
Abstract
Abstract
Purpose:
To assess side differences in patients undergoing bilateral intravitreal bevacizumab injections as treatment of exudative age-related macular degeneration (AMD).
Methods:
The clinical interventional case series study included 48 patients (96 eyes) who consecutively and bilaterally received 3 intravitreal bevacizumab injections. The mean age was 76.5±7.5 years (range: 59–88 years). Follow-up was 6 months. Main outcome parameters were best-corrected visual acuity (BCVA) and measurements by optic coherence tomography. The eyes of the same patient were assigned to a study group 1 for the eye with the higher visual acuity at baseline, and study group 2 for the contralateral eye with the lower visual acuity at baseline.
Results:
The increase in BCVA was significantly (P=0.02) greater in group 2 (0.07±0.25 logarithm of the minimum angle of resolution, LogMAR) than in group 1 (0.05±0.29 LogMAR). The height of a detached retinal pigment epithelium, the height of subretinal fluid, and the tissue thickness of the macula decreased significantly (P<0.05) in group 2 during follow-up, whereas these parameters did not markedly change in the eyes of group 1 (P=0.96, P=0.38, and P=0.07, respectively). The reduction in the height of a detached retinal pigment epithelium and in the height of subretinal fluid was significantly more pronounced in group 2 than in group 1 (P=0.03, P=0.04, respectively).
Conclusions:
After an initial set of 3 bilateral bevacizumab injections, patients with bilateral exudative AMD have a higher likelihood for an improvement in vision in the worse-seeing eye at baseline than in the better-seeing eye.
Introduction
Methods
This retrospective interventional case series included 48 patients (96 eyes) who consecutively received 3 intravitreal injections of bevacizumab for treatment of exudative AMD in both eyes. Exclusion criteria were the presence of any other retinal diseases, such as diabetic retinopathy or retinal vascular occlusions; a side difference in the lens status between the right eye and the left eye (i.e., both eyes had to be either phakic or both eyes had to be pseudophakic); and a history of a previous treatment of choroidal neovascularization, such as intravitreal triamcinolone injections or photodynamic therapy. All patients were fully informed about the experimental character of the therapy, and all patients signed an informed consent. The present study was a retrospective analysis of the clinical data that were obtained while routinely taking care of the patients.
At baseline, all patients underwent an ophthalmological examination including refractometry, best-corrected visual acuity (BCVA), applanation tonometry, ophthalmoscopy, fluorescein angiography, and optical coherence tomography (OCT). On the optical coherence tomograms (Stratus OCT™; Macular Thickness Analysis program; Carl Zeiss Meditec AG, Jena, Germany), we measured the highest elevation of a detached retinal pigment epithelium, the greatest height of subretinal fluid, and the highest thickness of the macular retinal tissue. According to the visual acuity at baseline of the study, the eyes of the same patient were divided into 2 groups: group 1, the eye with the higher visual acuity; and group 2, the contralateral eye with the lower visual acuity. If the measured visual acuity of both eyes was equal, the eye with a longer history of visual deterioration was included into group 2.
The injection method was recently described in detail. 11 Briefly, before the injection, topical anesthesia was applied, and the patients were completely draped as for any intraocular surgery. A lid speculum was inserted. In the temporal inferior region, 1.5 mg bevacizumab was injected with a sharp 27-gauge needle trans-conjunctivally at 3–3.5 mm from the limbus. After that, an antibiotic ointment (polymyxin and neomycine) was applied, and the eyes were patched for at least 3 h. The worse-seeing eye was usually injected first, unless the better-seeing eye had experienced a more rapid recent deterioration in visual acuity. The time interval between the injections of both eyes was at least 1 week. Three consecutive injections of bevacizumab were performed at intervals of 6–8 weeks. Within 1–3 days after each injection, the patients were controlled by the referring ophthalmologists to rule out an injection-related infection or sterile inflammation. After the third injection, the patients usually re-visited their ophthalmologists in monthly intervals before they re-appeared in the hospital at about 2–3 months after the last injection for the follow-up examination. The latter included an optical coherence tomographic imaging of the macula. During the follow-up, no additional ocular surgery including cataract surgery was carried out.
