
Abstract
Abstract
Purpose:
The purpose of this study was to evaluate whether baseline visual acuity and baseline anatomy of the macula influence visual outcome in patients receiving intravitreal bevacizumab as treatment of exudative age-related macular degeneration (AMD) in clinical practice.
Methods:
This clinical case series study included 319 patients (406 eyes) who consecutively received intravitreal injections of bevacizumab for treatment of exudative AMD. The intervals between injections were 6 weeks and postinjection examinations were performed at 4 weeks after injection. Mean follow-up was 3.6 months.
Results:
After 3 injections of bevacizumab, best-corrected visual acuity (BCVA) significantly (P<0.01) improved in eyes with a baseline BCVA of less than 0.2 (group 1; 138 eyes; −0.10±0.43 LogMAR) and in eyes with a baseline BCVA ≥0.2 and <0.4 (group 2; 117 eyes; −0.06±0.24 LogMAR), but BCVA deteriorated in eyes with a baseline BCVA of ≥0.4 (group 3; 151 eyes; 0.09±0.32 LogMAR). Correspondingly, regression analysis revealed that improvement in BCVA after 3 intravitreal bevacizumab injections was significantly (P=0.001) associated with a low baseline BCVA. After the first injection of bevacizumab, changes in optical coherent tomography measurements of the macula (height of subretinal fluid, macular tissue thickness) were statistically significant for group 1 (P=0.03, P=0.03, respectively) and group 2 (P=0.01, P=0.02, respectively), but not for group 3 (P=0.85, P=0.22, respectively).
Conclusions:
In clinical practice, patients with exudative AMD and a baseline BCVA of <0.2 have a better prognosis for an increase in BCVA after intravitreal bevacizumab injections than patients with a higher baseline BCVA.
Introduction
Methods
The clinical interventional case series study included 319 patients (406 eyes) who were consecutively treated for exudative AMD with intravitreal injections of 1.5 mg bevacizumab. Inclusion criteria were the diagnosis of exudative AMD with subfoveal choroidal neovascularization. Exclusion criteria were signs of other retinal diseases, such as diabetic retinopathy or vascular occlusions. All patients were fully informed about the experimental character of the therapy, and all patients signed an informed consent. The present study was a retrospective analysis of the clinical data obtained during routine clinical care of the patients.
At baseline, all patients underwent an ophthalmological examination including refractometry and measurement of best-corrected visual acuity (BCVA), applanation tonometry, ophthalmoscopy, optical coherence tomography (OCT), and fluorescein angiography (FA). According to the appearance of the macula in FA, the choroidal neovascular membranes were divided into a classic type (purely classic component), a predominantly classic type (>50% classic component), a minimally classic type (≤50% classic component), an occult type, and a detachment of the retinal pigment epithelium. On the optical coherence tomograms, we measured the highest elevation of a detached retinal pigment epithelium, the greatest height of subretinal fluid, and the highest thickness of the macular retinal tissue.
The method of the intravitreal injection has been previously described in detail. 12 Briefly, prior to injection, topical anesthesia was applied, and the patients were completely draped as for any intraocular surgery. A lid speculum was inserted. In the temporal inferior region, 1.5 mg bevacizumab was injected with a sharp 27-gauge needle transconjunctivally at 3–3.5 mm from the limbus. After that, an antibiotic ointment (polymyxin and neomycine) was applied. The injections were repeated at intervals of 6–8 weeks. The follow-up examinations took place at 1 month after each injection.
Statistical analysis was performed using a commercially available statistical software package (SPSS for Windows, version 17.0; SPSS, Chicago, IL). Measurements of BCVA were converted into the logarithm of the minimum angle of resolution (LogMAR) for statistical calculation. Logistic regression analysis was performed to investigate the associations of the binary dependent variable “BCVA improvement or not” with the continuous or categorical independent variables, such as age and gender. Only 1 randomly selected eye per patient was included into the statistical analysis. The data that were normally distributed were presented as the mean±standard deviation. Where appropriate, 1-way analysis of variance and the paired Student's t-test were used. Confidence intervals were presented. All P values were 2-sided and were considered statistically significant when the values were less than 0.05.
Results
The study group included 319 patients [207 (65%) women; 406 eyes] with a mean age of 77.3±7.8 years (median: 79 years; range: 51–94 years). Mean intraocular pressure was 14.8±2.8 mmHg (range: 6–26 mmHg) and mean spherical equivalent power was 0.72±2.3 diopters. There were 220 (54.2%) phakic eyes and 186 (45.8%) pseudophakic eyes. In 36 (8.9%) eyes, treatment history included intravitreal injections of triamcinolone acetonide and photodynamic therapy. Fifty-six (14.4%) patients were known to have diabetes mellitus without diabetic fundus changes.
