
Abstract
Abstract
Purpose:
To evaluate the clinical outcomes and biologic effects on the aqueous humor concentrations of vascular endothelial growth factor (VEGF) in patients with neovascular glaucoma (NVG) treated with intravitreal bevacizumab (IVB).
Methods:
Twenty-nine consecutive patients (35 eyes) treated with 1.0- or 0.1-mg injections of IVB for NVG between January and December 2009 were enrolled in this retrospective, interventional pilot study. The visual prognosis and changes in intraocular pressure (IOP) were followed for >6 months after the initial injection. Aqueous humor samples were obtained at the initial IVB injection from all study eyes and 1 week after the first injection in eyes undergoing a second intervention to measure the VEGF concentration.
Results:
The VEGF concentrations in the 35 eyes significantly correlated (r=0.535, P<0.001) with the pretreatment IOP. The mean reductions of the VEGF levels 1 week after IVB did not differ significantly between the 1.0- and 0.1-mg groups (P=0.738). Despite more repeated injections in the 0.1-mg group and additional medical or surgical interventions in both groups, both dosages inhibited the neovascular activity. The ability to control the IOP after IVB did not differ significantly between groups at 1 week (P=0.625) and 6 months (P>0.99). Visual improvements also did not differ significantly between groups during the 6-month follow-up (P=0.437).
Conclusions:
Aqueous humor levels of VEGF were significantly correlated with the IOP. Low-dose (0.1 mg) IVB was as effective as the currently used higher dose (1.0 mg) for treating NVG within at least 6 months after the initial injection.
Introduction
Vascular endothelial growth factor (VEGF), an endothelial cell-specific angiogenic factor, plays a central role in iris neovascularization and NVG.8,9 Preclinical primate studies have shown that an intravitreal injection of VEGF is sufficient to produce iris neovascularization, and intravitreal VEGF antibodies effectively halt the experimentally induced iris neovascularization.10,11 Aqueous humor levels of VEGF in patients with ischemic retinal pathologies are highly elevated and stimulate human endothelial cell migration and proliferation in vitro. 8 Based on these experimental and clinical findings, anti-VEGF pharmacotherapy to target VEGF was proposed as another encouraging therapy to treat ocular neovascularization. 12 Bevacizumab (Avastin, Genentech, South San Francisco, CA), a humanized monoclonal antibody against all VEGF isoforms, has promising potential to treat iris neovascularization and NVG.13–18 The off-label use of intravitreal bevacizumab (IVB) stabilizes neovascular activity and controls IOP in patients with iris and/or gonio-neovascularization alone and in early stage NVG without angle closure, even though repeated injections are required in some cases. 18 In advanced NVG, although IVB alone may not stabilize elevated IOP, IVB can be used as a preoperative adjunct to improve the quality and safety of surgery.15,16,18,19 Although these encouraging results may suggest that bevacizumab should be the first treatment of choice for NVG, the appropriate dosage and injection interval for IVB to treat NVG has not yet been established. The current intravitreal dose (1 mg or more) excessively reduces the increased VEGF concentration to far under the physiologic level in patients with diabetic retinopathy. 20 Since VEGF has several physiologic functions, that is, maintenance of the choriocapillaris and neuroprotection for ganglion cell survival,21–25 suppressing the intraocular VEGF concentration to far under the physiologic level raises concerns about circulatory disturbances and/or neural degeneration, which may result in irreversible visual impairment in patients with advanced NVG and its responsible ischemic retinal pathologies.26–29 If a lower dose of bevacizumab can control the VEGF concentration to a physiologic level with adequate treatment efficacy to halt neovascular activities, then it would be more appropriate and safer than the current dosage of 1.0 mg or more for treating NVG. Although many studies have reported the efficacy of IVB for managing NVG based on changes in IOP and fluorescein angiographic findings, a few studies in a MEDLINE search have quantitatively evaluated the changes in the aqueous humor concentration of VEGF resulting from IVB in a large case series of patients with advanced NVG.30,31
We investigated the clinical outcomes and changes in the aqueous humor levels of VEGF in patients with NVG treated with 0.1 mg of IVB and determined the biologic effect, safety, and potential for low-dose bevacizumab for treating NVG.
Methods
The current study was approved by the institutional review board of Osaka University Medical School Hospital, conducted in accordance with the principles stated in the Declaration of Helsinki, and complied with the Health Insurance Portability and Accountability Act. Consecutive patients who presented to the Department of Ophthalmology, Osaka University Medical School Hospital for treatment of NVG unresponsive to previous lazer photocoagulation and/or antiglaucoma medical treatment between January and December 2009 were enrolled in this retrospective study. Patients who had previously undergone intravitreal pharmacotherapy such as triamcinolone acetonide and/or injection of an anti-VEGF drug, or antiglaucoma surgery such as trabeculectomy, implant surgery, and cyclo-destructive surgery were excluded. All patients provided informed consent before every interventional procedure and agreed to the collection and analysis of samples that would have been discarded at the time of injection or surgery. All patients underwent detailed ophthalmologic examinations including measurement of the best-corrected visual acuity (VA), slit-lamp biomicroscopy, funduscopy, gonioscopy, and IOP measurements before and after IVB and surgery. The iris neovascularization was considered as having decreased based on the caliber of the neovascular lumen; angle neovascularization was considered as having regressed based on resolution of the neovasculature in more than one quadrant. Anterior segment slit-lamp photography and iris fluorescein angiography were performed in selected cases. Fundus photographs were obtained only in patients in whom the fundus was visible.