Statistical analysis was performed using a commercially available statistical software package (SPSS for Windows, version 17.0; SPSS, Chicago, IL). Measurements of BCVA were converted into the logarithm of the minimum angle of resolution (LogMAR) for statistical calculation. The data that were normally distributed were presented as the mean±standard deviation. Where appropriate, the Student's t-test for paired samples and Chi-square test were used. All P values were 2-sided and were considered statistically significant when the values were <0.05.
Results
The study group included 48 patients (31 women, 65%; 96 eyes) with a mean age of 76.5±7.5 years (range: 59–88 years). There were 24 patients with bilateral phakic eyes (50%) and 24 patients with bilateral pseudophakic eyes. The ophthalmic data of either group are presented in Table 1. Due to the selection criteria, BCVA was significantly better (P<0.001) in group 1 than in group 2; whereas all other parameters data did not differ significantly (P>0.05) between the 2 groups (Table 1).
BCVA, best-corrected visual acuity; IOP, intraocular pressure; CNV, choroidal neovascularization; LogMAR, logarithm of the minimum angle of resolution; RPE, retinal pigment epithelium; group 1, eyes with higher BCVA at baseline; group 2, contralateral eyes with lower BCVA at baseline.
At 3 months after last of the 3 intravitreal injections, BCVA of all eyes together had not changed significantly as compared with the baseline values (from 0.66±0.42 logMAR to 0.64±0.44 logMAR; P=0.68). Dividing the whole study population into group 1 and group 2 revealed that the eyes of group 2 experienced an increase in BCVA (0.07±0.25 LogMAR), whereas the eyes of group 1 lost in BCVA (0.05±0.29 LogMAR), with a significant difference in the change in BCVA between both groups (P=0.02) (Table 2 and Fig. 1).
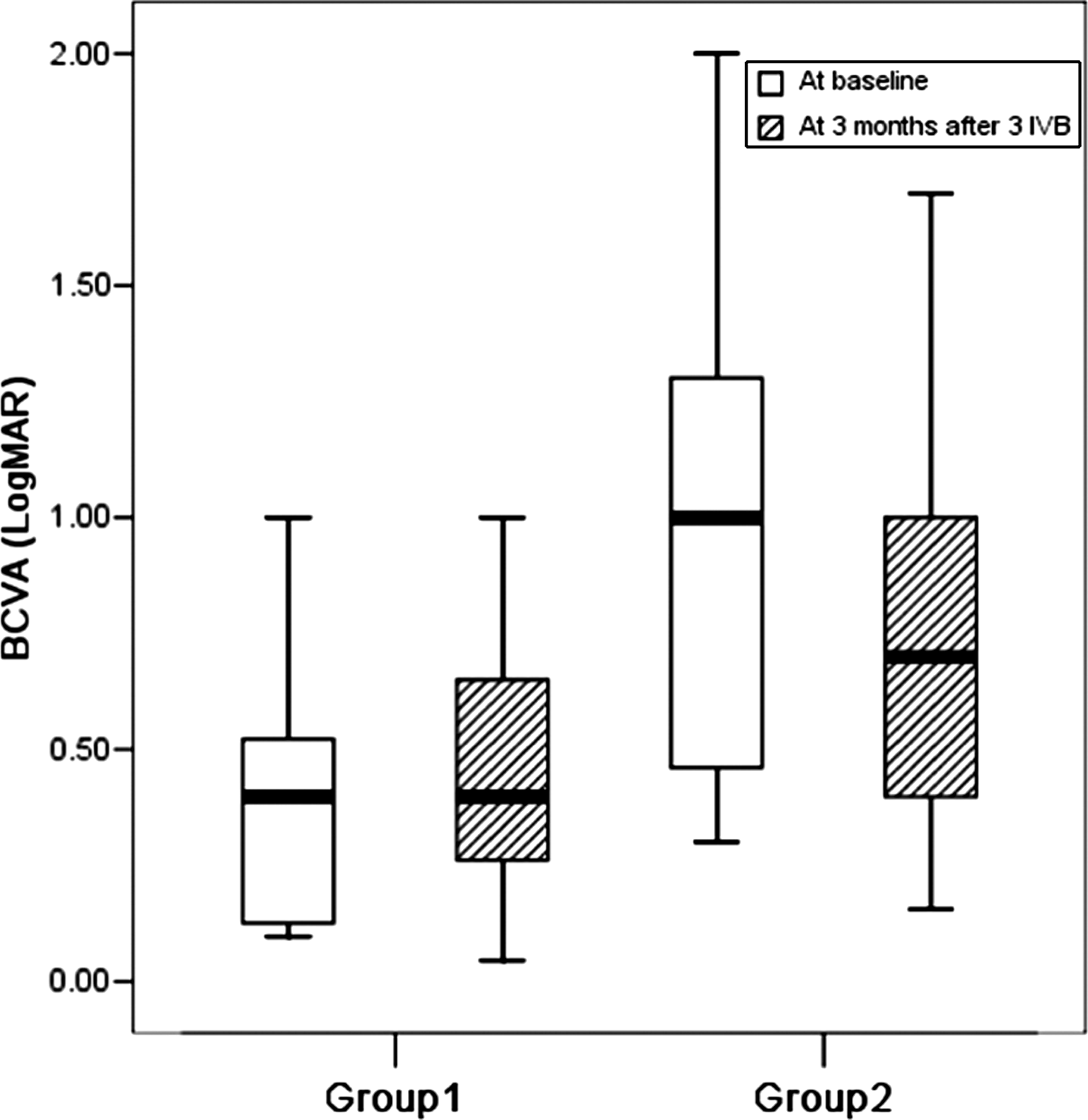
