
Abstract
Abstract
Purpose:
To evaluate postoperative outcome and recurrence rate after primary pterygium excision using preoperative Mitomycin C (MMC) injection versus limbal conjunctival autograft transplantation (LCAT).
Methods:
Ninety-one eyes with primary pterygium were divided into 2 groups. Group A eyes (included 48 eyes) were operated upon with pterygium excision 1 month after subpterygial injection of MMC 0.015%. Group B eyes (included 43 eyes) were operated upon with pterygium excision followed by LCAT technique. Pterygium regrowth over the cornea for 1 mm or more was considered as a recurrence.
Results:
The follow-up period was 24 months. In group A, reported recurrence was found in 2 (4.2%) eyes with a complication rate of 16.80%. While in group B, recurrence was reported in 4 (9.3%) eyes with a complication rate of 11.63%. No serious postoperative complications were reported. There was no statistically significant difference between the 2 groups regarding the recurrence rate as well as the complication rate.
Conclusion:
Both techniques used in the current study proved to be effective in reducing the recurrence rate after excision of primary nasal pterygium with minimal postoperative complications. Preoperative MMC injection was technically easier, with shorter operative and preservation of healthy conjunctiva. However, LCAT is a one-stage procedure and independent from adjunctive pharmacological or radiation therapies with their hazards.
Introduction
Several techniques have evolved in a trial to overcome the high rate of postoperative recurrence. However, none proved to be totally effective. Among these modalities are postoperative B-irradiation, 2 conjunctival autografting, 3 intraoperative4,5 or postoperative adjuvant mitomycin C (MMC),6,7 and amniotic membrane transplantation (AMT). 8
We represent our experience for control of postoperative pterygium recurrence by using 2 different techniques on 2 groups of patients with primary nasal pterygia. Then we compare the postoperative outcome in both groups.
Methods
This was a prospective randomized study conducted on 91 eyes of 91 patients with primary nasal pterygium who attended the health service in Menoufia University Hospitals in Shebin El Kom and Manshiet Soltan during the period from October 2005 to October 2008.
The patients were randomly enrolled into 2 groups. The first group had underwent bare scleral excision of the primary nasal pterygium 1 month after subconjunctival injection of 0.1 mL of 0.15 mg/mL MMC into the body of the pterygium. The second group had undergone limbal conjunctival autograft transplantation (LCAT) after pterygium excision. All surgeries were performed by one surgeon (Hassan G. Farahat).
All patients of the study had a primary nasal pterygium encroached on the surface of the cornea with no other ocular pathology. A comprehensive ophthalmic examination, including best-corrected visual acuity testing, slit-lamp examination, Goldmann applanation tonometry, fundus examination, and examination of ocular motility, was carried out for all patients. Consents were taken from all patients and research was approved by the institutional review board. All measures were in accordance with the tenets of the Declaration of Helsinki.
Surgical technique
Group (A)
Preparation of MMC: Mutamycin (Bristol-Myers-Squibb) vial containing 5 mg powder of mitomycin was reconstituted with 33 mL sterile water to get a concentration of 0.15 mg/mL for injection.
Technique of MMC injection: Topical anesthesia (Benoxinate hydrochloride 0.4%) was first applied in the involved eye followed with subconjunctival injection of 0.1 mL of 0.15 mg/mL MMC into the pterygium at the limbus using 27-gauge needle on insulin syringe. Cotton-tipped applicator was applied to the site of injection upon withdrawal of the needle to prevent reflux of the injected drug. Thorough rinsing of the ocular surface with saline was performed to remove any residuals of MMC.
After injection, the patient received topical-combined antibiotic-steroid eye drops 4 times daily and dexamethasone 0.1% ointment at bedtime for 1 week. The patient was seen at 1 day, 1 week, and 1 month after subconjunctival injection of MMC. A complete ophthalmic examination was performed each visit. One month after the injection, the patient underwent bare scleral excision of the pterygium.
Bare scleral excision of the pterygium: Topical anesthesia was instilled followed by placement of self-retaining eyelid speculum. Subconjunctival Lidocaine 2% with epinephrine 1:100,000 was injected beneath the body of the pterygium using 27-gauge needle.
A Bard Barker knife No. 15 or crescent knife was used to dissect the head of pterygium starting 0.5 mm temporal to the advancing edge till the limbus. A blunt Wesscot scissors was used to undermine the planned conjunctival resection and to dissect the pterygium 5 mm from the limbus leaving the peripheral base to avoid medial rectus tendon damage. Excision of the pterygium did not extend to or involve the plica semilunaris. When there was a large bare sclera, the conjunctiva was sutured to the episcleral 3 mm from the limbus using interrupted 8/0 vicryl suture.
