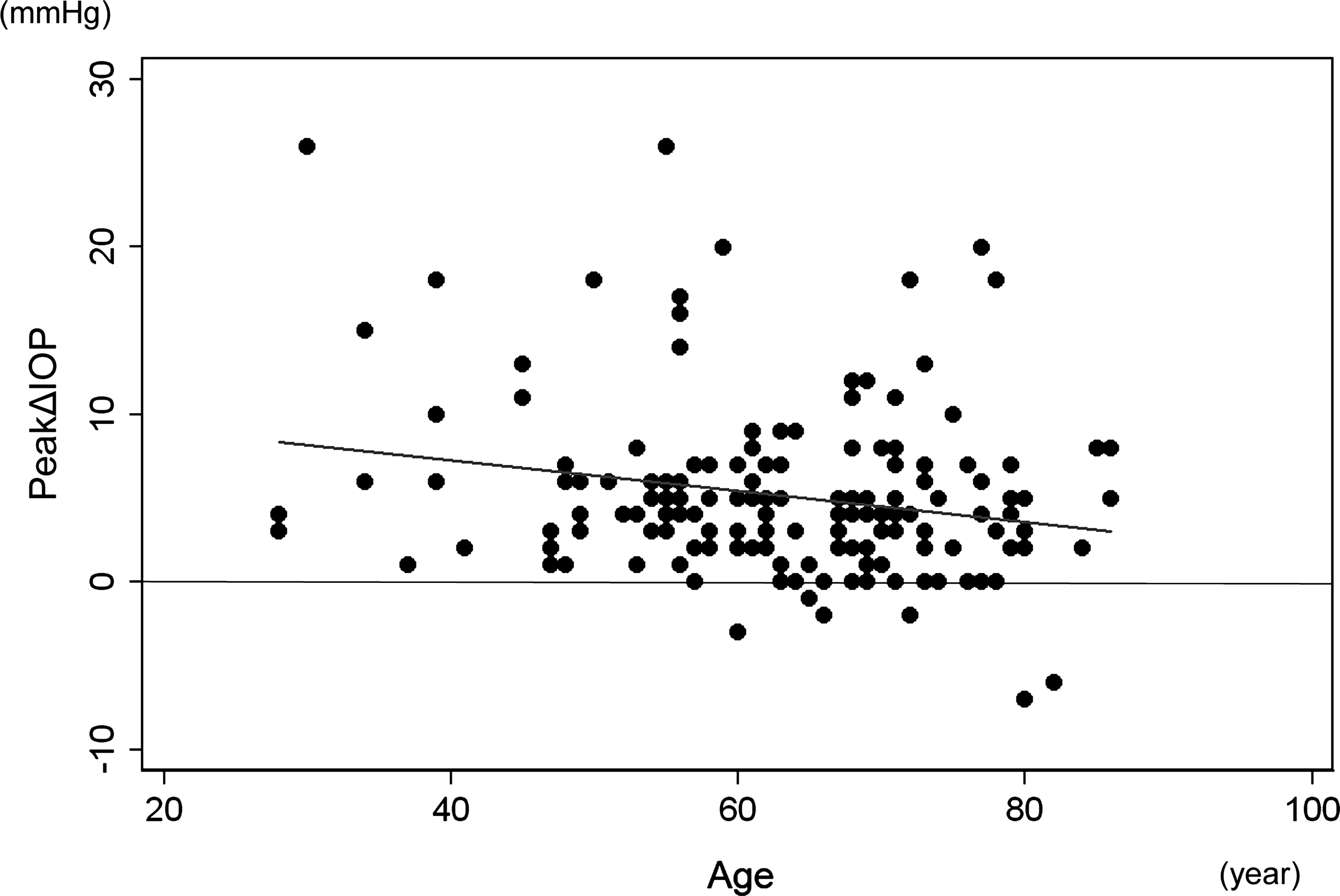
Relationship between the change in the peak ΔIOP (the peak elevation from the baseline IOP) and age. A significant negative correlation exists between the peak ΔIOP and the age, indicating that the IOP increased in younger patients more often than in older patients (P=0.006; r=−0.216, Pearson's correlation coefficient test). ΔIOP, incidence of IOP elevation.