Box plots showing the distribution of best-corrected visual acuity (BCVA) in patients with bilateral intravitreal injections of bevacizumab as therapy of exudative age-related macular degeneration, at baseline and at 3 months after 3 intravitreal injections; group 1, eyes with higher BCVA at baseline; group 2, contralateral eyes with lower BCVA at baseline. The bottom and top of the boxes represent the 25th and 75th percentile or the lower and upper quartiles, respectively; the band near the middle of the box is the 50th percentile or median; the ends of the whiskers indicate the 1.5-fold interquartile range; the circles represent mild outliers (within 1.5- to 3.0-fold of the interquartile range); and the asterisk represents an extreme outlier (outside of 3.0-fold of the interquartile range).
After continuity correction.
The percentage of eyes with an increase in BCVA of ≥1 line, ≥2 lines or ≥3 lines was higher, however not significantly (P>0.05; Chi-square test) higher, in group 2 than in group 1 (46% vs. 31%, 33% vs. 21%, and 19% vs. 4%, respectively) (Table 2) and the percentage of eyes with a loss in BCVA of ≥1 line, ≥2 lines or ≥3 lines was lower in group 2 than in group 1 (21% vs. 27%, 11% vs. 19%, and 8% vs. 17%; respectively) (Table 2).
As a corollary, the height of a detached retinal pigment epithelium, the height of subretinal fluid, and the tissue thickness of the macula decreased significantly (P<0.05) in group 2 during follow-up; whereas these parameters did not markedly change in the eyes of group 1 (P=0.96, P=0.38 and P=0.07, respectively) (Table 3). The reduction in the height of a detached retinal pigment epithelium and in the height of subretinal fluid was significantly more pronounced in group 2 than in group 1 (−2±109vs. 92±273 μm; P=0.03; 8±58 vs. 51±117 μm; P=0.04) (Fig. 2). The reduction of highest retinal thickness of macula of group 2 was slightly higher than in group 1 (−24±94 vs. 37±91 μm), but it was not statistically significant (P=0.44, Fig. 2).