Group (B)
Topical anesthesia followed by peribulbar anesthesia (Lidocaine 2% with epinephrine 1:100,000) was used in all cases of LCAT. After opening of the palpebral fissure with lid speculum, superior and inferior episcleral stay sutures (using silk 7/0) 2 mm from the limbus were used to secure the globe and to help rotating the globe temporally for proper surgical exposure and nasally for dissection of the autograft.
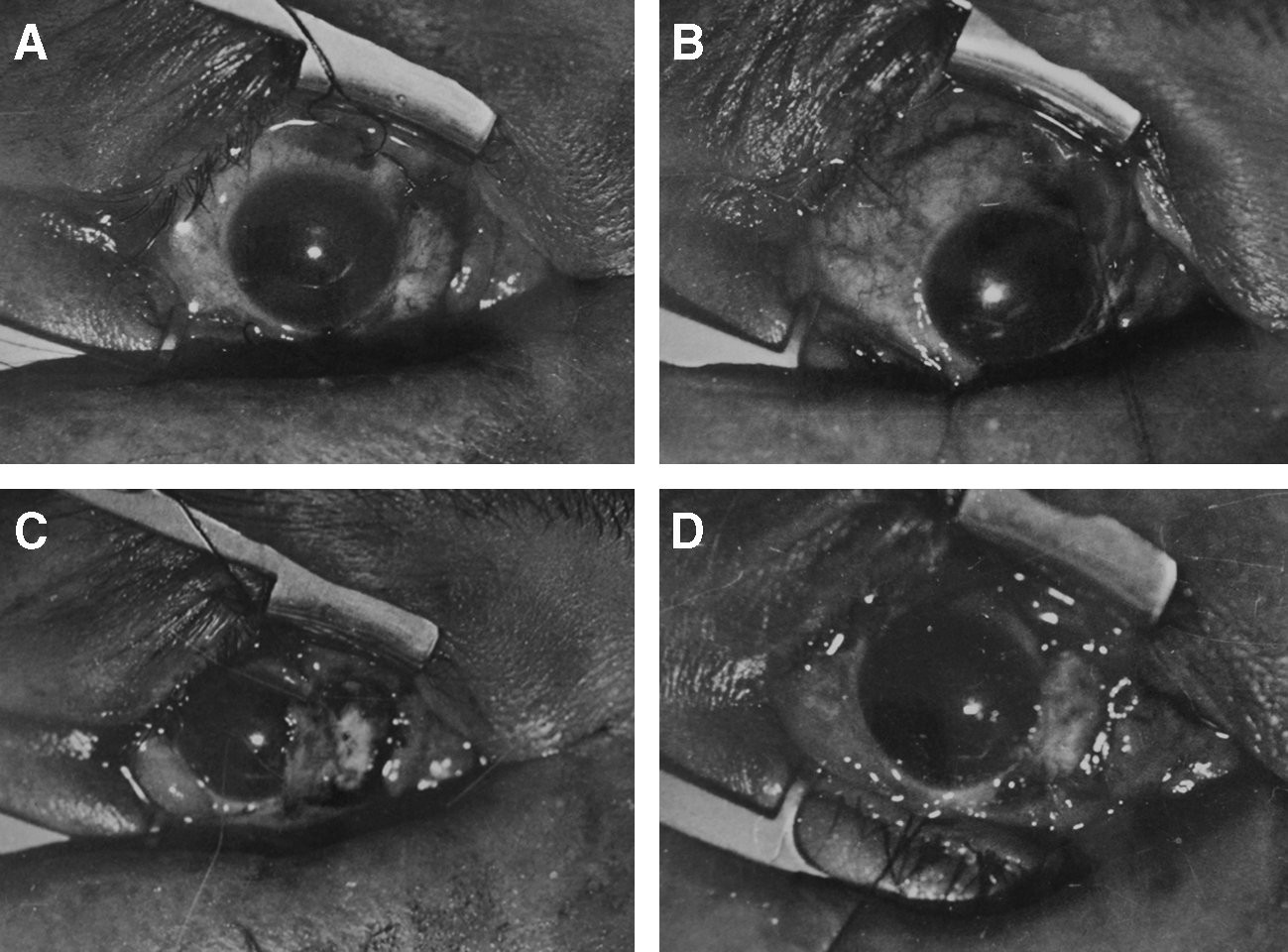
Pterygium limits were measured and marked. A Bard Barker knife No. 15 or crescent knife was used to dissect the head of pterygium starting 0.5 mm temporal to the advancing edge till the limbus. A blunt Wesscot scissors was used to undermine the planned conjunctival resection and to dissect the pterygium 5 mm from the limbus leaving the peripheral base to avoid medial rectus tendon damage (Fig. 1.A).
