
Abstract
Abstract
Purpose:
To determine the characteristics of the keratitis due to Colletotrichum gloeosporioides.
Methods:
The medical records of 3 cases of fungal keratitis caused by C. gloeosporioides were reviewed to determine the clinical characteristics. The minimal inhibitory concentrations of different antifungal drugs for all 3 isolates were determined. All 3 isolates were grown on Sabouraud dextrose agar at 25°C, 35°C, and 37°C to determine the temperature-sensitive growth.
Results:
All 3 patients lived in the southwestern part of Japan and had an ocular trauma involving organic materials. The infectious foci were localized in the anterior stroma, and they did not extend deep into the stroma in all cases. The keratitis was treated with antifungal medications including topical voriconazole and natamycin eye ointment, and was resolved in 2–3 weeks. All of the isolated strains grew well at 25°C but poorly at 35°C and 37°C. All isolated strains had similar drug-sensitivity profiles; they were sensitive to amphotericin B, itraconazole, miconazole, micafungin, and voriconazole, and relatively resistant to flucytosine, fluconazole, and natamycin.
Conclusions:
All 3 cases of C. gloeosporioides keratitis had similar clinical features. The similarities in the drug-sensitivity profiles should be helpful in treating C. gloeosporioides keratitis.
Introduction
The filamentous fungal plant pathogens belonging to the genus Colletotrichum are rare pathogens in humans, and the incidence of Colletotrichum infection in humans is low. Thus, Fernandez et al. reported that Colletotrichum was the cause of the fungal keratitis in 10 of 360 cases of keratitis (2.8%). 4 Later, Kaliamurthy et al. reviewed the cases of Colletotrichum keratitis, 5 and reported that the principal causes for Colletotrichum keratitis were ocular trauma, diabetes mellitus, and corticosteroid use. However, the number of reports on Colletotrichum corneal infection is still small, and a detailed characterization of Colletotrichum keratitis has not been published.4–13
We present the clinical characteristics of 3 patients with C. gloeosporioides keratitis, and we present the temperature and drug sensitivities of the isolated strain.
Methods
The medical records of 3 patients with C. gloeosporioides keratitis were reviewed, and the findings in these 3 patients are summarized in Table 1. Three isolates from corneal scrapings were sent to First Laboratory in Medical Mycology Research Center, Chiba University, for DNA sequencing and for determining the minimal inhibitory concentrations (MICs) of different antifungal drugs. The MIC of natamycin was determined by modified agar plate dilution method at the Department of Infection Control, Osaka University Hospital.14,15 All 3 isolates were also grown on Sabouraud dextrose agar at 25°C, 35°C, and 37°C for 5 days to determine the temperature sensitivities at the Clinical Laboratory, Ehime University Hospital.
DM, diabetes mellitus; MCZ, 0.1% miconazole; S-VCZ, systemic voriconazole; VCZ, 1% voriconazole; PM, pimaricin eye ointment; MFLX, moxifloxacin; LVFX, levofloxacin; SD, surgical debridementx; PKP, penetrating keratoplasty; NP, not provided.
The protocol for this study was approved by Institutional Review Board of Ehime University. An informed consent for the examination was obtained from all subjects, and the procedures used conformed to the tenets of the Declaration of Helsinki.
Results
Case reports
Case 1
The patient was an 80-year-old woman who felt dust particles blow into her right eye during farm work on October 13, 2008. She visited a private ophthalmological clinic and was treated with topical gatifloxacin and 0.1% betamethasone for 2 days. Since the symptoms did not improve, she was referred to the Ehime University Hospital on October 17, 2008.
On our initial examination, her best-corrected visual acuity (BCVA) was 20/2000 in the right eye, and slit-lamp examination showed a grayish, superficial stromal infiltrate on the cornea with a dry texture appearance and indistinct margins. Hypopyon was detected in the anterior chamber (Fig. 1A).