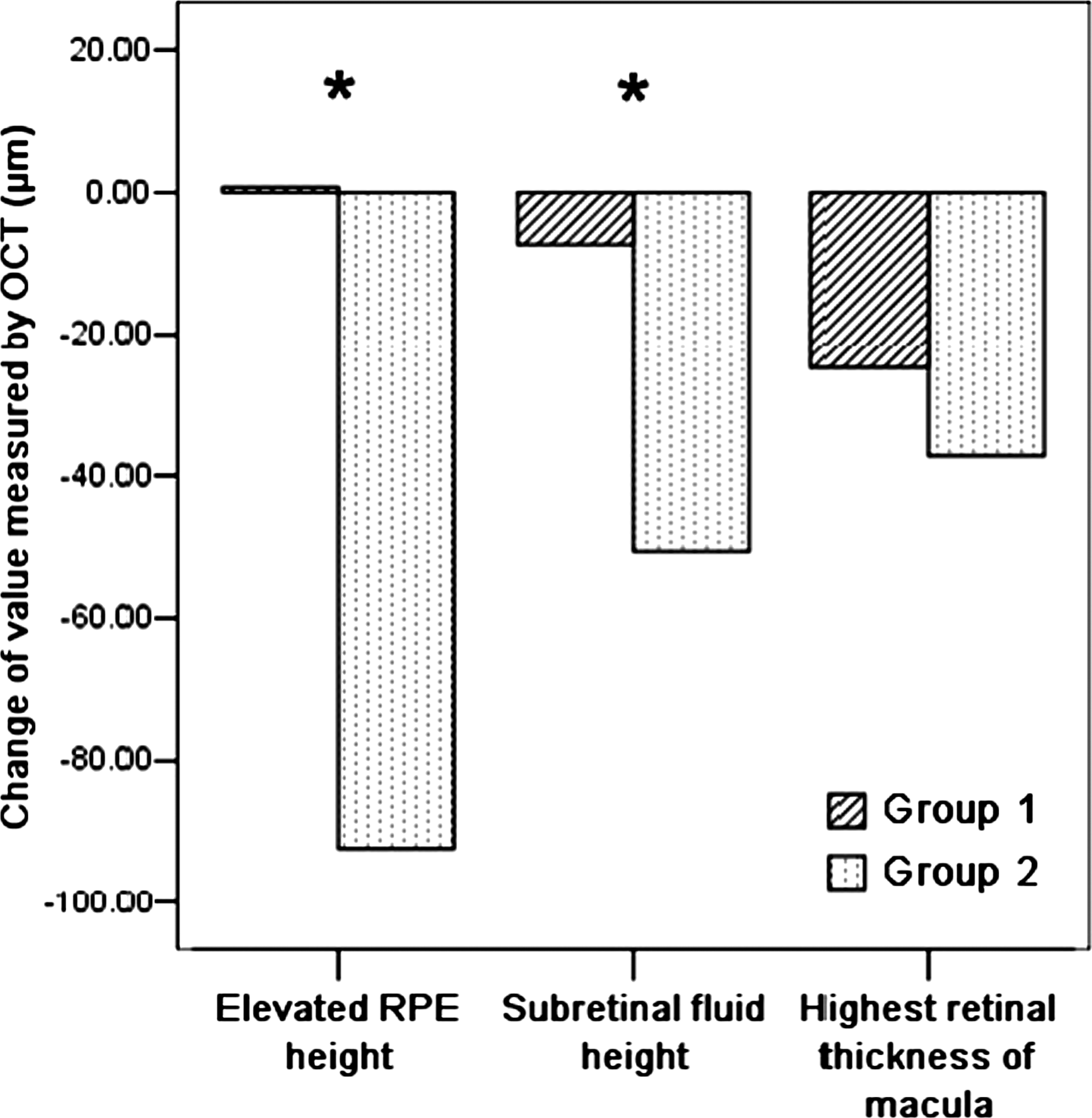
Cluster bars showing changes in the height of a detached retinal pigment epithelium (RPE), height of subretinal fluid, and tissue thickness of the macula in patients with bilateral intravitreal injections of bevacizumab as therapy of exudative age-related macular degeneration, at baseline and at 3 months after 3 intravitreal injections. *P<0.05.
