
Abstract
Abstract
Purpose:
The purpose of this study was to investigate the effectiveness of intravitreal bevacizumab injections combined with tunable argon yellow laser photocoagulation as a treatment for adult-onset Coats' disease.
Methods:
We consecutively treated 3 patients suffering from Coats' disease diagnosed in adulthood with a combination of intravitreal bevacizumab injection and tunable argon yellow laser photocoagulation. All patients received an intravitreal injection of 2.5 mg bevacizumab together with various sessions of laser photocoagulation targeting the area of telangiectasia. The patients' best-corrected visual acuities were recorded. Fundus photography, fluorescein angiography (FA), and optical coherence tomography were used to monitor vascular and retinal exudate changes.
Results:
Fundus photography and FA of all 3 patients revealed significant regression of the vascular dilatation and the aneurysmal appearance of the telangiectasia areas. Optical coherence tomography also showed a significant subsidence of the macular edema and submacular fluid in all patients. A concomitant improvement in visual acuity was also noted. No treatment-related complications were identified.
Conclusions:
Combining intravitreal bevacizumab and tunable argon yellow laser photocoagulation is an efficient treatment of choice for Coats' disease that has been diagnosed in adulthood.
Introduction
The main pathogenic mechanism of Coats' disease includes loss of endothelium and pericytes and breakdown of the blood–retinal barrier, which result in progressive weakening of the endothelial lining and the vascular wall structure. This leads to dilative vascular abnormalities and exudative retinopathy. 1 Although the pathogenesis remains largely unknown, recent evidence has suggested that it may be associated with an increased ocular level of the vascular endothelial growth factor (VEGF).4,5 This finding raises the possibility of using an anti-VEGF therapy to treat Coats' disease. Several reports have suggested that intravitreal injection of bevacizumab, a full-strength anti-VEGF antibody, may be an effective way of ameliorating the exudative complication of Coats' disease in children.4–12
Although Coats' disease can be recognized at any age, most patients are diagnosed during their first 2 decades of life.1,2 Only on rare occasions is Coats' disease initially diagnosed in adulthood.1,2 Coats' disease in adults seems to progress at a slower rate than in children; however, treatment is often necessary when the retinal exudation involves or threatens the macula area.13,14 Laser photocoagulation is one of the most frequently chosen methods for obliteration of the abnormal vessels in adult Coats' disease. However, the absorption of the exudative reaction is often very slow and the extent of the subretinal fluid (SRF) may preclude the effective obliteration of the abnormal vessels.13,14 As intravitreal anti-VEGF has been shown to be effective at reduction and also helps with the more rapid absorption of the exudates in children, it may also be effective when used to treat adult Coats' disease. Very few studies have been published describing the use of intravitreal bevacizumab or any other anti-VEGF agents to treat adult Coats' disease.15,16 In this case series, we conducted a treatment protocol that combined intravitreal bevacizumab and laser photocoagulation. It involved 3 consecutive patients with adult Coats' disease. The favorable results suggest that intravitreal bevacizumab may be a useful adjunctive treatment to the use of laser photocoagulation for the treatment of adult Coats' disease.
Case Reports
Three eyes of 3 patients (all aged over 18 years) with Coats' disease were diagnosed at Shin-Kong Wu Ho-Su Memorial Hospital in Taiwan. All patients signed a written informed consent. The correlation of patient data for this report was approved by the institutional review board of our hospital.