Slit-lamp photographs of case 1
Examination of the cornea with the HRT II-RCM confocal scanning microscope (Heidelberg Engineering, Heidelberg, Germany) showed a mass of interlocking and branching white lines in the area of the infiltrate, thus suggesting filamentous fungus keratitis (Fig. 2A). Microscopic examinations of corneal scrapings showed filamentous fungal hyphal fragments. Treatment was begun with oral voriconazole (400 mg/day), topical 0.1% voriconazole hourly, natamycin eye ointment 5 times/day, and topical 0.5% levofloxacin 4 times/day. After beginning the antifungal therapy, the hypopyon resolved in a few days, and the focal infiltrate resolved within 2 weeks. The medications were then tapered over a 3-month period, and the BCVA in her right eye improved to 20/25.

HRT II-RCM images from case 1
Case 2
The patient was a 71-year-old woman who felt pain in her left eye during farm work on September 10, 2009. She visited a private ophthalmological clinic on the next day and was treated with topical gatifloxacin for 5 days. She was referred to the Ehime University Hospital on September 15, 2009 because of uncontrollable corneal inflammation.
On our initial examination, her BCVA was 20/16 in the right eye and 20/80 in the left eye, and slit-lamp examination of the right eye showed a grayish, superficial corneal stromal infiltrate with a dry texture appearance and indistinct margins (Fig. 1B). Examination of the cornea with the HRT II-RCM showed a mass of interlocking and branching white lines in the area of the infiltrate, thus suggesting filamentous fungus keratitis (Fig. 2B). Microscopic examinations of corneal scrapings showed filamentous fungal hyphal fragments. Treatment was begun with topical 0.1% voriconazole hourly, natamycin eye ointment 5 times/day, and 0.1% moxifloxacin 6 times/day. After beginning the antifungal therapy, the size of the focal infiltrate rapidly decreased and resolve within 3 weeks. The medications were then tapered over a 2-month period, and the BCVA in her right eye improved to 20/16.
Case 3
The patient was a 60-year-old man whose right eye was injured by a branch of a mandarin orange tree during farm work on December 12, 2008. He visited the Ideta Eye hospital because of a worsening of the pain and conjunctival injections in his right eye on January 9, 2009. His BCVA at the initial examination was 20/300 in the right eye. Slit-lamp examination of the right eye revealed a grayish, round, superficial corneal stromal infiltrate at the 3’o clock position (Fig. 1C). Microscopic examination of corneal scrapings showed filamentous fungal hyphal fragments. Treatment was begun with topical 0.1% voriconazole and 0.1% miconazole hourly, natamycin eye ointment once a day, and topical 0.5% levofloxacin 4 times/day. After beginning the antifungal therapy, the focal infiltrate resolved within 3 weeks. The medications were then tapered over a 3-month period; however, the BCVA in his right eye did not improve due to macular degeneration.
Laboratory data
The corneal scrapings grew brownish-black fungal colonies on Sabouraud dextrose agar (Fig. 3). Microscopic examination of the colonies showed cylindrical conidia with hyphae (case 2, Fig. 4A) and brownish appressoria, which are features characteristic of C. gloeosporioides (case 2, Fig. 4B). The isolates from all 3 cases were confirmed to be C. gloeosporioides by DNA sequencing by the First Laboratory in Medical Mycology Research Center, Chiba University.