P value, statistical significance of the difference between both groups.
The intraocular pressure did not differ significantly between baseline and any follow-up examination in any group (group 1: 14.8±2.6 vs. 14.8±2.6; P=0.89, group 2: 15.3±2.8 vs. 15.0±2.2; P=0.54).
Discussion
The results of our study demonstrated that in patients with bilateral exudative AMD the eye with the worse vision at baseline had a better prognosis for a gain in visual acuity than the contralateral eyes with the higher visual acuity at baseline. This result may be clinically important for counseling of patients, that despite treatment with intravitreal bevacizumab injections, visual acuity may deteriorate in the better eye as compared with the contralateral eye with a worse baseline vision.
The results of our study might have been anticipated, as it is easier to lose if one starts at a high level, and it is easier to gain if one starts at a low level. The same accounts for morphological changes in the macula for which an improvement is easier to be detected if there is a marked degree of abnormality than as if there are only subtle changes at baseline. Correspondingly, previous studies on the potential benefit of intravitreal triamcinolone for therapy of exudative AMD showed that the increase in visual acuity was significantly (P<0.001) and negatively correlated with preoperative visual acuity.12–14
The finding of a significant improvement in BCVA after intravitreal injections of bevacizumab agrees with numerous several previous reports.15–19 It is also in agreement with large randomized clinical trials on the effect of another antivascular endothelial growth factor, ranibizumab. 20
Potential limitations of our study should be mentioned. First, the study design did not include a control group. It can, therefore, not be concluded that the intravitreal injection of bevacizumab in the eyes with a higher BCVA at baseline is not associated with a therapeutically positive effect. Second, it is a retrospective data analysis with all limitations of such a study design. All patients, however, had routinely received optical coherence tomographic examination, and the patients were consecutively included into the study. Third, the follow-up was relatively short, so that no statements can be made about the long-term prognosis. Strength of the study is its design as an intraindividual intereye comparison, so that systemic factors such as age, gender, smoking history, alcohol consumption, and genotype did not influence the results of the study and its conclusion. Fourth, the worse-seeing eye was usually the one which received the first injection, so that the better-seeing eye received the therapy at a later time point. This might have had a disadvantage for the better-seeing eye, as the disease might have progressed in the meantime. Since, however, baseline visual acuity was measured at the day of injection, deterioration in visual acuity that may have occurred in the interval between the injections in both eyes would have fully been covered in the statistical analysis. Another disadvantage for the better-seeing eye may have been tachyphylaxis induced by the injection into the contralatreal eye. Clinically significant tachyphylaxis over a short period, however, has not yet been described for the therapy with intravitreal bevacizumab.21,22 Fifth, since a time domain OCT was used, the follow-up measurements of the macular changes were less reliable than as if a spectral domain OCT had been available. This weakness of the study design held true for both study groups, however, so that it may not have markedly influenced the results and conclusions of the study.
In conclusion, patients after 3 bilateral intravitreal injections of bevacizumab as therapy of bilateral exudative AMD have a higher likelihood for an improvement in vision in the worse-seeing eye at baseline than in the better-seeing eye. This conclusion, however, should not lead to a delay in the treatment of the better-seeing eye, as the therapeutic efficacy of the intravitreal anti-vascular endothelial growth has been proved.2–19
Footnotes
Acknowledgment
The work of Yong Tao was supported by K.C.Wong Fellowship from the German Academic Exchange Service (DAAD).
Author Disclosure Statement
No competing financial interests exist.