
Abstract
Abstract
Purpose:
To evaluate the effectiveness of glycerin 1% formulated with the novel and proprietary ophthalmic excipient poly(
Methods:
This prospective single-center, single visit, randomized, double-masked exploratory trial compared the new formulation and Systane using TFBUT. Noninvasive break-up time (NIBUT) was measured in subjects with asymptomatic to mild (n=5), mild to moderate (n=5), and moderate to severe (n=6) dry eye disease using the TearscopePlus™ at pre-instillation and again at 15, 30, 60, and 120 min after instillation. Fluorescein break-up time (FBUT) was measured at 120 min after instillation.
Results:
At 15 min (N=16), the new formulation extended mean NIBUT by 14.67 s (P=0.05) compared with 7.40 s (P=0.34) by Systane. The new formulation had a mean FBUT of 4.92 s longer than Systane at 120 min (P=0.12). With outliers removed (N=13), the difference between the mean NIBUT change from baseline for the new formulation and Systane at 120 min was statistically significant (P=0.03).
Conclusions:
This study demonstrates that PLL-g-PEG as a polymer excipient in artificial tears is effective in improving the performance of demulcents to significantly prolong NIBUT at 15 min, and that protective activity from this artificial tear product for 2 or more hours after eye drop instillation is possible.
Introduction
Disturbances in the stability of the tear film can result in a condition known as dry eye disease. The 2007 Report of the International Dry Eye Workshop produced the following definition for dry eye disease: “Dry Eye is a multifactorial disease of the tears and ocular surface that results in symptoms of discomfort, visual disturbance, and tear film instability with potential damage to the ocular surface.” 5 Dry eye disease results in reduced tear film stability and rapid tear film break-up time (TFBUT). 6
Dry eye disease is a common condition that affects millions of people in the United States. The prevalence of dry eye disease has been estimated to range from 5% to 35%.7–9 An estimated 4.91 million Americans aged 50 years and older have dry eye disease, and tens of millions more have less severe or episodic symptoms of the condition.7–9 One in 4 patients who visit an ophthalmic clinic report symptoms of dry eye disease, making it one of the most common conditions encountered in ophthalmology. 10 The mainstay of treatment for dry eye disease is the use of over-the-counter (OTC) artificial tear preparations.
One way to evaluate the effectiveness of an artificial tear preparation is to measure the TFBUT before and after eye drop instillation. Tear film stability as measured by TFBUT is an important indication of artificial tear efficacy. Although there is no single “gold standard” test to evaluate the efficacy of treatment, there is evidence that TFBUT is more repeatable than other objective tests of dry eye disease. 11 TFBUT can be determined using fluorescein break-up time (FBUT) or noninvasive break-up time (NIBUT). FBUT is tested by instilling a small standard volume of fluorescein into the eye and recording the time from a blink to tear film break-up as seen under the cobalt blue light of slit-lamp microscope. NIBUT is tested by projecting a pattern onto the corneal surface and recording the time from a blink until the pattern is distorted.
Evaluation of tear film stability using NIBUT has advantages over other techniques because it does not introduce substrate into the eye and allows the observer to evaluate tear film in vivo. Introducing fluorescein into the eye may significantly reduce TFBUT. 12 One instrument used to measure NIBUT is the Keeler Tearscope Plus™. The instrument has been shown to be a reliable method to measure NIBUT. 13
Currently, even the best artificial tear products on the market provide only limited extensions of TFBUT. The mean TFBUT extension usually peaks 5–20 min after instillation of an artificial tear.14–17 One study that evaluated the performance of an artificial tear containing propylene glycol (0.3%) and polyethylene glycol (0.4%) as active demulcents with hydroxypropyl-guar as a gelling agent (Systane® Lubricant Eye Drops; Alcon) found that the mean TFBUT extension peaked at 20 min postinstillation. 14 The same study also found that TFBUT extension peaked at 5 and 10 min for artificial tears that contained 1% glycerin and 1% polysorbate 80 (Refresh Endura; Allergan, Inc.) and 0.5% carboxymethylcellulose sodium (Refresh Tears; Allergan, Inc.), respectively, as active demulcents.