Case 1
Case 1 was a 21-year-old man who denied having any systemic diseases. He visited our Ophthalmology Department in June 2008 with his chief complaint being a sudden onset of painless blurred vision in his right eye (OD) for 1 month. The best-corrected visual acuity (BCVA) was 6/15 (OD) and the intraocular pressure (IOP) was 11 mmHg (OD). A fundus examination showed convoluted telangiectasia with aneurysmal dilatation of the temporal equatorial area with a focal intraretinal hemorrhage around the dilated vasculature. Macular SRF and lipid exudates (OD) were also noted (Fig. 1A, C). Fluorescein angiography (FA) revealed the presence of areas of nonperfusion and aneurysmal dilatation of the telangiectasia with some leakage at this early phase (Fig. 1B). Marked thickening of the central retinal thickness (CRT) was noted in his right eye by optical coherence tomography (OCT) (OD: 467 μm; OS: 235 μm). The patient received 2 monthly intravitreal bevacizumab (Avastin; Genentech, San Francisco, CA) injections (2.5 mg/0.1 mL) in his right eye. One month later, tunable argon yellow laser photocoagulation (Novus Omni; Coherent Medical Laser, Palo Alto, CA) was applied to the abnormal vasculature and the area with hard exudates. The macular edema and SRF were obviously resolved after the treatment and the CRT was found to have decreased to 230 μm (OD) (Fig. 1F). Ophthalmoscopic examination showed a resolution of the lipid exudate (Fig. 1D) and FA showed regression of the telangiectasia and an obvious decrease in dye leakage (Fig. 1E). The BCVA improved to 6/6.7 and has remained the same for the 2 years since treatment. No progression of the lesions has been noted during these 2 years.
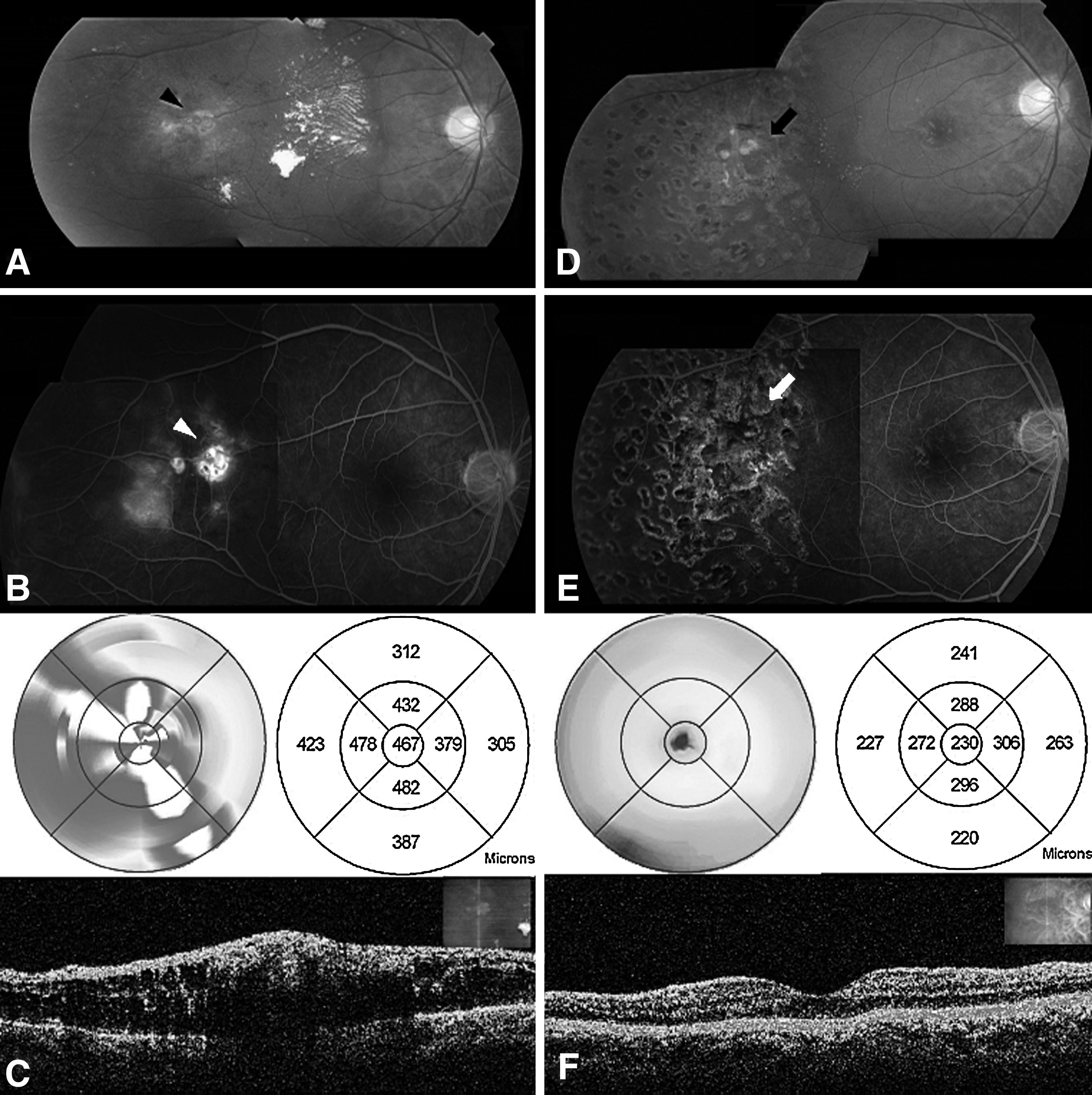
Case 1. The best-corrected visual acuity improved from 6/15 to 6/6.7 (OD) after treatment.