Limbal conjunctival autograft transplantation;
The bed of the excised pterygium was measured with a calliper. The conjunctivo-limbal graft was taken from the upper temporal bulbar conjunctiva of the same eye and was 0.5 mm larger than the measured pterygium bed; the dimensions of the graft were outlined by surgical marker pen (Fig 1.B). The conjunctiva was ballooned with 2% lidocaine with 1:100,000 epinephrine. The conjunctiva was dissected by a blunt Wesscot scissors from the fornix side toward the limbus so that the marks made by the pen were included in the graft.
A Bard Barker knife No. 15 or a crescent knife was used to extend the dissection of the graft across the limbus and was extended to include 0.5 mm of the peripheral clear cornea. Before the graft was separated, 10/0 monofilament nylon sutures were inserted in the limbal corners of the graft and 8/0 vicryl sutures were inserted in the conjunctival corners of the graft. The graft was transferred to the resected pterygium bed taking care to put the epithelial surface of the graft superficially and the corneal edge toward the cornea (Fig 1.C). It is then secured in place by interrupted 10/0 nylon sutures to the cornea and interrupted 8/0 vicryl to the conjunctiva (Fig. 1D).
The postoperative care included the administration of topical antibiotic eye drops 4 times daily and dexamethasone 0.1% ointment at bedtime until all signs of inflammation disappeared with an average of 4 weeks. An eye pad was applied till complete reepithelialization. Sutures were removed after healing of the wound or if they became loose.
In both groups, patients were examined 1 day postoperative and then after 1 week for evaluation of the healing process and detection of early (Fig. 2) postoperative complications. Patients were reexamined at 1, 3, 6, 9, and 12 months postoperatively, then every 6 months in the next year (Fig. 3). During each visit complete ophthalmic examination was done. It was judged that the lesion has recurred if there was fibrovascular growth over the cornea for 1 mm or more.
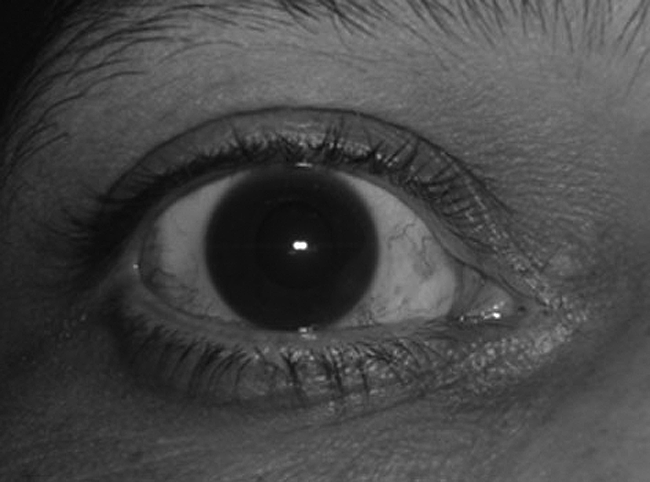
Postoperative photo of group A eye 1 month after excision of the pterygium.
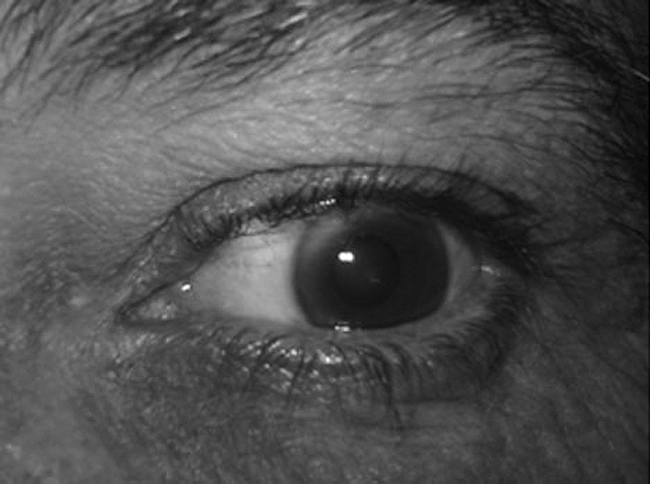
Postoperative photo of group A eye 24 months after excision of the pterygium.
Statistical analysis was carried out with SPSS version 15 (SPSS Science, Chicago, IL) using chi-square and student t-test with a level of significance at 95%.