Further, most artificial tears lose their effectiveness within ∼1 h.14–18 Depending on the specific artificial tear product, TFBUT usually returns to baseline (pre-instillation) 20–90 min after instillation.14–17 Few studies measure TFBUT at 120 min after instillation of an artificial tear.
Increasing the viscosity of artificial tear formulations is one approach used to prolong TFBUT. 19 This effect was demonstrated in a study that compared the performance of a mid-viscosity artificial tear with low-viscosity artificial tears. 15 The highest viscosity tear prolonged TFBUT at least 20 min while the low-viscosity tears prolonged TFBUT only 5–10 min. 15 Higher viscosity artificial tears, while providing prolonged ophthalmic lubrication and protection, are associated with visual disturbances and are typically not well tolerated.
Drug product formulation is critical to maximizing the benefits of an active pharmaceutical ingredient. The Food and Drug Administration specifies which ophthalmic demulcents are suitable as active ingredients in OTC ophthalmic drug products. 20 Glycerin is among the listed demulcents and can be used in concentrations from 0.2% to 1%. 20 In addition to the active ingredient, ophthalmic drug products often contain excipients, such as polymers, electrolytes, buffers, polymers, surfactants, and preservatives. Manufacturers include inactive ingredients in their artificial tear formulations to enhance the performance of the active agent. Excipients used in this regard include hydroxypropyl guar, hyaluronic acid, carbomer, osmoprotective solutes, and others.
In this study, a new formulation of glycerin 1% artificial tears with the novel excipient poly(
PLL-g-PEG was incorporated into the new formulation of a glycerin-based artificial tear to help retain and more evenly distribute the glycerin solution on the surface of the eye. PLL-g-PEG is a water-soluble, polycationic graft copolymer that consists of a PLL backbone and PEG side chains grafted to the PLL backbone (Fig. 1). The PLL-g-PEG molecule used in this trial has an average molecular weight of 73,000 Da. The PLL backbone carries multiple positive charges and spontaneously adsorbs from aqueous solution onto negatively charged surfaces (such as conjunctival and corneal epithelium) through electrostatic interaction.21–22 The PEG side chains are the hydrophilic block of the polymer and are sometimes referred to as combs or brushes.