Case 2
Case 2 was a male patient who was diagnosed as suffering from Coats' disease at an age of 51 years in July 2009. Argon laser photocoagulation was applied at the beginning to treat telangiectasia and lipid exudation. The telangiectasia diminished after the treatment. However, recurrence was noted 1 year later. A fundus examination at this time revealed more telangiectatic vessels with prominent retinal hemorrhage and progressive massive lipid exudation (Fig. 2A). FA revealed multiple leakages from the aneurismal telangiectasia and nonperfusion areas (Fig. 2B). Two courses of intravitreal bevacizumab (2.5 mg/0.1 mL) injections combined with tunable argon yellow laser photocoagulation applied to the nonperfusion and telangiectasia areas were carried out. The subsequent ophthalmoscopic examinations showed an obvious decrease in the size and amount of telangiectasia (Fig. 2D) and FA showed a significant decreased in the leakage from aneurismal telangiectasia (Fig. 2E). There was also a significant decrease in SRF on OCT (Fig. 2C, F). The BCVA improved from 6/12 to 6/6 and remained so during the 6 months of follow-up.

Case 3
The third case was a 68-year-old man who visited our clinic in March 2010 with his chief complaint being progressive blurred vision of his left eye (OS) for 1 year. Central metamorphopsia was also noted. His initial BCVA was 5/60 (OS), and the IOP was 10 mmHg (OS). A fundus examination revealed convoluted telangiectasia in the parafoveal area with retinal hemorrhage and circinate hard exudate (OS) (Fig. 3A). FA revealed multiple leakages from the telangiectasia and areas of capillary nonperfusion (Fig. 3B). Macular edema with increased CRT of his left eye was also noted on OCT (OD: 214 μm; OS: 412 μm) (Fig. 3C). He received 2 courses of intravitreal injections of bevacizumab (2.5 mg/0.1 mL) combined with tunable argon yellow laser photocoagulation. The latter was applied to areas of telangiectasia in his left eye. Subsequent ophthalmoscopic examinations revealed regression of the retinal telangiectasia accompanied by a decrease in exudation (Fig. 3D). FA revealed decreased fluorescein leakage (Fig. 3E). OCT also showed decreased macular edema (OS: 330 μm) after the treatment (Fig. 3F). The BCVA improved from 6/60 to 6/20 and remained the same for over 1 year.

Discussion
Except for the fact that they were diagnosed during adulthood, the present cases have the typical manifestations of Coats' disease, which include unilateral involvement in a male patient with vascular telangiectasia, lipid exudation, microaneurysms and macroaneurysms, macular edema, areas of capillary nonperfusion with adjacent webs of filigree-like capillaries, and an absence of retinal neovascularization.1,2 In contrast to typical Coats' disease in childhood, Smithen and colleagues have reported that adult Coats' disease often shows several distinct and characteristic morphological findings. 14 In typical childhood-onset Coats' disease, the vascular abnormalities are often in the far periphery, between the equator and the ora serrata. This contrasts with adult patients, in whom the vascular abnormalities more frequently involve the juxtamacular region. In addition, lipid deposition, frequently massive and diffuse in children, is usually localized and limited in the adult group. Hemorrhage, which is less common in typical Coats' disease among young patients, occurs in many adult patients, with the bleeding localized to the macroaneurysms. All 3 of these characteristics were present in our cases (Figs. 4).