Results
Ninety-one eyes of 91 patients were enrolled in the study, including 48 eyes in group A and 43 eyes in group B. There were 24 (50%) men and 24 (50%) women in groups A and 22 (51.16%) men and 21 (48.84%) women in group B. The patient age ranged from 25 to 65 years in group A and from 22 to 60 years in group B.
The mean of extension of pterygia onto the cornea was 3.04±1.08 mm in group A and 3.44±1.21 mm in group B. The mean width of the pterygium on the limbus was 4.46±1.44 mm in group A and 5.06±1.39 in group B.
The pterygia were less vascular and less inflamed at 1 month follow-up visit at the time of pterygium excision in group A eyes.
Follow-up period in group A ranged from 24 to 38 months with a mean of 29.5±4.3 months. In group B it ranged from 24 to 42 months with a mean of 30.3±4.1 months.
The visual acuity in group A was improved 1–2 lines in 18 eyes (37.5%), while in group B the improvement in visual acuity was recorded in 11 eyes (25.58%) for 1–3 lines. Other cases in both groups showed no improvement.
In group A, reported recurrence was found in 2 (4.2%) eyes. The time interval from the surgery to the recurrence was 5 months in one case and 6 months in the other one. While in group B, recurrence was reported in 4 (9.3%) eyes. The time interval from the surgery to the recurrence was 4.5±1.6 months. There was no statistically significant difference between the 2 groups regarding the recurrence rate (P=0.536) (Table 1).
Regarding the postoperative complications, in group A, there was subconjunctival hemorrhage in 6 cases (12.6%). Conjunctival vascularization was reported in 2 cases (4.2%) but it was away from the limbus and was not considered a recurrence. No patients developed a persistent epithelial defect, dellen, or signs of scleral melting at anytime during the postoperative follow-up. In group B, there was hematoma under the graft in 3 cases (6.98%) and Tenon's granuloma in 2 cases (4.65%). The hematomas were drained through 1 mm incision in the graft in the first postoperative day. The granulomas were excised 2 weeks postoperatively. No serious postoperative complications were reported. There was no statistically significant difference between the 2 groups regarding the complication rate (P=0.386) (Table 1).
Discussion
Due to the high recurrence rates of 30–80% after pterygium excision using the bare sclera technique, a variety of other treatment modalities have been proposed. 9 Adjunctive treatment after bare sclera excision with MMC is effective in reducing its recurrence rate (0.5–16%). 10 MMC acts as an alkylating agent and potent fibroblast inhibitor, which can cause irreversible damage to the cell. Besides, it also inhibits migration of fibroblast and synthesis of collagen and therefore affects wound healing. MMC used to be applied either intraoperatively or postoperatively.4,6,7
Applying MMC at the time of surgery provides an advantage of directly applying the drug to the bed of the pterygium.4,5 However, the direct contact of MMC with corneal and conjunctival endothelium caused persistent corneal or conjunctival defects. As well, MMC which comes in direct contact with the cornea has a negative effect on corneal endothelium. The same adverse events have been seen in postoperative MMC application in the form of eye drops. Moreover, the surgeon has to rely on the patient to correctly self-administer a toxic chemotherapeutic agent at home.7,9
Preoperative injection of low-dose MMC was suggested by Donnenfeld et al. 11 who recorded 6% recurrence rate in their series. They injected 0.015% (0.15 mg/mL) MMC subconjunctivally 1 month before bare sclera pterygium excision in 36 patients with a follow-up of 24 months. We adopted this technique in the first group of our series with a recurrence rate of 4.2% over a follow-up period of 24 months.