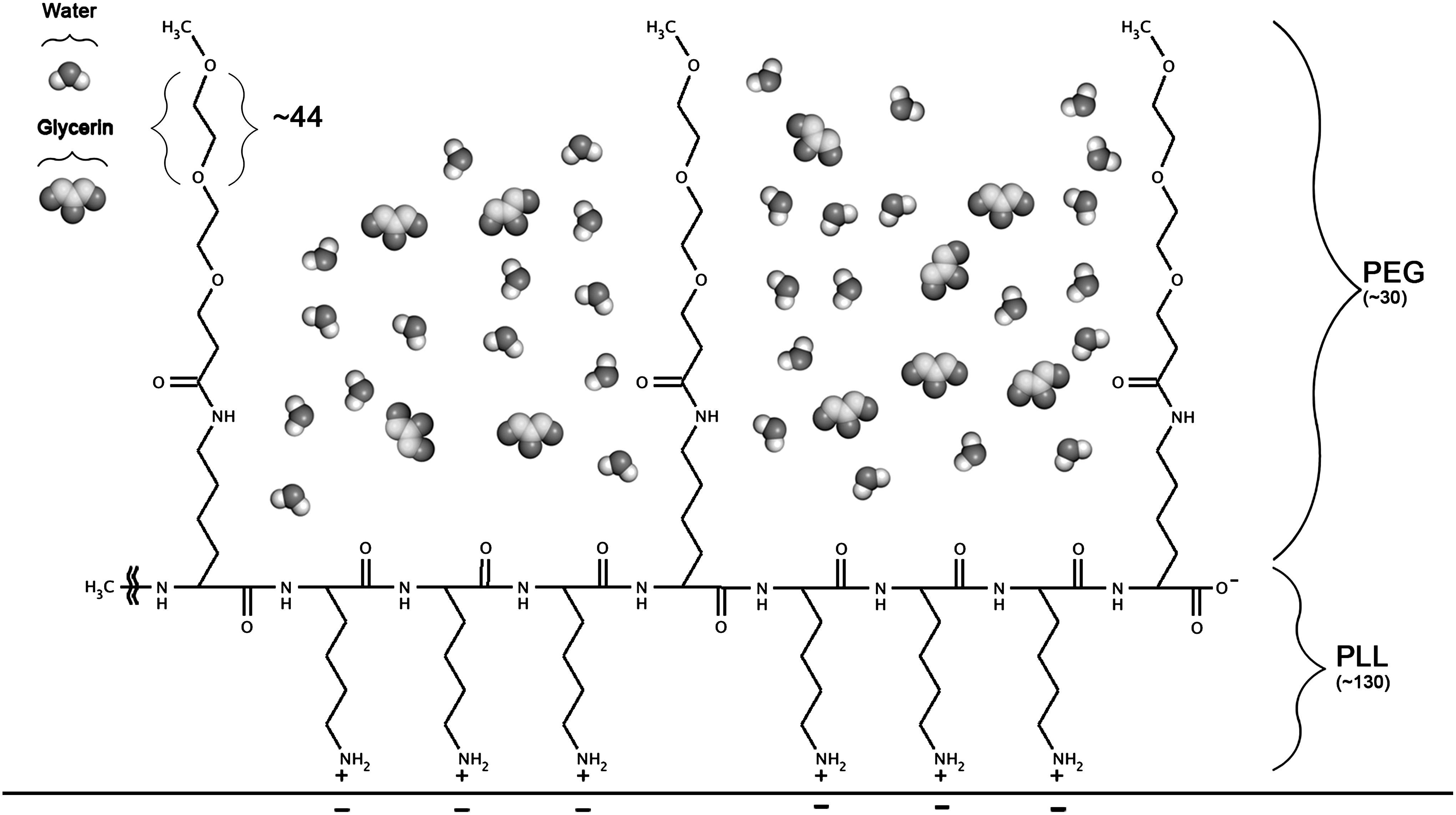
Poly(
The PEG brushes retain water (and glycerin in this case), keeping a coated surface wet and lubricated. PLL-g-PEG glycerol solutions have been shown to enhance the lubrication of surfaces in vitro.28,29 Thus, it is possible that PLL-g-PEG copolymer excipients will play an important role in improving the performance of drug products in the treatment of dry eye disease in the future.
Methods
Setting
This single-center, single visit, randomized, double-masked exploratory trial compared the extension of TFBUT between a new formulation of glycerin 1% (Eyeon Protect™; active ingredients: glycerin 1%; inactive ingredients: mannitol, PLL-g-PEG, poloxamer 407, sterile water for injection, sodium phosphate buffer, and mannitol; Eyeon Therapeutics, Inc.) and a market-leading artificial tear formulation (Systane Lubricant Eye Drops; active ingredients: polyethylene glycol 400 0.4% and propylene glycol 0.3%; inactive ingredients: boric acid, calcium chloride, hydroxypropyl guar, magnesium chloride, potassium chloride, purified water, sodium chloride, and zinc chloride; Alcon).
Study population
The population size (N=16) for this exploratory trial was determined empirically by the principal investigator (J.V.A.). Three groups of eligible subjects were enrolled at the University of Rochester Eye Institute (previous name of Flaum Eye Institute) in order to assess the performance of the 2 artificial tear products in patients with different degrees of dry eye disease. The study groups were asymptomatic to mild dry eye (Group 1; n=5), mild to moderate dry eye (Group 2; n=5), and moderate to severe dry eye (Group 3; n=6). Inclusion criteria for all 3 groups were age ≥18 years and the ability to give informed consent. Inclusion criteria for Groups 2 and 3 were a recent ocular history of dry eye symptoms in both eyes and current use of some form of OTC artificial tear. An additional inclusion criterion for Group 3 was objective findings of dry eye disease on the most recent eye exam. The exclusion criterion for Group 1 was symptoms of dry eye disease in the past 30 days. Exclusion criteria for all groups included use of artificial tears within 36 h of the study, or contact lenses or periocular cosmetics the day of the study.