IVB and sample collection
From January to June 2009, a bevacizumab dose of 1.0 mg in 40 μL (1.0-mg group) was intravitreally injected ; from July to December 2009, a bevacizumab dose of 0.1 mg in 40 μL (0.1-mg group) was injected. If a repeat injection was necessary, then the dose was the same as the initial dose used in individual eyes. For intravitreal injection, a 50-μL aliquot of commercially available bevacizumab (25 mg/mL) was prepared, placed in a tuberculin syringe with a 29-gauge needle, and stored at −80°C until use. For low-dose administration, the prealiquot bevacizumab (1.25 mg/50 μL) was diluted by an additional 10% to 0.125 mg/50 μL with balanced saline plus solution (Alcon Laboratories Inc., Fort Worth, TX). An intravitreal injection of bevacizumab in all study eyes was administered according to a modified strict aseptic protocol. 32 Briefly, after topical anesthesia with 4% lidocaine and conjunctival disinfection with 1.25% povidone iodine solution, bevacizumab (1 mg/40 μL or 0.1 mg/40 μL) was injected into the vitreous cavity via the pars plana. A 200-μL sample of undiluted aqueous humor was obtained by using a 30-gauge needle immediately before the injection of bevacizumab. One week after the initial injection, another injection of bevacizumab, the dose of which was the same as the first injection, was considered for patients with neovascularization refractory to the initial injection or in those with IOP ranging from 22 to 29 mmHg even after the initial injection; surgery such as trabeculectomy, pars plana vitrectomy, or both were performed in patients with IOP exceeding 30 mmHg despite intensive antiglaucoma medications. Another 200-μL sample of undiluted aqueous humor was then obtained immediately before injection or surgery. An undiluted aqueous humor sample (200 μL) also was obtained immediately before cataract surgery from the control patients undergoing cataract surgery. All samples from the study and control groups were collected in sterile syringes, immediately transferred to dry ice, and stored at −80°C until an assay was performed. The technician was masked to the samples.
Measurement of aqueous humor levels of VEGF
Aqueous humor levels of VEGF were measured by using an enzyme-linked immunosorbent assay (Quantikine®, Human VEGF immunoassay, R&D System Inc., Minneapolis, MN) for human VEGF. The primary antibody against VEGF detected 2 major soluble forms (VEGF121 and VEGF165) of the 4 VEGF isoforms. An experienced technician from Mitsubishi Chemical Evidence Inc., Tokyo, Japan, masked to the sample details performed the assays. According to the manufacturer's instructions, 100 μL per sample was used for each assay. The optical density was determined at 450 nm by using absorption spectrophotometry. The mean of 2 readings was used for quantitative analysis. The limit of the detectable VEGF concentration was 15.6 pg/mL.
Data analysis
The patient medical records were reviewed for gender, age, preexisting ischemic retinal disorders, previous treatments, lens status, follow-up period, and changes in VA and IOP before and after treatments. The regression and recurrence rates of iris neovascularization and NVG, the number of repeated injections of IVB, changes in the number of topical antiglaucoma medications if previously administered, type of additional surgery, and systemic and local adverse events related to the injection also were followed for 6 months after the initial IVB. The VA, measured using the Landolt C acuity chart, was analyzed on a logarithm of minimal angle of resolution (logMAR) scale. Counting fingers vision was defined as 0.01 (2.0 logMAR units), hand movements as 0.005 (2.3 logMAR units), and light perception only as 0.002 (2.7 logMAR units), according to previous studies (available at www.iovs.org/cgi/eletters/47/3/1236).33,34 Visual changes were defined as a change of 0.3 or more logMAR unit.
Baseline data with a normal distribution are presented as the mean±standard deviation. Since the distribution of the VEGF concentration was skewed, the VEGF concentration was transformed into logarithmic scale (logVEGF) for statistical analysis and expressed as the mean and the range. The within-subject correlation was adjusted by using generalized estimating equations for subsequent data analyses. When comparing the impact of the 2 doses of bevacizumab on the changes in the aqueous humor VEGF concentrations and IOP, stepwise regression analysis with analysis of covariance (ANCOVA) was performed to eliminate the effect of potential confounders on the baseline characteristics. The Student's t-test was performed to compare normally distributed unpaired continuous variables between the 2 groups (1.0-mg vs. 0.1-mg). The chi-square or Fisher's exact test was performed to compare the variables between groups as appropriate. To examine the relations between the aqueous humor VEGF levels and IOP, Pearson's correlation coefficient was calculated. We performed the calculations based on the data including the cut-off values (15.6 pg/mL) when the samples had VEGF levels under the detectable limit. All statistical analyses were performed by using the commercially available software program JMP 8.0 for Windows (SAS Institute Japan Inc., Tokyo, Japan). P<0.05 was considered statistically significant.
Results
A total of 35 eyes of 29 patients (10 women, 19 men; mean age, 64.5±11.8 years; range, 45–92) were included. The mean follow-up period was 7.5±1.2 months. Of the 35 eyes, the underlying ocular pathologies causing NVG were proliferative diabetic retinopathy in 22 (63%) eyes, central retinal vein occlusion in 6 (17%) eyes, ocular ischemic syndrome in 3 (8.5%) eyes, uveitis in 3 (8.5%) eyes, and central retinal artery occlusion in one (3%) eye. PRP had been previously applied in 7 (20%) eyes and was insufficient in 14 (40%) eyes. Vitrectomy had been performed in 7 (20%) eyes before progression to NVG. The mean IOP of the 35 study eyes before IVB was 33.1±16.0 mmHg (range, 7–71 mmHg). The aqueous humor level of VEGF was higher in the 35 eyes before IVB (mean, 4,091 pg/mL; range, 426–48,400 pg/mL). The aqueous humor levels of VEGF were significantly correlated (r=0.535, P<0.001) (Fig. 1) with the baseline IOP.