According to the baseline BCVA, the study population was divided into 3 study groups: group 1, with a baseline BCVA of less than 0.2 (138 eyes); group 2 with a baseline BCVA ≥0.2 and <0.4 (117 eyes); and group 3 with a baseline BCVA of ≥0.4 (151 eyes). The reason to choose the cutoff values for the definition of the 3 groups was to obtain roughly similarly sized groups. The change in BCVA during follow-up was not significantly different between the 3 study groups after the first or second intravitreal injection of bevacizumab (P=0.23 and P=0.67, respectively; Table 1). After 3 injections of bevacizumab, the changes in BCVA became significantly different between the 3 study groups (P<0.01; Table 1, Fig. 1). In study group 1 and study group 2, BCVA improved (group 1: −0.10±0.43 LogMAR; group 2: −0.06±0.24 LogMAR), but BCVA deteriorated in study group 3 (0.09±0.32 LogMAR). In addition, study group 3 was the only group in which BCVA was significantly lower at all 3 follow-up examinations when compared with the baseline value (P=0.03, P<0.01, and P=0.01, respectively; Table 1).
The P values were calculated by Student's t-test for paired samples (except the ANOVA calculation in the last column).
P<0.05.
P<0.01.
BCVA, best-corrected visual acuity; ANOVA, analysis of variance; RPE, retinal pigment epithelium.
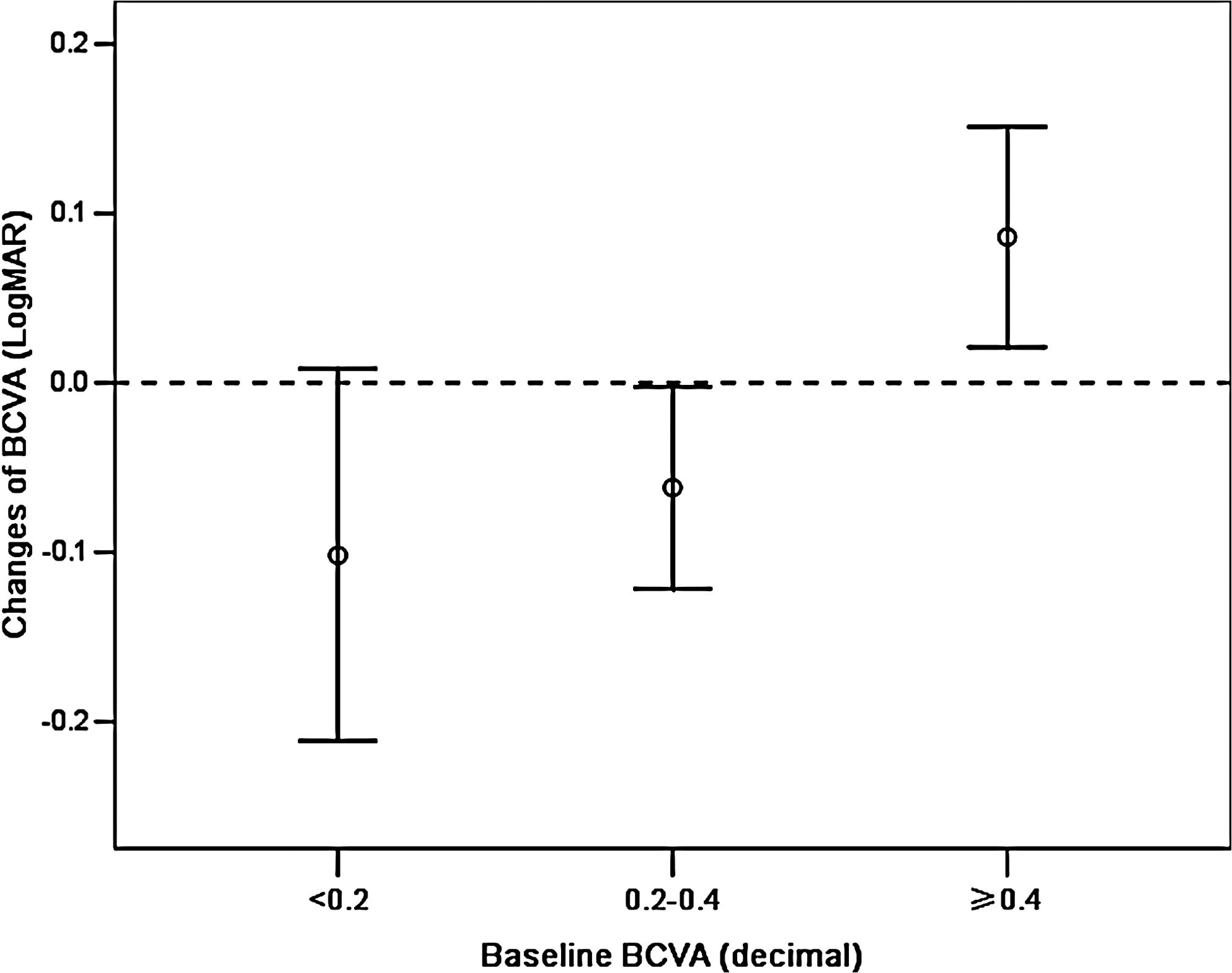
Diagram showing the changes in best-corrected visual acuity (BCVA, LogMAR) during follow-up in patients receiving intravitreal injections of bevacizumab for therapy of exudative age-related macular degeneration. Error bars: 95% confidence intervals; the difference between the groups was significant (P<0.01).
