
Abstract
Abstract
Purpose:
The purpose of this article was to evaluate the long-term efficacy of a low-concentration (LC) atropine eye drop regimen (0.05%–0.1%) for controlling myopia progression in schoolchildren.
Methods:
This retrospective, case–control study enrolled myopic schoolchildren who had been followed-up for at least 3 years from 1999 to 2007. Children who received LC doses of atropine eye drops [initial prescription 0.05%, if progression over −0.5 diopter (D) during a 6-month follow-up then changed to 0.1% atropine] every night at bedtime were included in the LC atropine group, and untreated children served as controls.
Results:
A total of 117 children were included in this study. The mean age was 8.4 years. There were 97 children in the LC atropine group and 20 children in the control group. The mean follow-up duration was 4.5 years. In a mixed model analysis, the adjusted myopia progression in the LC atropine group was −0.23 D/year, significantly lower than that of the control group, which was −0.86 D/year (P<0.001). About 80% of the treatment group had slow myopia progression (less than −0.5 D progression per year). In a multivariate analysis, factors such as initial spherical refraction with less myopia and treatment with LC atropine were significantly associated with less myopia progression, but age, sex, and initial astigmatism were not significantly associated (P<0.001, P<0.001, P=0.442, 0.494, and 0.547, respectively).
Conclusion:
The results of this study demonstrate that long-term and regular instillation of LC atropine eye drops is effective for controlling myopia progression and provides a possible strategy for an initial myopia regimen.
Introduction
Recently, high myopia has become a leading cause of untreatable visual loss in East Asia.8–10 Myopia is a refraction error that requires optical correction. High myopia especially is highly associated with sight-threatening conditions. High myopia, defined as refraction greater than −6 D, is a significant public health problem because of its association with increased risk of several ocular diseases including cataract, glaucoma, retinal detachment, myopic retinal degeneration, visual impairment, and blindness.11–13 Studies have shown that myopia progresses faster in children with myopia at a younger age.14,15 Once myopia occurs in schoolchildren, it quickly progresses until early adulthood when it slows down.16–18 Early onset of myopia in childhood is associated with high myopia in adult life.19–21 Therefore, it is very important to stop or control myopia progression in myopic children from a young age.
Myopia progression in children is difficult to control. Recently, orthokeratology seems to have some effect on controlling myopia progression. 22 However, because of fear of corneal infection and the high cost, it is not widely used. Pirezepine eye ointment has been shown to have a moderate effect on preventing myopia progression, but effects of its long-term use and efficacy still need to be investigated.23,24
Atropine, a nonselective muscarinic antagonist, is the most widely studied pharmacological agent for the prevention of myopia progression in children. To date, atropine is the only known effective drug to retard myopia progression, and high concentrations (1% or 0.5%) of atropine eye drops are the most effective in controlling myopic progression in children.25–27 However, mydriasis and photophobia symptoms induced by high concentrations of atropine often disturb patients. Photophobia, blurred near-vision, and fear of long-term ocular or systemic side-effects resulted in a high rate of noncompliance from patients. 5 We previously reported the effectiveness of topical low-concentration (LC) (0.05%) atropine in controlling myopia progression in myopic schoolchildren. 28 This low-concentration might have fewer side effects and provide a greater balance between efficacy and compliance. In this study, we investigated the effectiveness of a long-term regimen of LC (0.05% to 0.1%) atropine eye drops for controlling myopia progression in myopic children.
Methods
A retrospective chart review was conducted of children with myopia who had visited Chang Gung Memorial Hospital, Kaohsiung Medical Center, Taiwan, between 1999 and 2007. Myopia was defined as spherical equivalence of refractive status (SER, spherical refraction plus half of cylinder refraction) greater than −0.5 D. Children aged from 6 to 12 years who had regular follow-ups for at least 3 years were included. Exclusion criteria included astigmatism (cylinder refraction) greater than 2 D, other combined ocular disease, such as amblyopia, strabismus, congenital cataract, glaucoma, corneal scar, optic neuropathy, traumatic ocular injury, uveitis, and ocular tumor, history of any ocular surgery, and any systemic diseases or condition that may affect visual function and development, such as diabetes mellitus and chromosome anomaly.