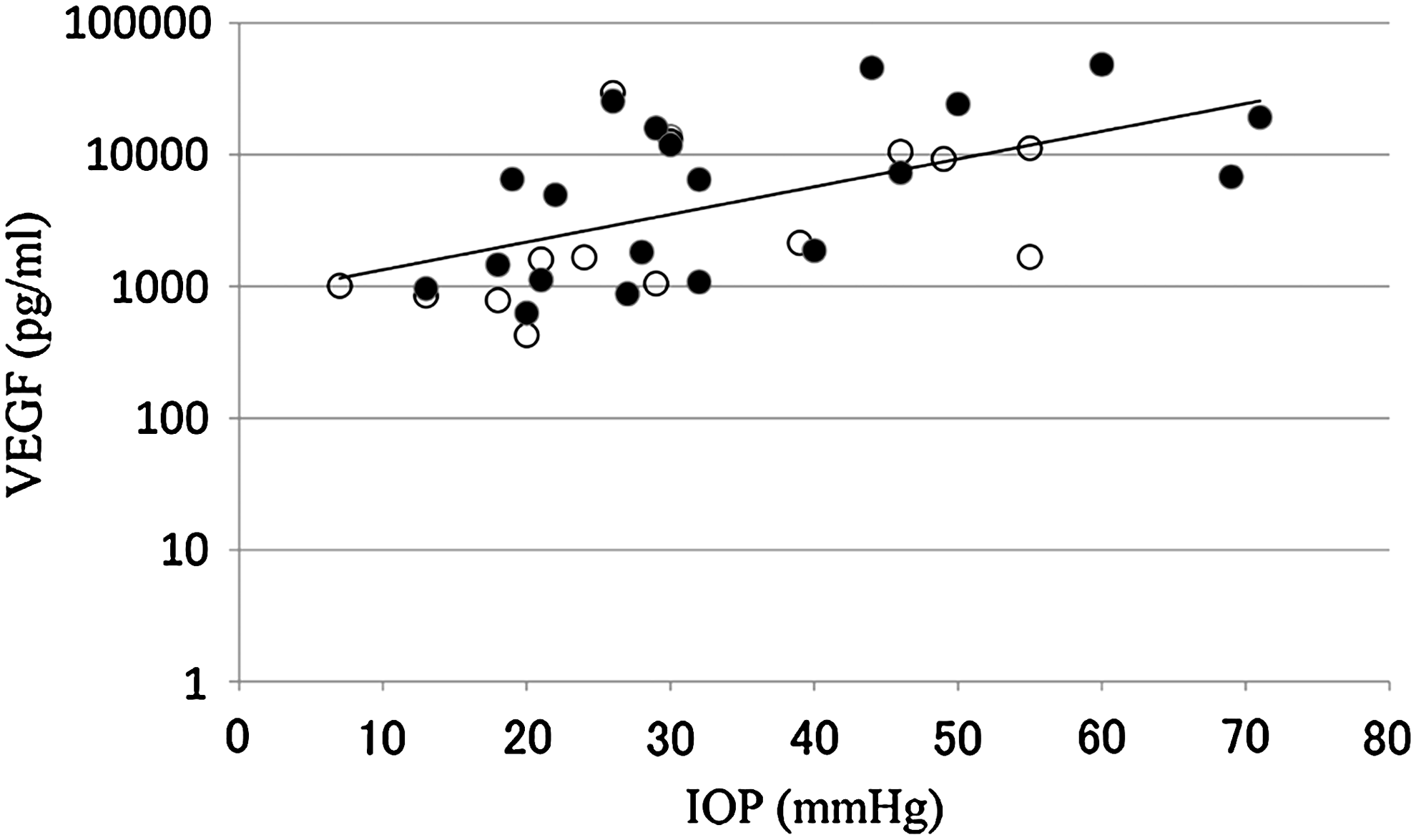
Relation between intraocular pressure (IOP) and aqueous humor levels of vascular endothelial growth factor (VEGF) in eyes with iris neovascularization and neovascular glaucoma (NVG) before intravitreal bevacizumab (IVB). The aqueous humor levels of VEGF are significantly (r=0.535, P<0.001) correlated with the IOP. Solid circles indicate the 1.0-mg group; open circles indicate the 0.1-mg group.
Of the 35 eyes, an IVB injection of 1.0 mg/40 μL was administered in 20 eyes (1.0-mg group) and 0.1 mg/40 μL in 15 eyes (0.1-mg group). The baseline profile and treatment results for each group are shown in Table 1. The mean aqueous humor concentration before the IVB injection was 5,136 pg/mL (range, 627–48,400 pg/mL) in the 1.0-mg group and 3,020 pg/mL (range, 426–29,400 pg/mL) in the 0.1-mg group. There was no significant difference between groups (P=0.212). One week after injection, marked regression or complete resolution of iris and angle neovascularization occurred in all study eyes regardless of the dose (Fig. 2). The mean IOP 1 week after injection significantly decreased to 25.9±14.3 mmHg (range, 12–60 mmHg) in the 1.0-mg group and 24.9±10.5 mmHg (range, 12–50 mmHg) in the 0.1-mg group compared with baseline (P<0.001 and P=0.001, respectively) (Fig. 3). Stepwise regression analysis showed that a larger decrease in IOP for 1 week was significantly correlated with higher baseline IOP and older age (P<0.001 and P<0.001, respectively). There were no significant differences in the impact on changes in the IOP between the 1.0- and 0.1-mg groups after adjusting the covariates detected by stepwise regression analysis (P=0.282). At 1 week, the IOP was within the normal range (≤21 mmHg) in 18 (51%) eyes: 11 eyes (55%) in the 1.0-mg group and 7 (47%) eyes in the 0.1-mg group without significant differences in IOP stabilization between groups (P=0.625).

Representative clinical findings of NVG treated with 0.1 mg IVB.