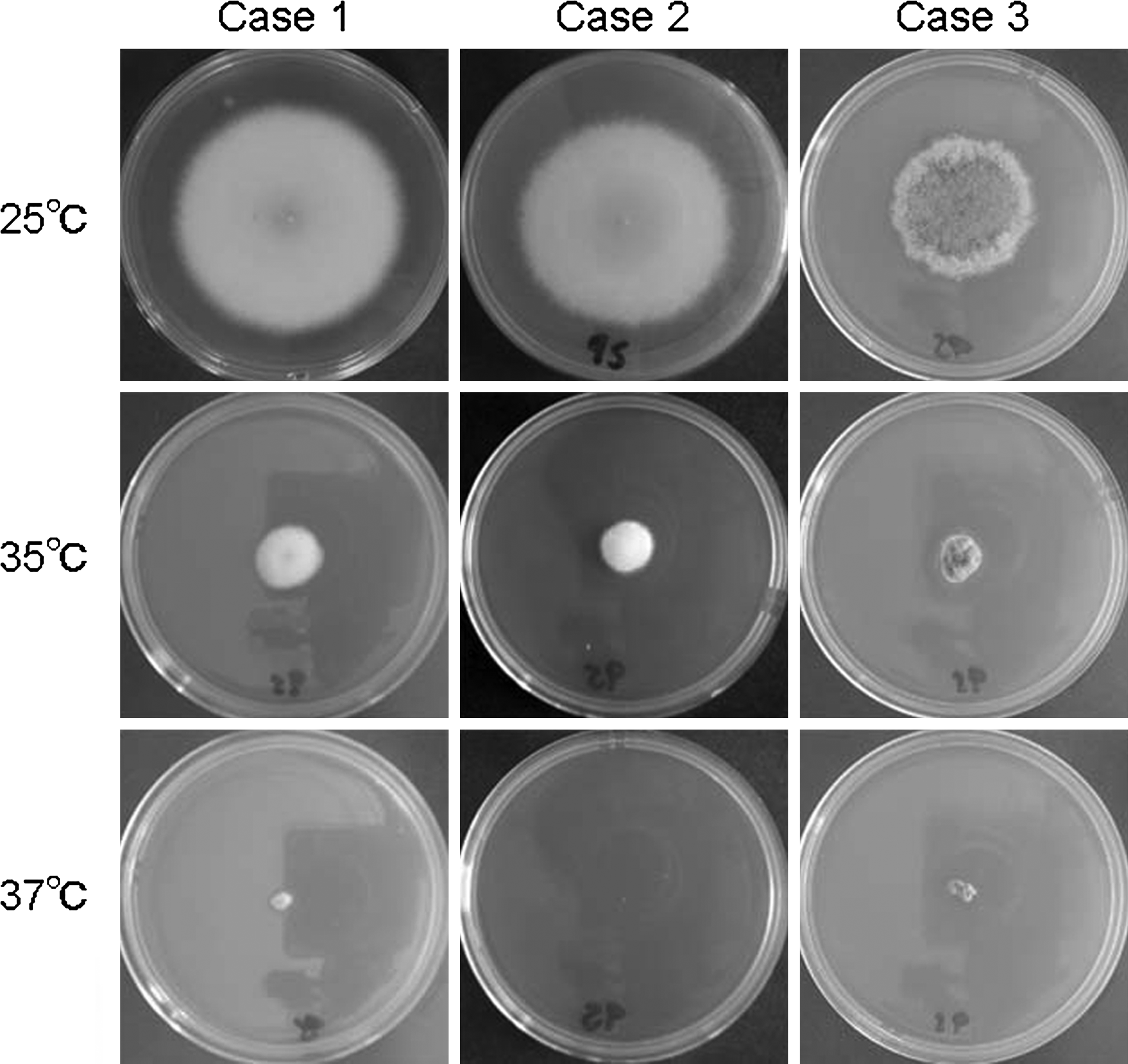
Fungal colonies grown on Sabouraud dextrose agar at different temperatures. All 3 isolates grew well and formed large brownish-black pigmented colonies at 25°C. All 3 isolates had smaller colonies on 35°C. For 37°C, the colonies of cases 1 and 3 were even smaller, and nothing grew on the plate for case 2.