One hundred 17 myopic schoolchildren met the above criteria and were included in the study. In the LC atropine treatment group, an LC atropine eye drop was prescribed for retarding myopia progression. The protocol of this LC atropine regimen was an initial prescription of 1 drop of 0.05% atropine at bedtime every night. If myopia progression was greater than −0.5 D at a 6 month follow-up, then the concentration was increased to 0.1% atropine. The control group included 20 myopic children who did not receive any treatment during the follow-up period.
Initial ocular investigations included slit lamp biomicroscopic examination for anterior segment, direct or indirect ophthalmoscopic examination for vitreous, retina and optic disc evaluation, and cycloplegic refraction. The spherical equivalent of refractive status was obtained by autorefractor (KR-7000/8100; Topcon; Tokyo, Japan) at 30 min after a cycloplegic procedure with initial 1% cyclopentolate, followed by 2 successive instillations of 1% tropicamide with a 10-min interval. Cycloplegic visual acuity with correction was measured using a Landolt's C chart for confirmation. The LC (0.05% or 0.1%) atropine solution was prepared by diluting 0.5% or 0.1% atropine ophthalmic solution (Atropine Sulphate Eye Drops; Wu-Fu Lab. Co.; Ilan, Taiwan) with sterile distilled water.
The records of refractive status obtained by the initial survey method were collected for analysis from the beginning of therapy to the last follow-up at the end of 2009. The progression of myopia per year (mean myopia progression rate) was calculated as changes of spherical equivalent of refractive status (diopters) divided by follow-up period (months) and then multiplied by 12. Four grades of myopia progression rate were defined as between 0 and less than −0.25 D/year (slowest), between −0.25 and less than −0.5 D (moderate), between −0.5 D and less than −1 D (faster), and −1 D or greater (fastest). A “threshold” of myopia shift −0.50 D/year for slow and fast progression was chosen as a target point for comparison between groups according to the reported result of 2% pirenzepine gel on myopia control. 16
Statistical analysis
Because of the high correlation of SER between the right eye and left eye of subjects (r=0.941), only the SER of right eye was used for further statistical analysis. For continuous variables such as age, the duration of follow-up, and spherical equivalent refraction, the Student's t-test was used to determine the statistical significance of the between-group differences. We used a longitudinal mixed-model analysis to test for associations between LCs of atropine treatment and the rate of myopia progression, a technique that permits full use of available data while controlling for internal correlations and other covariates. This approach treats each refraction measurement from each subject as a separate observation and adjusts for the variable follow-up time difference within subject correlations and the correlation with the prior refraction measurement. Subjects were treated as random effects so the analysis could be adjusted to each individual's own refraction. A first-order autoregressive error structure accounted for within-subject correlation. The adjusted covariates in the mixed model also include time from baseline, age, gender, initial SER, initial astigmatism, and initial spherical refraction for analysis.
The chi-square test was used to compare the categorical variables such as the portion of patients with more than −0.5 D myopia progression per year in each group. The Statistical Package for the Social Sciences software (SPSS version 14, Chicago, IL) was used for analysis.
Results
There were 97 myopic children in the LC atropine group (treatment group) and 20 myopic children in the control group (Table 1). The male:female ratios were 54:43 in the treatment groups and 11:9 in control. The mean ages at the beginning of study were 8.47±1.82 years (range: 6–12) in the treatment group and 8.25±1.88 years (range: 6–12) in the control group. The mean follow-up intervals were 4.54±1.40 (range: 3.0–8.0) and 4.11±1.21 (range: 3.0–7.0) years in the treatment and control groups, respectively. The initial SER were −2.45±1.63 D (ranging from −0.50 to −7.25) in the treatment group and −1.87±0.94 D (ranging from −0.50 to −4.13) in the control group. There were no significant differences observed when comparing gender, age, initial SER, and follow-up period between the 2 groups (P=0.591, 0.956, 0.328, and 0.253 respectively).