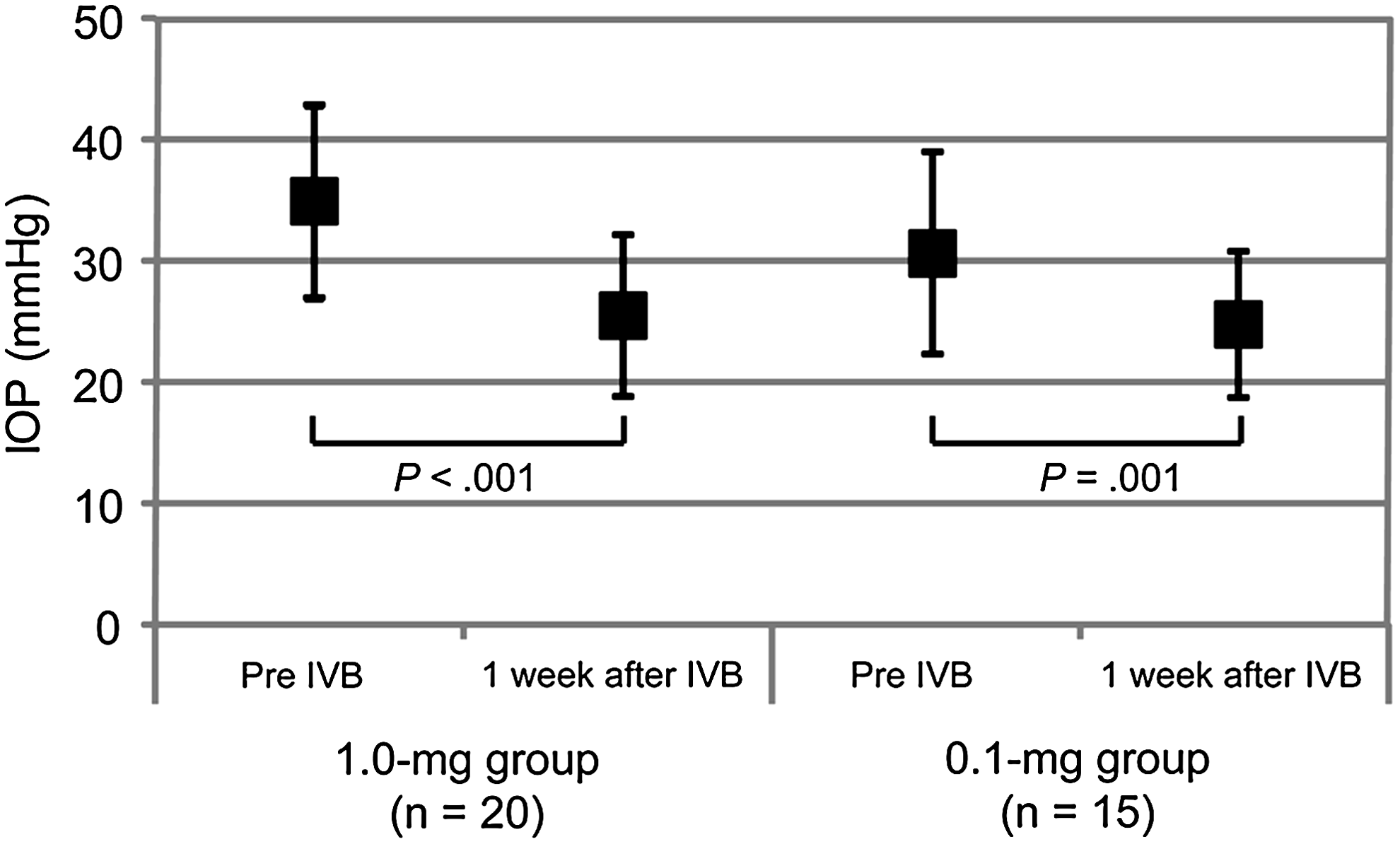
A graph shows the IOP (mean±95% confidence intervals) at baseline and 1 week after a 1.0-mg or 0.1-mg injection of IVB. The mean IOP significantly decreased after IVB in both groups.
Since there are 3 breakpoints along the disease continuum starting with INV and progressing through open-angle NVG to closed-angle NVG, 1 the study eyes were divided into 3 categories at the initial visit for IVB: eyes with iris and/or gonio-neovascularization without elevated IOP (≤21 mmHg, INV); eyes with IOP exceeding 21 mmHg with an open angle (O-NVG); and eyes with angle-closure glaucoma (C-NVG). Angle closure was defined as an angle closed 270° or more with formation of peripheral anterior synechiae; an open angle was defined as an angle open>90° according to the previous definition. 18
C-NVG, angle-closure neovascular glaucoma; F/M, female/male; SD, standard deviation; HM, hand motions; INV, iris neovascularization; IOP, intraocular pressure; IVB, intravitreal bevacizumab; logMAR, logarithm of minimum angle of resolution; LP, light perception; O-NVG, open-angle neovascular glaucoma; PPV, pars plana vitrectomy; PRP, panretinal photocoagulation; VA, visual acuity; VEGF, vascular endothelial growth factor.
Although the biologic effects of bevacizumab were maintained in 7 (20%) of 35 eyes 1 week after the initial injection, repeated injections of bevacizumab or surgeries were needed and performed with additional collection of aqueous humor samples in the other 28 eyes 1 week after initial IVB: 15 eyes (75%) in the 1.0-mg group and 13 eyes (87%) in the 0.1-mg group. The aqueous humor levels of VEGF in both subgroups significantly (P<0.001) decreased 1 week after the initial injection (Fig. 4). The mean VEGF concentrations in the aqueous humor significantly decreased to 25.5 pg/mL (range, <15.6–415 pg/mL) in the 15 eyes in the 1.0-mg group (P<0.001) and to 29.7 pg/mL (range, <15.6–169 pg/mL) in 13 eyes in the 0.1-mg group (P<0.001) compared with baseline in each group, thereby suggesting that the aqueous VEGF concentrations decreased by at least 100-fold in both groups. The mean changes in the aqueous humor VEGF concentrations did not differ between the 1.0-mg group and the 0.1-mg group (P=0.738). Seven (47%) of 15 eyes in the 1.0-mg group and 4 (31%) of 13 eyes in the 0.1-mg group had aqueous VEGF levels under the detectable level of 15.6 pg/mL 1 week after the injection. As expected, the mean changes in IOP and the rates of IOP stabilization (≤21 mmHg) in the 15 eyes of the 1.0-mg group and the 13 eyes in the 0.1-mg group did not differ significantly (P=0.718).