All of our cases had the characteristic morphological findings associated with adult Coats' disease.
Retinal cryotherapy and laser photocoagulation are the most frequently applied treatments for the ablation of abnormal vessels in Coats' disease. Cryotherapy is useful in peripheral telangiectasia associated with extensive exudation or subtotal retinal detachment, which is a common feature associated with childhood-onset Coats' disease. However, it often induces significant inflammation and does not improve vision effectively. 17 For adult-onset Coats' disease, aggressive treatment with cryotherapy is often difficult and unnecessary, because the distribution of abnormal vessels is usually not very peripheral and the exudative reaction is less extensive. Laser photocoagulation, on the other hand, is much less destructive than cryotherapy. Repeated laser photocoagulation of telangiectatic vessels and areas of exudative retinal detachment should be able to achieve globe salvage and retain useful vision. 18 However, this treatment may still break down the blood–retinal barrier and transiently increase the hard exudates of the vitreoretinal traction.7,11 In addition, the application of laser treatment effectively needs the retina to be flat or minimally elevated, a condition that is not always available in patients with Coats' disease on presentation. 3 Therefore, adjunct therapy to facilitate laser photocoagulation and make it more effective would seem to be the treatment of choice.
The effect of intravitreal bevacizumab on the absorption of macular edema and submacular fluid is clearly demonstrated by the pre- and post-treatment OCT findings in our cases 1 and 3 (Figs. 1 and 3). This supports recent findings that VEGF play a role in the pathogenesis of the abnormal vessel formation in Coats' disease and that intravitreal injection of anti-VEGF may be an effective way of achieving resolution of macular edema and exudative reaction.4,5 Sun et al. 4 found an elevated vitreous VEGF level in a 2-year-old boy with stage-4 Coats' disease, and the application of pegatinib (an anti-VEGF that inhibits mainly an VEGF isomer with 165 amino acids) resulted in a marked resolution of the exudative reaction and the serous retinal detachment. He et al. 5 found elevated VEGF levels in the subretinal fluid or aqueous humor of 4 patients with Coats' disease, and intravitreal injection of bevacizumab resulted in a resolution of the macular edema and an improvement in visual acuity in 1 patient. There have been several other case reports describing the application of intravitreal injections of anti-VEGF agent to treat Coats' disease and most of which have had favorable outcomes in which there was a reduction in subretinal lipid exudation and exudative retinal detachment.6–12 Other agents, such as intravitreal triamcinolone, may also have a similar effect.15,19–21
Subsequent laser photocoagulation is often necessary to achieve ablation of the abnormal vessels and to prevent a recurrence of exudative reaction. 9 We used a tunable argon yellow laser for the ablation of the telangiectatic vessels in our 3 cases. Yellow laser light has been used to treat Coats' disease with successful long-term results. 22 Yellow laser light has the property of selective absorption by hemoglobin. When applied to the photocoagulation of dilated vessels, this allows direct uptake by the vessels themselves and allows ablation to be achieved without uptake by the retinal pigment epithelium. This is a particular advantage when there is SRF underlying the targeted vessels, a condition frequently encountered in Coats' disease. 22 Using anti-VEGF injections as a pretreatment to decrease the retinal edema and exudation may also decrease the laser energy necessary for the ablation of the abnormal vessels and this will facilitate the efficacy of the laser treatment. As the telangiectatic vessels in adult-onset Coats' disease are often localized near the macular area, minimizing the laser energy is important to avoid the aggravation of the macular exudation or inadvertent macular damage.
In summary, our cases have indicated that anti-VEGF treatment combined with laser photocoagulation is effective not only in typical childhood Coats' disease, but also in the adult-onset variant of the disease. Appropriate treatment that combines laser photocoagulation with intravitreal bevacizumab should be able to achieve better results in terms of both the eradication of telangiectatic vessels and the regression of retinal exudation.
Footnotes
Author Disclosure Statement
The authors have no financial or proprietary interest in any product mentioned in this article.