Statistically significant (P<0.05).
LC atropine, low-concentration atropine; N, number; M/F, male/female; SER, spherical equivalent refraction; D, diopter.
After the interval of follow-up, the final SER were −3.38±1.77 D (range from −0.375 to −9.25) in the treatment group and −4.94±1.15 D (range from −3.375 to −8.00) in the control group. The mean myopia progression per year (mean myopia progression rate) in the treatment group was significantly lower than the control group (−0.31±0.26 D vs. −0.90±0.30 D; P<0.001, Table 2). In the mixed model analysis, the unadjusted myopia progression rate in the treatment group was also significantly lower than the control group (−0.23 D vs. −0.86 D; P<0.001; Fig. 1). After adjusting covariates of age, sex, initial spherical refraction, and initial astigmatism, the myopia progression rate in the treatment group (−0.23 D, 95% CI=−0.27 to −0.20, P<0.001) was still significantly lower than the control group (−0.86 D, 95% CI=−0.93 to −0.78, P<0.001, Table 3). The estimated difference between the 2 progression rates is 0.62 D (95% CI=0.54–0.71, P<0.001). In addition, initial spherical refraction was significantly associated with the myopia progression rate (Table 3). Children with a less severity of initial myopic spherical refraction had less myopia progression rate. Age, sex, and initial astigmatism were not statistically significantly (P=0.442, 0.494, and 0.547, respectively) associated with progression rates.
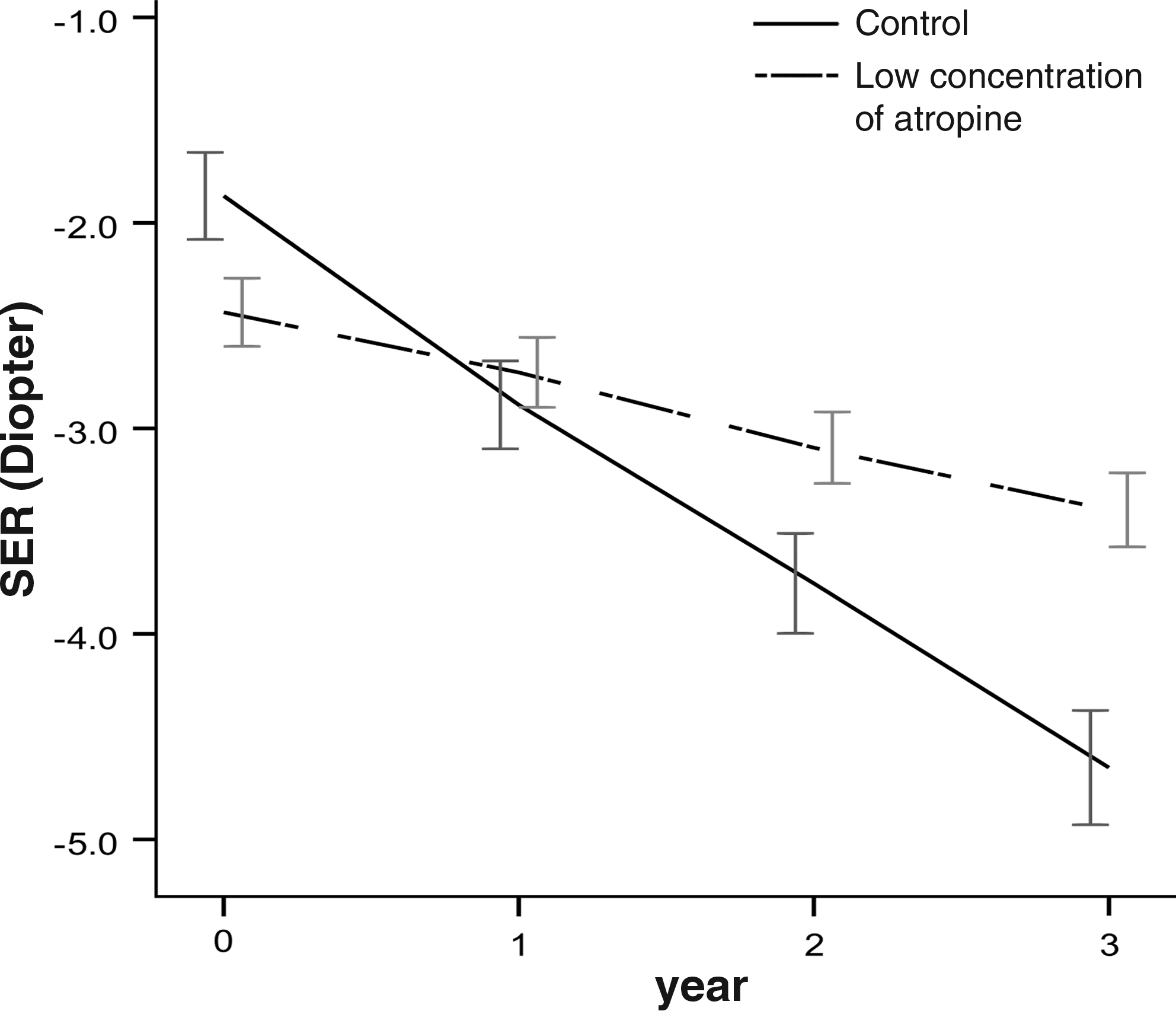
The initial and final spherical equivalent refraction and myopia progression with time in the low-concentration atropine group and the control group. Error bars: ±1 standard error. SER, spherical equivalence of refractive status.
Statistically significant (P<0.05).
SD, standard deviation; CI, confidence interval.
Estimate of difference between the two progression rates is 0.62 (95% CI=0.54–0.71, P<0.001).
Fast myopia progression is defined as myopia progression greater than −0.5 D per year. Nineteen of 97 (20%) of the children in the treatment group and all 20 (100%) children in the control group had fast myopia progression (P<0.001; Table 4). Two of 97 (2%) in the treatment group had fastest myopia progression in comparison to 6 of 20 (30%) in the control group. Seventeen of 97 (18%) in the treatment group had faster myopia progression in comparison to 14 of 20 (70%) in the control group. About 80% of the children in the treatment group had slow myopia progression in comparison to 0% in the control group. Thirty of 97 (31%) and 48 of 97 (49%) in the treatment group had moderate and slowest myopia progression in comparison to 0 of 20 (0%) for both in the control group.