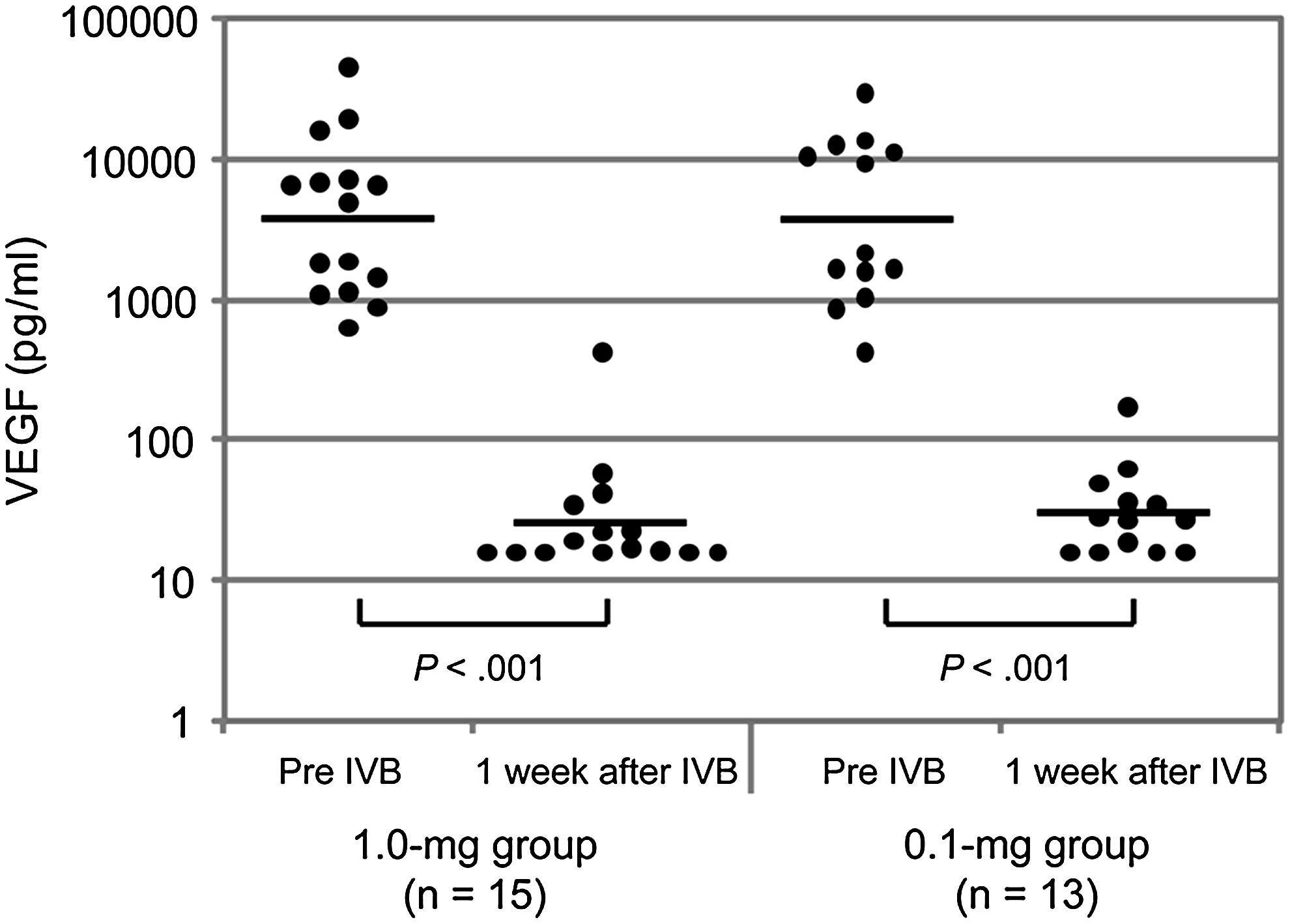
The graph shows VEGF levels in the aqueous humor at baseline and 1 week after injection of 1.0 mg or 0.1 mg of IVB. Each bar indicates the average value. The aqueous humor VEGF levels significantly decreased after IVB in both the 1.0-mg and 0.1-mg groups (P<0.001). However, the changes did not differ significantly between groups by at least 1 week after the injection (P=0.738).
During the 6-month follow-up of the study eyes, the IOP remained in the normal range in 25 eyes (83%); 16 eyes (84%) in the 1.0-mg group and 9 eyes (82%) in the 0.1-mg group, despite antiglaucoma medications (18 eyes, 60%), received repeated IVB injections (22 eyes, 73%) and/or antiglaucoma surgery (13 eyes, 43%). The mean IOPs at the 6-month examination significantly decreased to 18.3±6.6 mmHg in the 1.0-mg group (P<0.001) and to 14.5±6.3 mmHg in the 0.1-mg group (P<0.001) (Fig. 5). No significant difference in IOP stabilization was seen between groups (84% vs. 82%, P>0.99). The mean numbers of antiglaucoma medications at the 6-month follow-up visit were 1.4 (range, 0–5) in the 1.0-mg group and 1.2 (range, 0–3) in the 0.1-mg group (P=0.646). Although the numbers of surgeries did not differ significantly between the groups (0.9±0.8 in the 1.0-mg group vs. 1.0±1.3 in the 0.1-mg group) (P=0.898), the number of repeated injections in the 0.1-mg group tended to be higher than in the 1.0-mg group (1.7±0.9 vs. 0.84±0.96) but did not reach significance (P=0.073). The visual improvements overall and in each group measured at the 6-month follow-up are shown in Fig. 6. In the 1.0-mg group, the final VA improved in 7 eyes (37%), was unchanged in 7 eyes (37%), and deteriorated in 5 eyes (26%). In the 0.1-mg group, the final VA improved in 4 eyes (36%), remained unchanged in 6 eyes (55%), and deteriorated in one eye (9%). There were no significant differences in the visual changes between the groups (P=0.437). No eyes lost light perception throughout the follow-up period. No adverse systemic and local complications related to IVB were observed throughout the study in any study eyes including the 25 eyes (71%) that received repeated injections.