The informed consent and protocol were approved by the Research Subjects Review Board at the University of Rochester School of Medicine and Dentistry in Rochester, New York. Informed consent was obtained from the subjects in this study. The ClinicalTrials.gov identifier is NCT00681265. This study is in accordance with HIPAA regulations. This study adhered to the tenets of the Declaration of Helsinki.
Intervention procedures
After meeting all of the inclusion/exclusion criteria and obtaining informed consent, qualified subjects were asked several questions at baseline (pre-instillation) about their eyes and an ophthalmic examination with standard slit lamp was performed of each eye with pertinent findings recorded. NIBUT was then measured in each eye by interferometry using the Tearscope Plus (Keeler Instruments, Inc.). The subject was instructed to blink twice and then hold their eyes open. Using the grid filter and stopwatch function of the Tearscope Plus, the trained examiner recorded NIBUT as the time from the second opening of the eyelid until the first significant appearance of distortion in the grid pattern on the corneal tear film surface. A black patch was placed over the eye not being examined. If the subject inadvertently blinked during the test sequence before tear film break-up was observed, then the subject was instructed to rest briefly and then the measurement was repeated with reinforcement of the instructions. The waiting room and all exam rooms were maintained at the same temperature and relative humidity. There was no airflow detectable in any exam rooms or in the waiting area.
For uniformity of delivery and to maintain patient and examiner masking, in a different location under sterile conditions, an unmasked investigator transferred 100 μL of each solution from the product's original packaging into a sterile 1 cc tuberculin syringe that was then capped. One set of syringes was created for each subject and the syringes were color coded. Using a predetermined randomization schedule generated by the study statistician based upon a 50/50 chance, 1 eye of the subject received a masked 50 μL drop of Eyeon Protect. The other eye received a masked 50 μL drop of Systane.
After instillation and at the conclusion of the study, subjects were asked several questions about their eyes. Although there was a comparison question at the 5-min time point, the questionnaire was primarily designed to assess safety, not compare the drops based on subjective symptoms. NIBUT was measured again in each eye using the Tearscope Plus at 15, 30, 60, and 120 min after instillation. Following the 120 min of NIBUT measurement, a final ophthalmic examination with slit lamp was performed of each eye with pertinent findings recorded. FBUT was then measured in each eye. A final set of questions was administered before subjects were debriefed and dismissed. A follow-up phone call was placed 24 h later to check for adverse events.
Viscosity measurements for the new formulation of glycerin 1% with polymer excipients and Systane were made with a Rotational Rheometer (TA-AR1000; TA Instruments). Flow curves were measured for all samples from 0.1 to 1,000 Pa using a 40-mm plate with a 500-μm gap. Using rotational rheometry, viscosity was measured for Eyeon Protect (Eyeon Therapeutics lot No. NB# 211–46) and Systane (Alcon lot No. 80088A).
Main outcome measures
Three cohorts were included in the study: asymptomatic to mild, mild to moderate, and moderate to severe dry eye symptoms. Analyses were performed together for all subjects who met inclusion/exclusion criteria and completed the study (N=16).
Efficacy measures were NIBUT at 15, 30, 60, and 120 min and FBUT at 120 min. The predetermined primary efficacy endpoint was calculated as area under the curve (AUC) from the time of tear drop instillation until NIBUT returned to baseline level. NIBUT was set to the baseline time for any value that fell below the time zero measurement. If NIBUT had not returned to baseline by the final measurement, 120 min was used to calculate AUC. Secondary efficacy endpoints were NIBUT extension at each time point, FBUT at 120 min, and predicted NIBUT return to baseline. NIBUT extension was calculated as the difference between NIBUT at a given time point and the baseline NIBUT. Predicted NIBUT return to baseline was an estimate of the time from tear drop instillation until NIBUT returned to baseline level. Information gained from the questions at pre-instillation, 5 min after instillation, 120 min after instillation, and 24 h later was tabulated and summarized.