In a binary logistic regression analysis, the potential association between the presence or absence of an improvement in BCVA as dependent variable and age, baseline BCVA (LogMAR), type of the choroidal neovascular membrane, lens status, and presence of diabetes mellitus as independent variables was examined. It revealed that an improvement in BCVA after 3 intravitreal bevacizumab injections was significantly associated only with the baseline BCVA [P=0.001; regression coefficient=0.86; exponential B: 0.63; 95% confidence intervals (CI): 0.40, 0.99], whereas the type of subfoveal membrane (P=0.36; B=1.07; 95% CI: 0.93, 1.23), age (P=0.99; B=1.00; 95% CI: 0.97, 1.03), phakia versus pseudophakia (P=0.70; B=0.91; 95% CI: 0.57, 1.46), and diabetes (P=0.58; B=0.82; 95% CI: 0.41, 1.64) were not significantly associated with an improvement in BCVA.
After the first injection of bevacizumab, changes in the optical coherent tomography measurements of the macula (height of subretinal fluid, macular tissue thickness) when compared with baseline measurements were statistically significant for study group 1 (P=0.03 and P=0.03, respectively) and study group 2 (P=0.01 and P=0.02, respectively), but nor for study group 3 (P=0.85 and P=0.22, respectively) (Table 1). The changes detected after the second and third intravitreal bevacizumab injections when compared with the baseline values were significant for all 3 study groups (Table 1). After each injection, the reductions in macular thickness were more pronounced in study group 1 than in study group 2 and study group 3, although the difference between the study groups was not statistically significant (Table 1). After the second injection of bevacizumab, the change in the height of subretinal fluid was significantly more marked in study group 1 than in study group 2 and study group 3 (P<0.01) (Table 1).
Discussion
The results of our retrospective study demonstrate that patients with a low baseline BCVA have a better prognosis for an improvement in vision than patients starting at a relatively high level of BCVA. This result may be clinically important for the counseling of patients, that is, particularly those patients who still see relatively well may undergo deterioration in quality of vision, despite the repeated intravitreal injections of bevacizumab.
The results of our study may seem unsurprising and might have been anticipated, because it is easier to lose if one starts at a high level, and it is easier to gain if one starts at a low level. Correspondingly, a previous study on the potential benefit of intravitreal triamcinolone for therapy of exudative AMD also showed that the postoperative increase in visual acuity was significantly (P<0.001) and negatively correlated with preoperative visual acuity (correlation coefficient: −0.49). 13 In that study, the gain in visual acuity was significantly (P=0.009) higher if the preoperative visual acuity was less than 0.08 (gain: 3.2±2.9 Snellen lines) than if the preoperative visual acuity ranged between 0.08 and 0.20 (gain: 1.2±2.2 Snellen lines), or than if the preoperative visual acuity was higher than 0.20 (change: −0.8±3.4 Snellen lines).
Taking the whole study population independent of stratification by baseline BCVA, the finding of a significant improvement in BCVA after intravitreal injections of bevacizumab agrees with numerous previous reports.14–19 It is also in agreement with large randomized clinical trials on the effect of another antivascular endothelial growth factor, ranibizumab. 19 The finding that the improvement in visual acuity in our study was independent of the type of subfoveal choroidal neovascular membrane agrees with previous investigations in which the increase in visual acuity after intravitreal injections of bevacizumab for therapy of exudative AMD did not depend on the type of membrane.20,21
There are limitations in this study. First, the study design did not include a control group. Therefore, it cannot be concluded that the intravitreal injection of bevacizumab in eyes with a baseline BCVA of ≥0.4 leads to a deterioration of vision. Second, it is a retrospective data analysis with all limitations of such a study design. All eyes, however, had routinely received OCT examinations, and the patients were consecutively included into the study. Third, it is possible that not all factors influencing the visual outcome after intravitreal injection of bevacizumab for exudative AMD were included in the analysis. The conclusion is not, therefore, that the improvement of BCVA after intravitreal injection of bevacizumab for AMD depends on the baseline BCVA alone. Fourth, the follow-up was relatively short, so that no statements can be made with regard to the long-term prognosis.
In conclusion, patients with exudative AMD and a baseline BCVA of <0.2 in clinical practice have a better prognosis for an increase in BCVA after intravitreal bevacizumab injections than patients with a higher baseline BCVA. This may, however, not withhold the therapy of patients with a higher baseline BCVA.
Footnotes
Author Disclosure Statement
No competing financial interests exist.