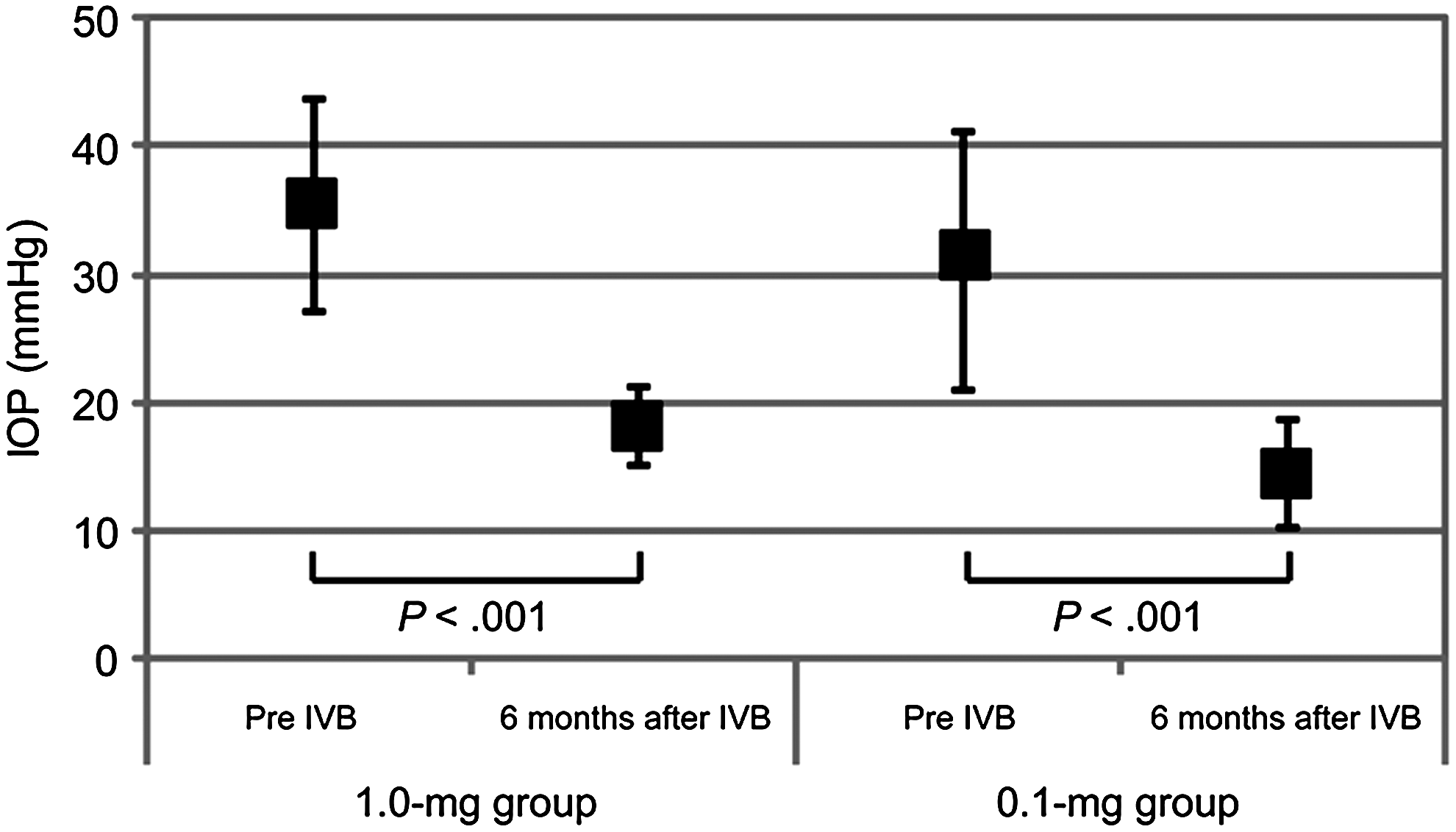
The graph shows the IOP (mean±95% confidence intervals) at baseline and 6 months after IVB in the 2 groups. The mean IOP at the 6-month examination has substantially decreased in both groups.
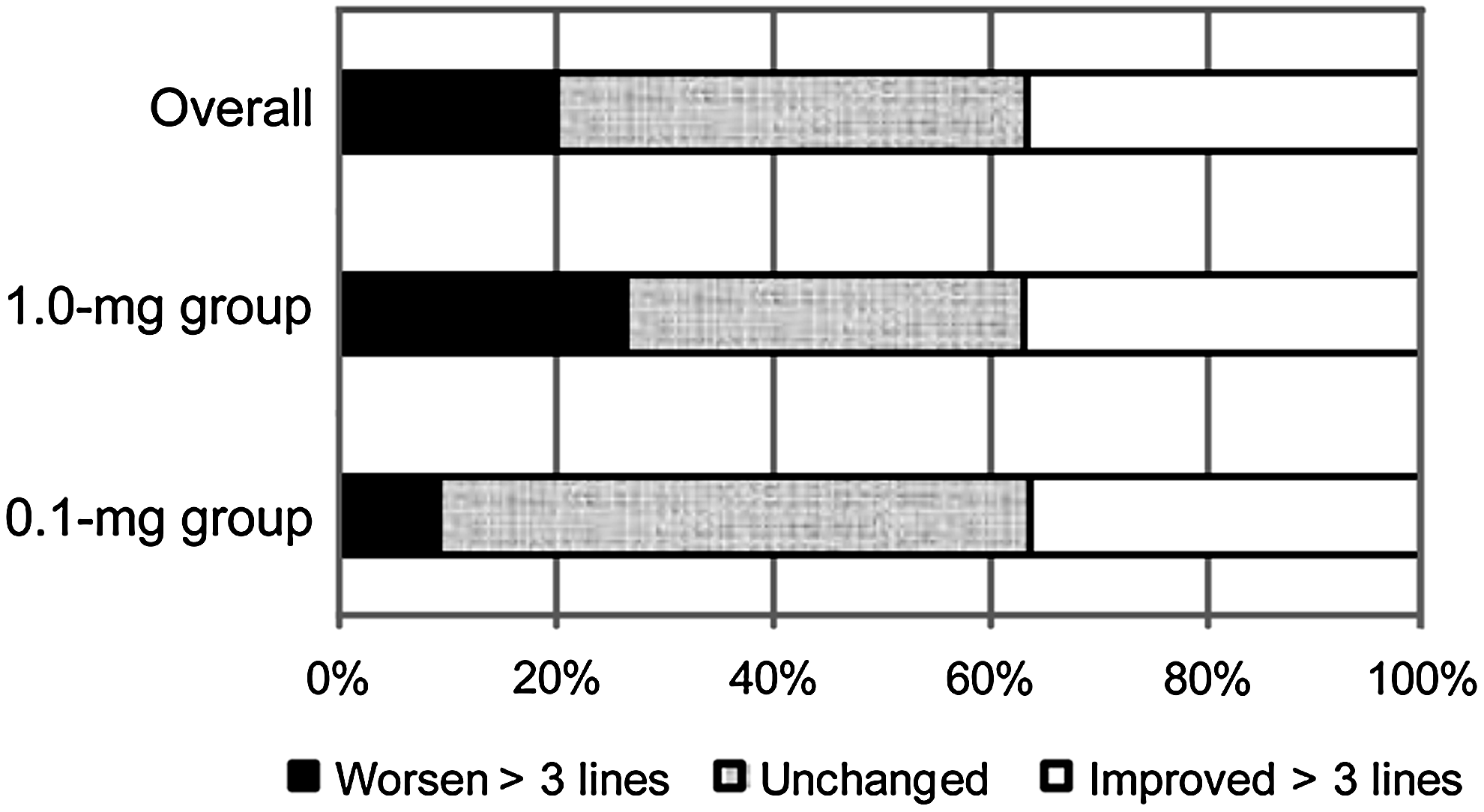
The bar graph shows the changes in the best-corrected visual acuity 6 months after IVB in the 1.0-mg group and the 0.1-mg group. Visual changes are defined as a change of 0.3 logarithm or more in the minimum angle of resolution unit.
Discussion
The current study is the first to report that the logarithmically transformed aqueous VEGF levels were highly significantly (r=0.535, P<0.001) correlated with the IOP. This finding may collaborate evidence suggesting that elevations of the aqueous VEGF levels and IOP may synergistically create a vicious cycle that results in progression of NVG, that is, the elevated VEGF promotes iris and angle neovascularization followed by fibrovascular membrane formation in the chamber angle to impede aqueous outflow leading to progressive angle closure and irreversible IOP elevation. The elevated IOP, in turn, may facilitate progression of circulatory disturbances with further exacerbation of ocular ischemia and consequent additional VEGF stimulation and secretion from the activated vascular endothelial cells, thus creating a vicious cycle of NVG progression. Therefore, reducing the elevated IOP and using anti-VEGF drugs to suppress the oversecreted VEGF are critical for preventing the negative spiral into progression of NVG.
The rapid and favorable biologic effect of bevacizumab for stabilizing intraocular neovascular activities has been reported in numerous studies,14–20 which encouraged us to consider bevacizumab as the first treatment of choice for NVG despite the off-label use. However, since the effect on regression of iris and angle neovascularization is transient because of the drug's short half life,35,36 flexible therapeutic strategies for using IVB to treat NVG have been recently proposed depending on the disease severity, that is, the use of repeated IVB injections with or without additional lazer treatment to facilitate resolution of anterior segment neovascularization and maintain stable IOP in the early stage of NVG with an open angle. 