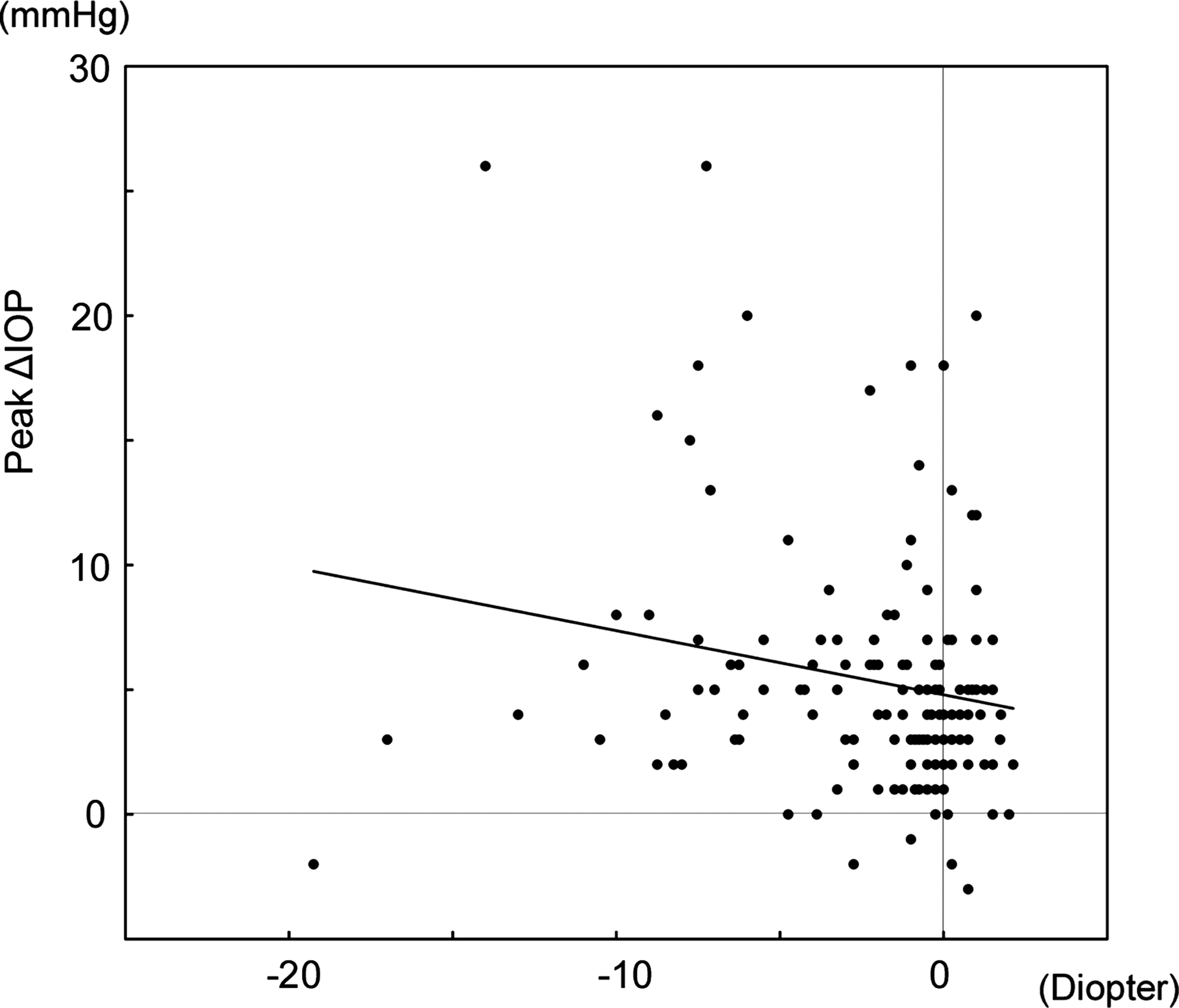
Relationship between the change in the peak ΔIOP (the peak elevation from the baseline IOP) and refractive error. A significant negative correlation exists between the peak ΔIOP and the refractive error, indicating that the IOP in myopic eyes increased more often than in eyes with higher refractive errors (P=0.018; r=−0.198, Pearson's correlation coefficient test).
Forward stepwise regression analysis.