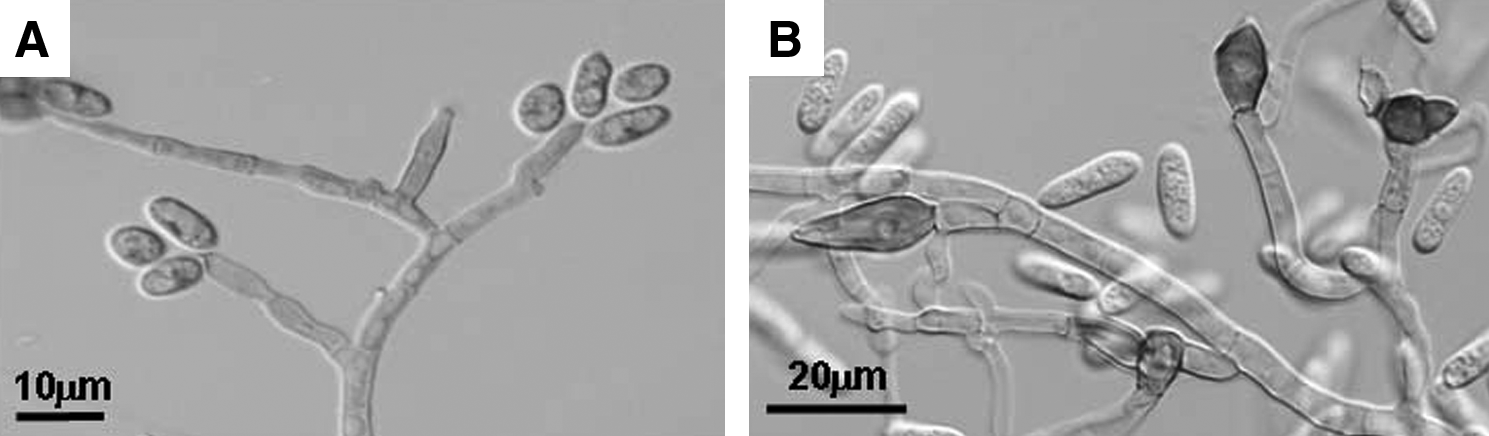
Microscopic examination of the culture media of case 2 reveals cylindrical conidia with hyphae
The MICs of different antifungal drugs are listed in Table 2. All of the isolated strains had very similar drug-sensitive profiles, and all were sensitive to amphotericin B, itraconazole, miconazole, micafungin, and voriconazole. They were relatively resistant to flucytosine, fluconazole, and natamycin.
MIC (μg/mL) AMPH, amphotericin B; 5-FC, flucytosine; FLCZ, fluconazole; ITZ, itraconazole; MCFG, micafungin; NTM, natamycin.
All 3 isolates were also grown on Sabouraud dextrose agar at 25°C, 35°C, and 37°C (Fig. 3). All 3 isolates grew well and formed large brownish-black pigmented colonies at 25°C, and all 3 isolates had smaller colonies at 35°C. At 37°C, the colonies of cases 1 and 3 were even smaller, and nothing grew on the plate for case 2.
Discussion
We have presented the clinical characteristics of 3 patients with keratitis caused by C. gloeosporioides, a coelomycetous fungus. We also presented the temperature and drug sensitivities of the isolated strains. The consistency of clinical and in vitro findings may reflect the clinical feature of C. gloeosporioides keratitis. A review of the literature showed that C. gloeosporioides is the second most common species of Colletotrichum keratitis after Colletotrichum dematium. The C. dematium has been reported in cases from India and Florida, and C. gloeosporioides keratitis has been reported from Florida and Japan including our 3 cases.4–8,10–13 Fernandez et al. and Kaliamurthy et al. reported that the principal risk factor for Colletotrichum keratitis was ocular trauma.4,5 Colletotrichum spp. are usually pathogenic to plants causing anthracnosis, necrosis, leaf spots, and fruit rot, and all our 3 patients were injured during farm work. Thus, the principal risk factor for Colletotrichum keratitis including C. gloeosporioides would be ocular trauma and contamination by organic materials.