37 Otherwise, bevacizumab is recommended as a preoperative surgical adjunct to facilitate the safety and quality of antiglaucoma surgery for treating advanced NVG, because IVB alone is not effective for normalizing highly elevated IOP in eyes with angle closure.16,18,19 Although the intravitreal dose of 1.0 to 1.25 mg of bevacizumab is about 300- to 400-fold lower than the systemic dose, the risk of systemic adverse events such as thromboembolic events is still serious in elderly patients treated with intravitreal anti-VEGF therapy.16,38 In addition, over-suppression of VEGF to far below the physiologic level in eyes may increase the risk of retinal circulatory disturbances and visual impairment, particularly in patients with severe retinal ischemia.26,29 Given that patients with NVG often have high-risk backgrounds of retinal ischemia or thromboembolic events compared with patients with other retinal pathologies, decreasing the effective dosage of IVB to minimize or eliminate the risk of these side effects is desirable for patients with NVG. According to a previous study which suggested that a dose of bevacizumab as low as 6.2 μg resulted in regression of retinal neovascular activity in patients with diabetes, 13 we conducted a preliminary trial in a small number of consecutive patients with NVG to assess the biologic effect of 0.1 and 0.01 mg of IVB on iris and angle neovascularization. However, we failed to find any clinical effects with 0.01 mg for stabilizing both iris and angle neovascular activities (data not shown) in that preliminary trial, presumably because the intraocular VEGF levels in patients with NVG might be much higher than those without NVG.8,9,20 Therefore, we conducted the current pilot study to retrospectively compare the clinical and biologic effects of 0.1 mg IVB with the conventional dose of 1.0 mg.