Chi-square test for trend in four grades between two groups, P<0.001.
Chi-square test for slow and fast progression rate between two groups, P<0.001.
In the course of our study, 44 of 97 (45%) children in the LC treatment group changed the atropine treatment concentration from 0.05% to 0.1% because of myopia progression over −0.5 D during a 6-month period. There were no side effects of cataract formation and retinopathy noted in these children during any follow-up period.
Discussion
The prevention of myopia progression is of critical importance to reduce the threat of visual complications associated with high myopia in later life. Therefore, delaying the onset of myopia and intervention to stop or retard the myopia progression from childhood to adolescence are important issues. In this study, it was shown that long-term use of LC atropine helps to retard myopia progression in children. In addition, this study supports previous work showing that children with a less severity of initial spherical refraction (SR) have significantly less myopia progression than children with a greater severity of initial myopia refraction.14,19,29
To date, atropine eye drops are still the only treatment demonstrated to have a consistent effect on the retardation of myopia progression.25,30 Although there are multiple reports about the effect of atropine in the treatment of myopia progression (Table 5),5,27,28,31–35 most of the reports are short-term studies (1 to 2 years) that use high concentrations of atropine (1% or 0.5%). Because of the side effect of photophobia and fear of systemic effect, long-term high concentration regimens of atropine have led to a high drop-out rate due to poor compliance (16% to 58%), which may be a causative factor in the high rates of patients with high myopia later in life.32,34 The difficulty in getting patients to comply with high concentration treatment regimens over the long term may be lessened by a lower concentration regimen that results in less severe side-effects. Even though LC atropine is not as effective as a high concentration in the arrest of myopia progression, it still significantly retards myopia progression in comparison to no treatment (−0.23 D vs. −0.86 D per year). In addition, 80% of patients responded well with slow myopia progression from LC atropine in comparison to 0% with no treatment. Therefore, LC atropine might be an initial choice for long-term therapy to balance the compliance and therapeutic effect.