Preoperative MMC injection has an advantage of more precise titration of the drug and its direct delivery to the site of the pathology with no contact with the corneal surface. The drug is applied directly to the activated fibroblasts in the subconjunctival space, where it can work directly on the cells responsible for pterygium recurrence without damaging the surface epithelium stem cells, which play no role in pterygia formation or recurrence. This may diminish long-term healing difficulties associated with MMC. 11 Another advantage of preoperative MMC injection is that it is technically easy with short operative time. 12
In the current study, histopathological evaluation of 30 specimens of pretreated pterygia with subconjunctival injection of MMC 1 month before excision revealed normal conjunctival epithelium in most cases (Fig. 4). The conjunctival epithelium was thin in 4 cases and multiple foci of goblet cells were found in 6 cases. These findings clarify the safe effect of injection of 0.1 mL of 0.15 mg/mL MMC 1 month before excision of pterygium on the conjunctival epithelium and they coincide with the results obtained by Donnenfeld et al. 11 and Chang et al. 13
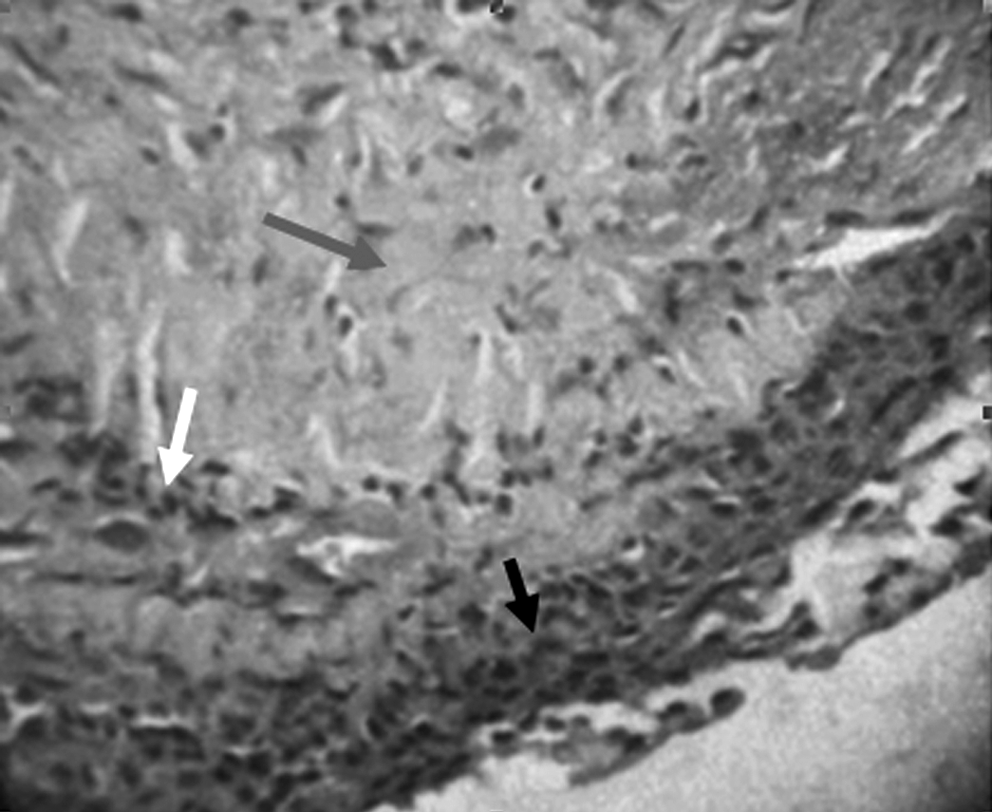
Light microscopic section of pterygium 1 month after subconjunctival injection of mitomycin C shows intact epithelium (black arrow). Subepithelial tissue shows dense fibrosis (grey arrow), scattered chronic inflammatory cells (white arrow), and congested blood vessels.
Clinical and laboratory evidence indicates that corneal stem cells are located at the limbus. 14 Localized corneal stem cell dysfunction with loss of limbal barrier against conjunctival invasion has been proposed as a pathogenic factor in pterygium growth and recurrence. The discovery of the role of limbal stem cells in the maintenance and stability of the corneal surface has rationalized the use of limbal conjunctival autograft transplantation LCAT. 15
LCAT has been used successfully to correct limbal dysfunction, acting as a barrier against conjunctival invasion of the cornea using the principle of contact inhibition. It was first performed by Kenyon et al. 16 who reported a recurrence rate of 7.9% in patients with primary pterygia. Since then, less impressive results were revealed with a recurrence rate ranging from 16% to 25.9%.3,17
This technique was adopted in the second group of current series. The recurrence rate reported in was 9.3% which is lower than that recorded in cases done with conjunctival autograft only. This low rate is comparable to that of the first group in the current study as well as the results recorded in other series using different techniques such as conjunctival autografting, AMT, and adjuvant antimetabolite application. However, it is a technically difficult and time-consuming procedure. Moreover, it sacrificed part of the healthy conjunctiva and initiated fibrous tissue formation at the site of donor graft. This may affect the outcome of surgical procedures that require healthy conjunctiva if needed in the future for those patients.
We concluded that both techniques used in the current study proved to be effective in reducing the recurrence rate after excision of primary nasal pterygium with minimal complications in the short- and intermediate-term postoperatively. Preoperative MMC injection was technically easier, provided short operative time compared with LCAT, and preserved healthy conjunctiva. However, LCAT is a one-stage procedure in contrast to the preoperative MMC injection which requires the patient to come first for the injection, and then he has to wait for 1 month before excision of the pterygium. As well, LCAT has the advantage of independence from adjunctive pharmacological or radiation therapies.
Footnotes
Author Disclosure Statement
No competing financial interests exist.