In the current study, similar to the rapid biologic effects obtained in the 20 eyes that received the conventional 1.0-mg dose of IVB, we found that the lower 0.1-mg dose of IVB also achieved rapid and marked regression or complete resolution of iris and angle neovascularization in the 15 eyes with varying stages of NVG. The IOP was well controlled with regression of iris and angle neovascularization in eyes with early stage NVG 1 week after IVB, whereas additional surgeries or repeated injections were required in those with advanced NVG in both the 1.0- and 0.1-mg groups. The absence of significant differences in IOP control between the groups 1 week after IVB suggested that both doses may have equal clinical effects at least within 1 week after the initial injection. This finding is not surprising, because previous studies have suggested that IVB administered below the standard dosage may achieve rapid regression of retinal neovascularization in proliferative diabetic retinopathy.13,39 However, given that the aqueous VEGF levels in eyes with advanced NVG generally are much higher than in diabetic eyes without iris or angle neovascularization,8,9 we further investigated the biologic impact of 0.1 mg IVB on the reduction of aqueous VEGF concentrations. Due to the retrospective nature of the current study, we used generalized estimating equations to adjust the within-subject correlation and analyzed the data by using stepwise regression analysis with ANCOVA to minimize the effect of potential cofounders on the baseline parameters. Based on the VEGF data obtained from the aqueous humor samples before and after IVB in 28 eyes, we found that 1.0- and 0.1-mg doses of IVB are likely to achieve similar reductions in the VEGF concentrations in the aqueous humor at least by 1 week after the injection. Although the mean VEGF concentrations 1 week after IVB could not be precisely determined because of several cases with aqueous VEGF levels under the detectable limit, overall, the mean VEGF concentrations in the aqueous humor can be expected to decrease by at least 100-fold compared with the baseline level with both doses.
In addition to the favorable 1-week results with the lower dose of IVB, we followed the study eyes for >6 months after the initial injection to identify longer-term dose-dependent differences in anatomic and visual outcomes in eyes with NVG. During the follow-up, repeated injections of IVB and/or additional antiglaucoma surgery were often required in our series regardless of the dose. The mean IOP (18.3±6.6 mmHg vs. 14.5±6.3) and rate of IOP controllability (84% vs. 82%) at the 6-month examination did not differ significantly between the 2 doses. As in our previous study, 18 eyes with advanced NVG generally have a higher chance of requiring antiglaucoma surgery to stabilize the elevated IOP. However, the mean number of antiglaucoma medications (1.4 vs. 1.2) and surgeries (0.9 vs. 1.0) during the 6-month follow-up did not differ significantly between the 2 groups. The frequency of repeated injections was the only variable markedly higher in the 0.1-mg group with a borderline significance (P=0.073), thus suggesting that both iris and angle neovascularization, with or without re-elevations of IOP, may recur more often in eyes treated with the 0.1-mg injection. Nonetheless, the overall visual outcomes of the 19 eyes in the 1.0-mg group were similar to those of the 11 eyes in the 0.1-mg group, that is, the mean VA at the 6-month examination and the changes in VA from baseline did not differ significantly between the groups. Another noteworthy finding was that no eyes, even those with severely advanced NVG, lost vision or developed phthisis bulbi during the follow-up period in either group. These data taken together suggested that the 0.1-mg dose of IVB can achieve favorable anatomic and functional outcomes similar to those achieved with the 1.0-mg dose at least by 6 months after the initial injection, even though more frequent repeated injections and the same chance of the need for additional surgery were present with the lower dose compared with the conventional dose of 1.0 mg.
The current study had several limitations, that is, its retrospective nature, the absence of randomization, limited follow-up, a small number of patients in each group, and the different lengths of the study periods of the 1.0- and 0.1-mg groups. In addition, the aqueous humor samples could be collected only from eyes that required secondary interventions. Nevertheless, consecutive eyes treated with the same dose of bevacizumab during each of the 2 different periods can eliminate the bias in case selection. Although we did not encounter any systemic or local adverse events in either group during the study, dose-dependent adverse effects cannot be overlooked because of the difficulty in detecting infrequent events in a small number of cases. It is obvious that the lower dosage is more advisable to avoid untoward events if similar biologic effects can be obtained. Given that a recent study showed that recurrence of anterior segment neovascularization frequently occurs in advanced cases even with 1.25-mg of IVB and trabeculectomy after bevacizumab injection as the primary inhibitory factors for recurrence, 40 we believe that a decreased dose of 0.1 mg bevacizumab via intravitreal injection is at least sufficient as a surgical adjunctive treatment in eyes with advanced NVG, because it can stabilize neovascular activities preoperatively with minimal concerns about complications. In addition, although the interval between repeated injections is likely shorter with the 0.1-mg dose compared with the 1.0-mg dose, administering the lower dose of IVB initially might be recommended to confirm its clinical and biologic effects against both active neovascularization and ischemic retina, especially in high-risk patients. Since increasing the number of repeated injections will carry risks of infection, retinal detachment, and damage to the crystalline lens, development of an intraocular continuous-release drug delivery system for the optimal dose of bevacizumab should be an important topic for future research.
Considering that 31% of study eyes in the 0.1-mg group had aqueous VEGF levels under the detectable limit, a much lower dose of bevacizumab might be sufficient and desirable to treat NVG in selected cases. Customizing an optimal dose of IVB for treating NVG based on the aqueous VEGF concentration would be the most desirable regimen. Despite the semiquantitative nature and limited detection range of the immune-enzymatic assay that prevented us from obtaining exact VEGF concentrations in the aqueous humor in all study eyes, the significant positive correlation obtained in the current study strongly suggested that the aqueous VEGF levels in eyes with NVG can be estimated by measuring the IOP. Further studies with more patient data to establish an accurate empiric formula may be helpful in estimating the VEGF concentration in the aqueous humor based on IOP levels, with the goal of customizing the optimal dose of IVB for individual cases of NVG.
In conclusion, the current data showed for the first time that the aqueous humor levels of VEGF were significantly correlated with the IOP in patients with NVG. Similar clinical and biologic effects of 0.1-mg IVB compared with the conventional dose of 1.0 mg for decreasing the elevated levels of VEGF in the aqueous humor with rapid involution of iris and angle neovascularization at least in the short term suggested that 0.1 mg of bevacizumab may be more desirable and safer for use as a surgical adjunctive therapy for treating NVG in high-risk patients.
Footnotes
Acknowledgment
The current study is supported in part by a Research Grant from the Ministry of Education, Science, and Culture, Tokyo, Japan.
Author Disclosure Statement
The authors have no proprietary interest in any materials discussed in this article.