Analysis of change within either Systane or Eyeon Protect groups was performed by paired t-tests, in which the difference from baseline to a subsequent time point was tested against the null hypothesis of no change. Difference between the 2 groups was assessed by t-tests. A significance level of α=0.05 was used for all tests.
Results
A total of 16 subjects were enrolled in the study. All 16 subjects met enrollment criteria and completed the study. For all subjects (N=16), the range of dry eye disease included the following: 5 asymptomatic to mild, 5 mild to moderate, and 6 moderate to severe. The mean age for subjects was 44.5 years. Ten subjects were women (62.5%) and 6 subjects were men (37.5%). In this sample, all subjects were Caucasian. No prohibited concomitant medications were in use, and no patients used any eye drops within 36 h of the study start time.
Safety
No adverse events were reported during the entire study. There were no changes in the ophthalmic examination with slit lamp from baseline to 120 min. Safety was noted in 3 distinct patient populations with dry eye disease: asymptomatic to mild, mild to moderate, and moderate to severe. There were no complaints reported during the study or the 24 h follow-up call for any subject.
Efficacy
Primary data analysis (N=16) demonstrated that the new, specifically engineered, formulation containing glycerin 1% with PLL-g-PEG significantly extended mean NIBUT by 14.67 s at 15 min (P=0.05) compared with pre-instillation NIBUT (Fig. 2). Systane, which is a market-leading product, extended mean NIBUT by 7.40 s at the same time point (P=0.34). The new formulation had a mean FBUT difference from baseline 4.92 s longer than Systane at 120 min (P=0.12) (Fig. 3). The AUC was numerically superior for Eyeon Protect versus Systane (3,007–1,735 minute-seconds, respectively), but the difference was