In this study, 45% of patients treated with 0.05% atropine had myopia progression greater than −0.5 D during 6-month therapy and were shifted to 0.1% atropine treatment. With LC atropine treatments (0.05% or 0.1%), 80% of patients achieved slow myopia progression and 20% had fast progression. It is well recognized that patients have varied responses to drugs, both beneficial and adverse. There are many factors such as genetic factors, environmental exposures, severity of disease, and so on,36–41 which might help explain heterogeneity in drug responses. Recently, pharmacogenetics and personalized medicine have garnered more attention in clinical and research fields because of their effectiveness on an individual basis.42–44 We propose that different individuals might have different responses to atropine and some patients would have good myopia control by using LC atropine eye drops rather than high concentration. The development of personalized medicine for atropine treatment with myopia, though currently nonexistent, is important and promising as it will balance side effects and efficacy. Even though, currently, pharmacogenetic tests and pharmacogenetic-guided dosing are still unavailable, using LC atropine (0.05%) initially and routine follow-up for myopia progression would be considered as an alternative for therapeutic screen. After 6 months of monitoring myopia progression, changing to a higher concentration is reasonable for the patients with fast myopia progression. This strategy for the myopia regimen, from low to high concentration, might provide some kind of personalized medicine.
Treatment with high-concentration atropine eye drops can produce some unwanted adverse effects, such as photophobia due to mydriasis and blurring of near vision from induced cycloplegia. For example, Yen et al. reported that 100% of participants receiving 1% atropine had photophobia. 34 LC atropine (0.05% and 0.1%) will induce mild to moderate mydriasis in comparison to full mydriasis induced by 1% atropine. The pupil sizes of mydriasis induced by LC (0.05% and 0.1%) atropine are around 3.2 and 5.5 mm (data not published). LC atropine might also induce less photophobia, making it more suitable for long-term use to retard myopia progression. However, we still suggest patients use photochromatic and anti-ultraviolet light–coated lenses to minimize the photophobia symptom and protect the retina. For the accommodation inhibition, it is reported that using 1% of atropine resulted in the accommodation amplitude decreasing from 13.76 to 2.81 D. 45 Theoretically, the 3 D of accommodation with low myopia might be sufficient for ordinary near work. LC atropine might retain more accommodation amplitude in comparison to 1% atropine. Therefore, the complaint of near blurring might be not serious and we also notice that the complaints are uncommon in clinical practice.
Recently, Tong et al. reported that rebound myopia progression was noticed after 2 years of high concentration of atropine (1%) treatment. 45 Unfortunately, in this study, we do not have the data to show the rebound condition with LC atropine treatment. In our opinion, if there is a rebound condition, LC atropine might be less severe than the high concentration. In addition, because myopia slowly progresses in early adulthood, if treatment could last for long term, the rebound effect might also be less severe in older age after long-term use. However, a further prospective study to examine this is warranted.
The major limitation of this study is that it is a retrospective. It lacked data including the drop-out rate, incidence of side effects such as photophobia, the extent of accommodation inhibition, and the role of other confounding factors such as parent myopia, near work time, and outdoor time. In addition, the smaller sample size of control is also noted even though the baseline demographic data are similar to the treatment group and the myopia progression rate is similar to other Asian studies. Still, the large sample size and long-term follow-up of this study provides some important information. However, a further large-scale, prospective, and randomized study is necessary to confirm this.
In conclusion, this study demonstrates that the regimen strategy of LC (0.05%–0.1%) atropine is effective to prevent myopia progression in myopic children in long-term follow-up. It provides a choice for the initial treatment of myopia children and might help to prevent myopic children from becoming high myopia patients later in life.
Footnotes
Acknowledgment
The authors thank Dr. Garbiel Gordon for reading and editing the manuscript.
Author Disclosure Statement
There is no proprietary interest for each author.