Discussion
An increase in the IOP is the most frequent complication of TA use. The increase in the IOP is usually transient, and the patient is often asymptomatic even when the IOP is elevated to 50 to 60 mmHg, a characteristic of steroid glaucoma. 7 The effect of TA has been reported to last from 3 to 8 months. 14 Thus, careful attention should be paid to the IOP after both types of TA injection, because an increase in the IOP can lead to irreversible optic nerve atrophy, and the elevated IOP can be controlled by topical anti-glaucoma drugs in most cases. However, some cases may require filtering surgery to normalize the IOP.
Helm and Holland reviewed 20 eyes that had received subtenon injections of TA, and they reported that an elevated IOP was found in 6 patients (30%), and 2 of the 6 eyes had received several injections. 13 Mueller and associates studied 54 steroid nonresponders and reported that a subtenon injection of TA (40 mg) was safe and did not cause an increase in the IOP when the deposit was injected into the subtenon space. 15 Levin and associates reported an increase in the IOP in 4 of 9 patients (44%) who were steroid-responders and 7 of 55 patients (13%) who were steroid nonresponders. 16 Some patients had an IOP elevation after a subtenon injection of TA even in steroid nonresponders. These findings indicated that the conventional steroid response test cannot clearly differentiate the eyes that will have an elevation of the IOP after subtenon TA.
Ito and associates reported that the IOP increased to >21 mmHg in 41 eyes (34.5%) of 119 eyes after intravitreal and subtenon injections of TA, and an IOP increased by >5 mmHg from the baseline was found in 59 eyes (49.6%). 17 It has also been reported that the ΔIOP was higher in younger patients and also after repeated injections. 17 Jonas and associates also reported that the IOP increased to >21 mmHg in 39 (52%) of 75 eyes after an intravitreal injection of TA, and one of these cases required trabeculectomy.7,18 The dose of TA for subtenon injection was usually 20 to 40 mg, which was more than that of an intavitreal injection of 4 to 20 mg. An intravitreal injection of TA is believed to affect the trabecular meshwork in the angle more directly than the subtenon injection. This may be why a delayed IOP elevation was observed after subtenon TA injection in our study.
We injected the TA into the posterior subtenon space around the equator of the eye, and 46% of the cases had an elevated IOP within 2 months after the initial subtenon injection of TA. By 3 months, 80% of the eyes had developed an IOP elevation. However, cases of late-onset IOP elevation were present in our series, and repeated injections of TA may increase the risk of an IOP elevation. An IOP elevation was observed in 20% of our cases beginning 4 months after the TA injection. This suggests that a repeat TA injection within 4 months of a previous injection might increase the risk of IOP elevation. There may be a potential bias in our delay in giving the second injection when the IOP had risen after the initial injection. Thus, the incidence of IOP elevation after repeated injections would be higher than that stated earlier. Thus, repeated injections should be considered more carefully to avoid the risk of ocular hypertension.
A significant correlation was found between an IOP elevation and younger age and gender. 19 A weak but significantly negative correlation between refractive error and IOP elevation was found in our cases, indicating that more attention should be paid to younger patients and those with high myopia. In an earlier report, the authors recommended that patients should be tested for the presence of a positive steroid response by applying a topical steroid before the use of TA, and TA should be avoided if the patient was a steroid-responder. 16 However, our results showed that the IOP elevation could be controlled in most of the cases by topical anti-glaucoma drugs. In addition, we found that some patients had an elevation of the IOP unilaterally after a bilateral injection of TA. Thus, we believed that an elevated IOP after TA is probably more complex than expected from the presence of topical steroid response. The mechanism for the significant correlation between high myopia and an elevation of the IOP requires further study.
In conclusion, a subtenon injection of TA has been used for treatment, but can be a high risk of an IOP elevation. However, the elevated IOP is transient. We recommend frequent measurements of the IOP and long-term observations in patients who have had a subtenon or an intravitreal injection of TA, because cases with late-onset increases in the IOP can be present and retreatment with TA increases the risk of IOP elevation.
Footnotes
Acknowledgments
None of the authors has a financial or proprietary interest in any material or method mentioned.
Author contributions
Design of the study (R.K., M.I., K.S., K.T.); Conduct of the study (R.K., M.I., K.S., S.I., K.T.); Collection and Analysis of the data (R.K., H.S., Y.I.); Literature Search (R.K., M.I., K.S.).
Author Disclosure Statement
No competing financial interests exist.