In our antifungal susceptibility tests, all 3 strains had similar antifungal sensitivity profiles. Although there has not been an investigation of the antifungal susceptibility against Colletotrichum spp. isolated from keratitis, 2 studies have reported antifungal susceptibility against Colletotrichum spp. isolated from hyalohyphomycosis, a cutaneous disease.10,16 O'Quinn et al. tested 1 strain of C. gloleosporioides and 2 strains of Colletotrichum coccodes, and Guarro et al. tested 1 strain of C. gloleosporioides, 1 strain of C. coccodes, and 1 strain of C. dematium.10,16 All of the tested strains were resistant to 5-flucytocine and fuluconazole, but susceptible to amphotericin B, itraconazole, miconazole, and ketoconazole. These results are similar to our results indicating that the drug-sensitivity profiles are probably characteristics of Colletotrichum spp.
One concern in the selection of an antifungal medication is that most of the cases of Colletotrichum keratitis were treated with natamycin with or without other antifungal agents. This selection may be because of the ready availability of natamycin in the ophthalmology clinic.
There have been a few reports mentioning the drug sensitivity test against natamycin because of the unavailability of a test kit. Fernandez et al. tested the sensitivity of 5 strains of Colletotrichum spp. to natamycin, and found that 3 were resistant and the other 2 had intermediate resistance. 4 One of the 5 strains was C. gloeosporioides and had intermediate resistance. 4 We also tested the drug sensitivity test against natamycin, and found that all 3 strains had intermediate resistance. These results may explain the clinical course reported, because most of the Colletotrichum keratitis cases were treated by natamycin and some cases were healed and some cases did not respond to natamycin. We treated our 3 cases with natamycin combined with voriconazole, or combined with miconazole in 1 case, and both had prompt resolution. Thus, the clinical course and drug sensitivity results suggest that a combination of natamycin with other antifungal drugs might be an effective therapy against C. gloeosporioides keratitis. We treated all our cases with voriconazole, because voriconazole is a new, broad-spectrum antifungal drug, and excellent results have been reported after voriconazole treatment in cases of fungal keratitis and endophthalmitis caused by a number of species of fungi.17–19
An interesting finding in our study was that the sites of infection in all 3 cases were located in the anterior corneal stroma, although the appearance of infiltrates showed typical filamentous fungal keratitis. Although hypopyon was seen in 1 case, the hypopyon disappeared a few days after the initiation of antifungal therapy, thus indicating that the hypopyon was most likely an inflammatory response to the infection. These findings may be related to the temperature sensitivity of the C. gloeosporioides; all 3 strains grew well at 25°C but did not grow well at 35°C, and smaller or no colonies were found at 37°C. The temperature of the anterior chamber is usually 35°C or higher, and that of the corneal surface is 35°C or lower depending on the ambient temperature.20,21 Thus, it could be hypothesized that the strains which cannot grow at temperatures of 35°C or higher may not be able to infiltrate deep into the corneal stroma and are, thus, located in the anterior stroma. This temperature sensitivity might be another reason that C. gloeosporioides are rare pathogens in humans, and that C. gloeosporioides infection in humans is limited to the body surface such as the cornea and skin. Further experiments on animals may be helpful in testing this hypothesis.
In conclusion, we report the characteristics of 3 cases of C. gloeosporioides keratitis. The lesion of all 3 cases was located in the anterior stroma, and it was resolved in a few weeks treated with natamycin combined with voriconazole and miconazole. The similar drug-sensitivity profiles of C. gloeosporioides could be helpful for the treatment of C. gloeosporioides keratitis.
Footnotes
Acknowledgments
The authors would like to acknowledge Professor Kazuko Nishimura of Department of Fungal Infections: Research Center for Pathogenic Fungi and Microbial Toxicoses, Chiba University, for her definite microbiological suggestions.
Author Disclosure Statement
The authors indicate no financial support or financial conflicts of interest.