not statistically significant (P=0.29). Likewise, the predicted return to baseline was superior for Eyeon Protect versus Systane (86–74 min, respectively), but the difference was not statistically significant. Data analysis was stratified by cohort; however, due to the small n, statistically significant differences in mean NIBUT between Eyeon Protect and Systane for Group 1 (n=5), Group 2 (n=5), or Group 3 (n=6) were not detected.
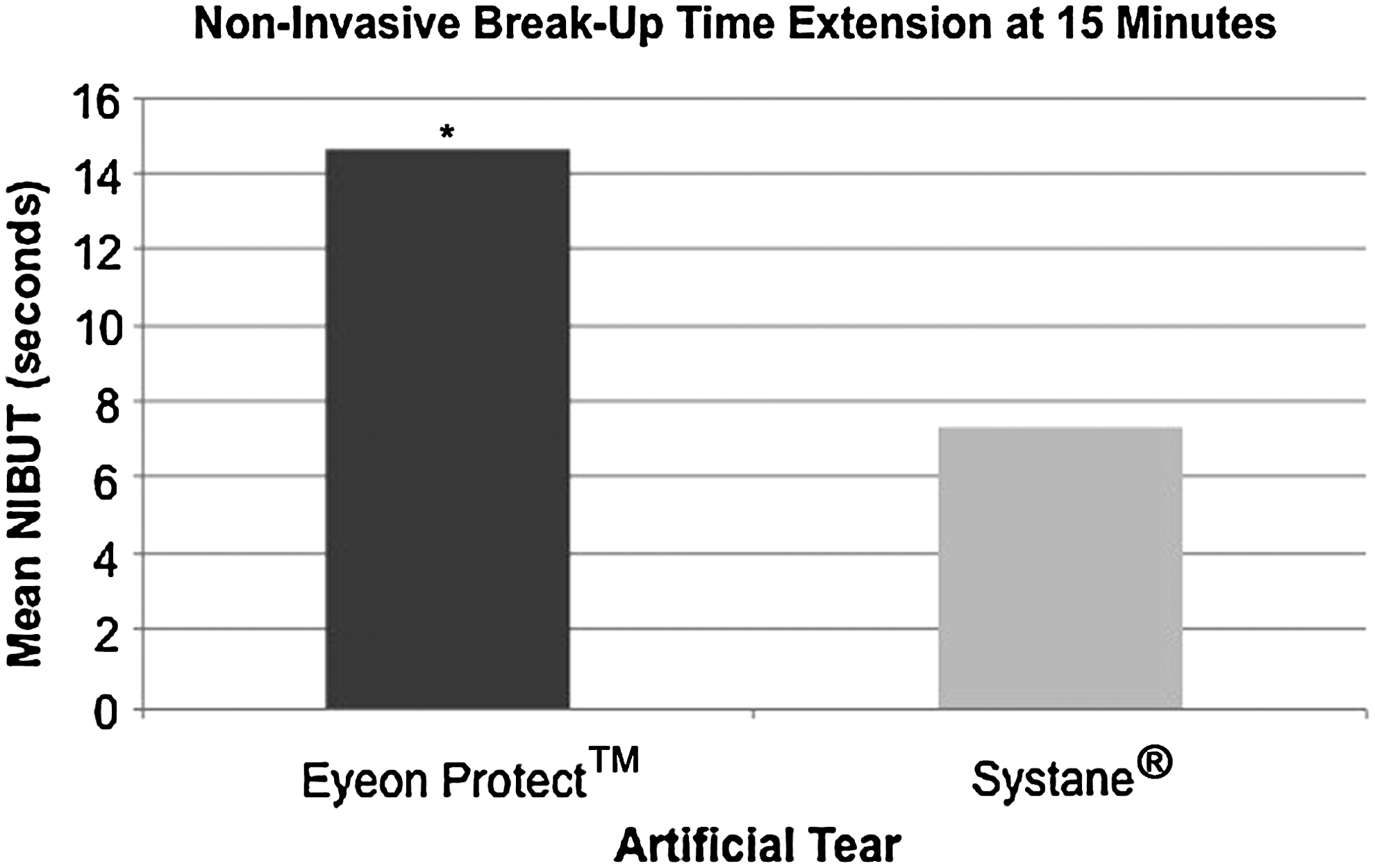
Mean noninvasive break-up time (NIBUT) extension at 15 min (N=16). *Eyeon Protect™ significantly extended NIBUT by 14.67 s at 15 min (P=0.05).

Mean fluorescein break-up time (FBUT) at 120 min (N=16). *Eyeon Protect had an FBUT 4.92 s longer than Systane® at 120 min (P=0.12).
Prior to unmasking the data set, it was noted that several subjects with very long baseline NIBUT values skewed the mean values at some time points in the small study group; the principal investigator and statistician decided to generate a secondary post hoc analysis by removing all subjects with NIBUT ≥30 s at baseline. This decision made physiological sense as subjects with prolonged NIBUT are not individuals who would (at that time) need or benefit from the use of artificial tears, and such long and atypical NIBUT values can affect statistical analysis in small cohorts. Three subjects were removed from the data based upon this criterion and a secondary data analysis (N=13) was performed. One subject was removed from each cohort.
With outliers removed (N=13), mean NIBUT extension at 15 min for the new formulation was 12.61 s (P=0.08) (Fig. 4). Mean NIBUT extension for Systane at the same time point was 5.17 s (P=0.32). The difference between the mean NIBUT for the new formulation and Systane at 120 min was 3.5 s longer for the new product, and this difference was statistically significant (P=0.03).
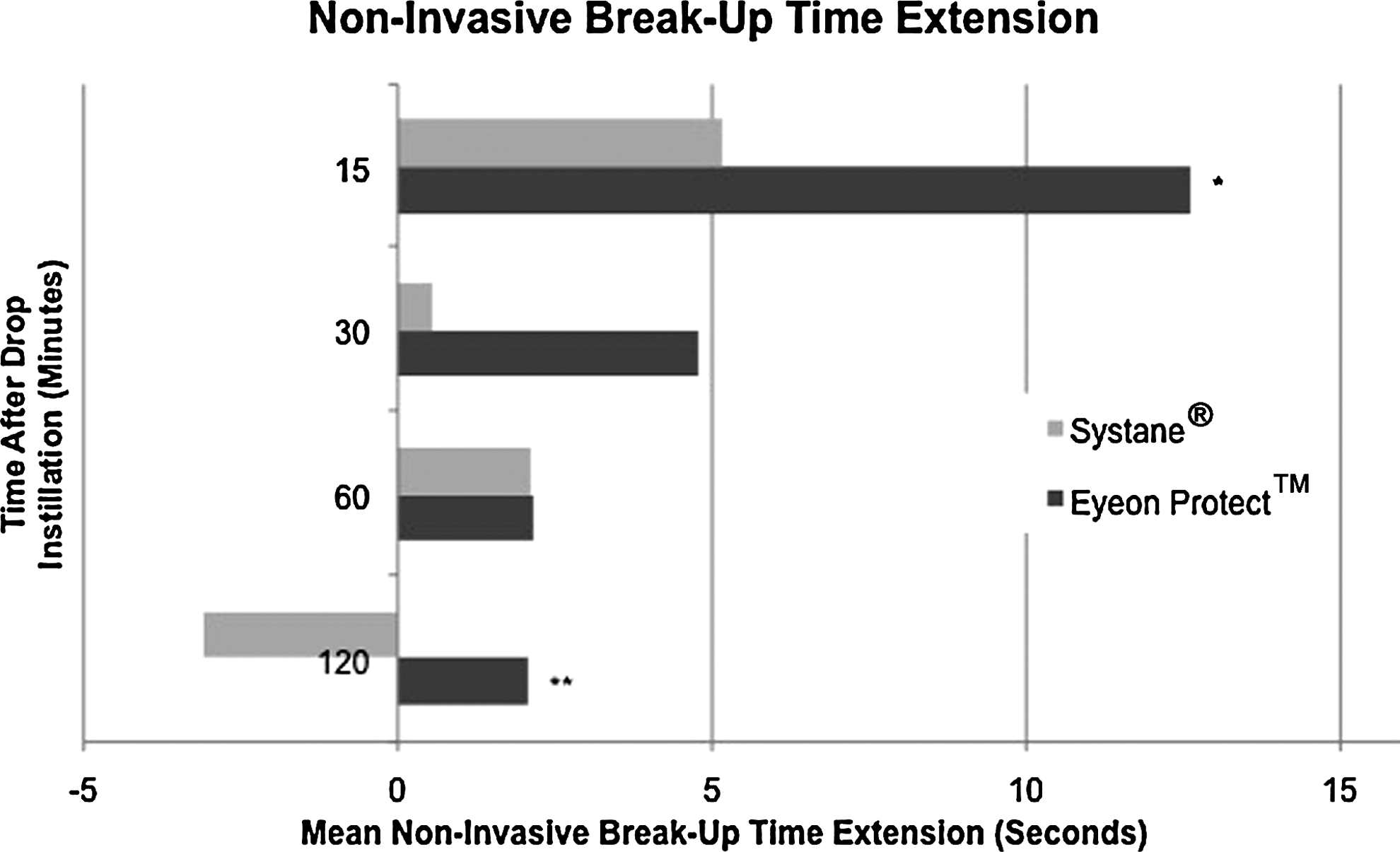
Mean NIBUT extension with outliers removed (N=13). *Eyeon Protect extended mean NIBUT at 15 min (P=0.08). **Eyeon Protect had a mean NIBUT significantly longer than the Systane at 120 min (P=0.03).
With outliers removed (N=13), mean NIBUT at baseline (pre-instillation) for Eyeon Protect and Systane was 7.18±5.82 and 8.85±7.80 s, respectively. Mean NIBUT for the new formulation at 15, 30, 60, and 120 min was 19.78±28.20, 11.94±13.17, 9.33±9.25, and 9.26±6.49 s, respectively. Mean NIBUT for Systane at 15, 30, 60, and 120 min was 14.02±18.00, 9.38±7.95, 10.98±10.74, and 5.76±4.72 s, respectively.
Subject responses to questions about the eye drops 5 min after instillation were recorded. Four subjects (25%) preferred Eyeon Protect, 5 subjects (32%) preferred Systane, and 7 subjects stated there was no difference between the 2 eye drops at 5 min. Two subjects said Systane led to temporary blurry vision, while no subjects reported visual changes after instillation of Eyeon Protect. Subject responses at 2 h were similar for the 2 products.
The viscosity of Eyeon Protect was lower than the viscosity of Systane. Viscosities were determined by Particle Sciences, Inc., using rotational rheometry. The viscosity of Eyeon Protect and Systane at 10 Pa shear stress was 2.7303 cP and 5.211 cP, respectively.
Discussion
This study demonstrates that glycerin 1% formulated with PLL-g-PEG as an excipient can significantly prolong NIBUT at 15 min, and that measurable protective activity from an artificial tear product for at least 2 h after eye drop instillation is possible. In the primary analysis, mean NIBUT extension at 15 min was significantly longer for Eyeon Protect compared with Systane. In addition, mean FBUT for Eyeon Protect was almost 5 s longer than Systane. The secondary analysis with outliers removed showed that the difference between the mean NIBUT of Eyeon Protect and Systane at 120 min was statistically significant. These results are particularly interesting as this was a pilot study with a small number of subjects. It was not powered to demonstrate efficacy yet meaningful differences in the metrics between the 2 products were observed. Further, Eyeon Protect was not formulated to optimize performance; it was primarily designed to assess in a small trial the ability of PLL-g-PEG to enhance the performance of demulcents in OTC artificial tears.
Importantly, this study showed excellent safety in all subjects. There were no adverse events, and the new artificial tear solution was shown to be safe in this study among 3 distinct populations: those with mild, moderate, and severe dry eye.
In retrospect, the AUC should not have been chosen as the primary endpoint. There were too few time points over the 120-min period and under the statistical methodology the NIBUT was truncated at 120 min. Although conceptually AUC could be an interesting way to look at prolongation of TFBUT, it is not recommended until further more meaningful methodology is developed. Similarly, although an estimate of NIBUT to return to baseline after eye drop instillation is an appealing statistical metric for dry eye products, large jumps in time points and no measure after 120 min made this predetermined variable less meaningful than anticipated.
The extension of TFBUT seen with Eyeon Protect is due to its unique formulation; blinking and the lacrimal system would wash away a simple glycerin 1% aqueous solution within minutes of instillation. PLL-g-PEG in aqueous solution has been shown to adsorb onto negatively charged surfaces through electrostatic attraction.21,22 We hypothesize that interactions between PLL-g-PEG, glycerin, and the negatively charged epithelial cells and membrane-bound mucins allow for prolonged corneal residence time of both the graft copolymer and the active agent. This results in increased tear film stability on the ocular surface and thus prolonged TFBUT.
The prolongation of TFBUT by Eyeon Protect is not due to high viscosity. The viscosity of the new formulation is lower than all the other commercial eye drop samples measured in this study. Therefore, it provides the benefit of increased TFBUT without the visual blurring and eye discharge encountered with high-viscosity artificial tears.
In conclusion, the use of PLL-g-PEG as an excipient in an artificial tear formulation of glycerin 1% is a promising therapy for dry eye disease. Its unique formulation significantly extends TFBUT. Increasing TFBUT is important in the treatment of dry eye disease because it can improve the clinical signs and symptoms of dry eye disease and promote epithelial repair. Widespread topical ophthalmic opportunities exist for this novel polymer system and development is ongoing.
Footnotes
Acknowledgments
Elisabeth Carter works as an Administrative Assistant in Flaum Eye Institute, Rochester, New York. This work was funded by Eyeon Therapeutics, Inc., Rochester, New York.
Author Disclosure Statement
Financial disclosures: William G. Gensheimer: none; David M. Kleinman: Bausch and Lomb, Inc., Eyeon Therapeutics, Inc., GlaxoSmithKline, Lumetrics, Inc., MacuSight, Inc., and Talecris Biotherapeutics, Inc.; Mithra Gonzalez: none; Deepak Sobti: none; Eugene R. Cooper: Eyeon Therapeutics, Inc.; Gerard Smits: none; Andrew Loxley: Particle Sciences, Inc.; Mark Mitchnick: Kolltan Pharmaceuticals, Inc., Particle Sciences, Inc., Procter and Gamble, and Teva Pharmaceutical Industries Ltd.; James V. Aquavella: Allergan, Inc., and Bausch & Lomb, Inc.